
Abstract
Abstract
Background:
Current in vitro approaches to assess lung deposition, dissolution, and cellular transport behavior of orally inhaled products (OIPs) have relied on compendial impactors to collect drug particles that are likely to deposit in the airway; however, the main drawback with this approach is that these impactors do not reflect the airway and may not necessarily represent drug deposition behavior in vivo. The aim of this article is to describe the development and method validation of a novel hybrid in vitro approach to assess drug deposition and permeation behavior in a more representative airway model.
Methods:
The medium-sized Virginia Commonwealth University (VCU) mouth–throat (MT) and tracheal–bronchial (TB) realistic upper airway models were used in this study as representative models of the upper airway. The TB model was modified to accommodate two Snapwell® inserts above the first TB airway bifurcation region to collect deposited nebulized ciprofloxacin–hydrochloride (CIP-HCL) droplets as a model drug aerosol system. Permeation characteristics of deposited nebulized CIP-HCL droplets were assessed across different synthetic membranes using the Snapwell test system.
Results:
The Snapwell test system demonstrated reproducible and discriminatory drug permeation profiles for already dissolved and nebulized CIP-HCL droplets through a range of synthetic permeable membranes under different test conditions. The rate and extent of drug permeation depended on the permeable membrane material used, presence of a stirrer in the receptor compartment, and, most importantly, the drug collection method.
Conclusions:
This novel hybrid in vitro approach, which incorporates a modified version of a realistic upper airway model, coupled with the Snapwell test system holds great potential to evaluate postairway deposition characteristics, such as drug permeation and particle dissolution behavior of OIPs. Future studies will expand this approach using a cell culture-based setup instead of synthetic membranes, within a humidified chamber, to assess airway epithelia transport behavior in a more representative manner.
Introduction
D
To mimic in vitro absorption across the human airway epithelia, a number of researchers have modified the cascade impactor with integrated epithelial cell monolayers to deposit respirable-sized particles directly onto cells(4,5); however, the main drawback in this approach is that these nozzle-based impactors may not necessarily represent the deposition behavior of inhaled drug in vivo.(6) To address this issue, a preliminary study by Huynh et al.(7) has evaluated the feasibility of modifying the medium-sized Virginia Commonwealth University (VCU) mouth–throat (MT) and tracheal–bronchial (TB) realistic upper airway model to accommodate Snapwell® inserts within the TB region, without any cells for drug collection and sampling. The airway model used in their study was a physical representation of the upper airway of an average sized human, which has provided excellent in vitro total lung dose predictions with in vivo outcomes.(8,9)
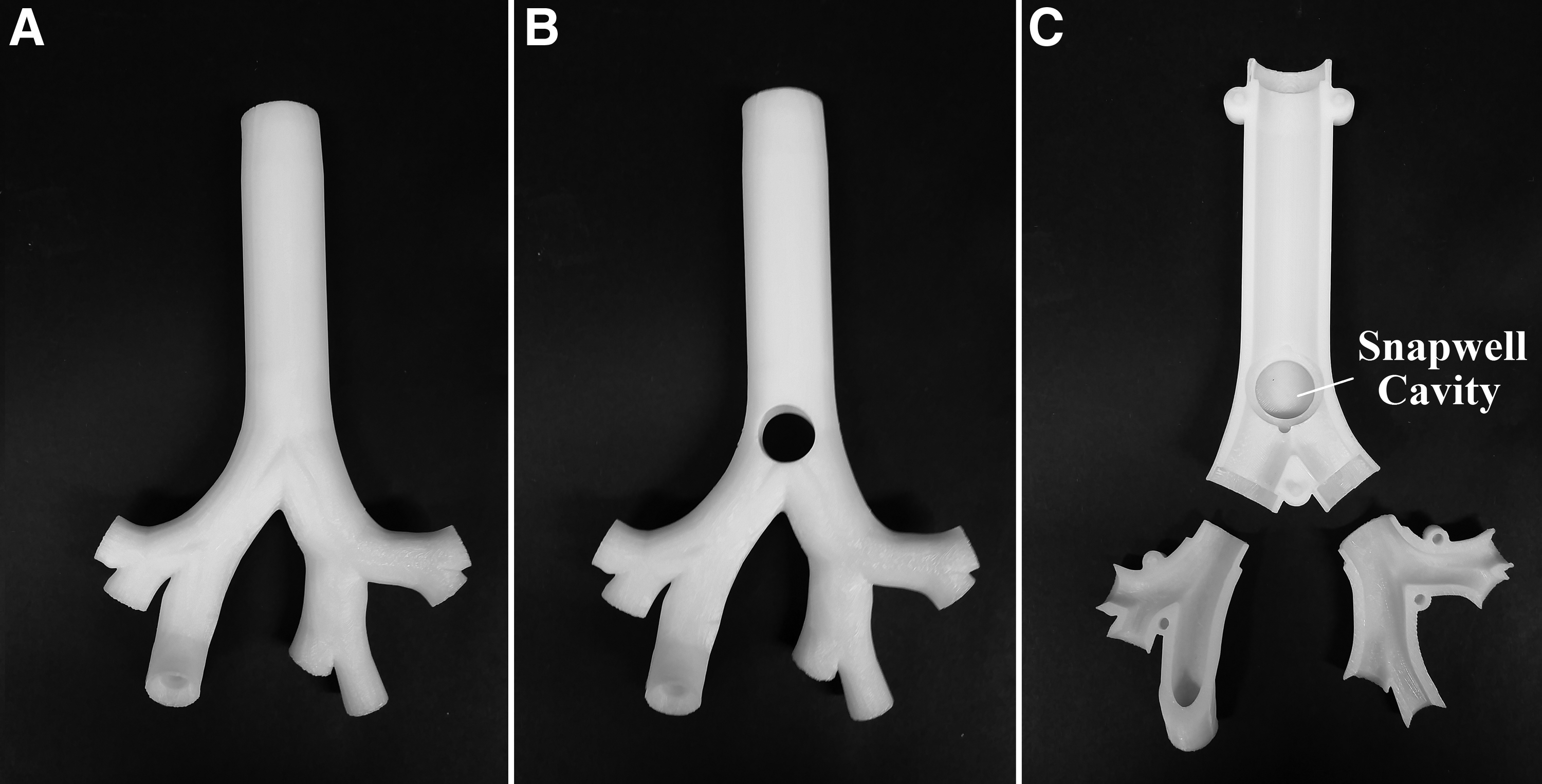
As a proof-of-concept study, Huynh et al.(7) were able to show high drug deposition hot spots in the upper and first TB airway bifurcation regions when ciprofloxacin-hydrochloride (CIP-HCL) solution was nebulized into the airway model. Two Snapwell inserts were placed above the first TB bifurcation region by drilling two 14.0 mm diameter holes, one at the front and the other at the back, with the inserts placed from the outside of the model to ensure internal flush conditions with the inner tracheal walls.(7) In vitro deposition studies of nebulized CIP-HCL showed no significant changes in airway deposition behavior between the unmodified and modified prototype models.(7)
We hypothesize in this study that this initial prototype of the modified-drilled TB airway model could be further modified to accommodate two Snapwell inserts within the model at these regions of interest to evaluate postdeposition behavior in vitro. Therefore, the aims of this study are to (a) modify and validate the existing prototype of the medium-sized VCU MT-TB airway to accommodate Snapwell inserts within the model for drug collection, (b) evaluate the feasibility in adapting the Snapwell test system to assess the permeation characteristics of already dissolved CIP-HCL solution through a series of different synthetic permeable membranes, and (c) utilize the optimized Snapwell test system to characterize and compare the permeation profiles of nebulized CIP-HCL droplets collected onto the Snapwell inserts within the modified TB airway model.
Materials and Methods
Development and validation of the modified airway model
The TB airway model was modified by dividing it into two separate halves to allow the insertion and removal of the standard polyester (PE) membrane Snapwell inserts (Corning® Costar® Snapwell cell-culture inserts, 12.0 mm with 0.4 μm pore size; Corning Life Sciences, MA), and a cavity at the first TB bifurcation was incorporated as shown in Figure 1C (MOD#2). The unmodified and previously modified (MOD#1) models of the medium-sized TB airway model are also displayed in Figure 1. The medium-sized MT (not shown) and modified TB airway model used in this study were manufactured from a clear acrylic photopolymer resin (GPLCL02) at a resolution of 0.025 mm using 3D rapid prototyping (Form 2 Desktop SLA 3D Printer; Formlabs, Inc., MN).
The medium-sized TB airway model:
In vitro realistic airway deposition of nebulized CIP-HCL solution
An in-house formulation of CIP-HCL aqueous solution, 20 mg/mL, was chosen as the model drug for this study. The formulation was prepared by dissolving CIP-HCL powder (MP Biomedical Australasia Pty Limited, NSW, Australia) in Milli-Q water. The MT model was made to snap fit on top of the TB model. Airway deposition of nebulized CIP-HCL solution onto the medium-sized MT and unmodified and modified (MOD#2) TB airway models were performed using the setup as shown in Figure 2.(7)

Physical setup of the modified airway model (MOD#2) used to assess in vitro airway deposition of nebulized CIP-HCL. CIP-HCL, ciprofloxacin–hydrochloride.
In brief, the TB airway region was housed in a custom-built housing assembly, with a vacuum pump attached at the base of the housing assembly, connected to a filter (Suregard®, Bird Healthcare, VIC, Australia) to draw ambient air through the airway model at 15.0 L/min. Three milliliters of CIP-HCL solution was loaded into the reservoir of a PARI LC Sprint® nebulizer (PARI Medical Holding GmbH, Starnberg, Germany) and delivered into the airway model by the PARI TurboBOY S compressor (PARI Medical Holding GmbH, Starnberg, Germany) for 5 minutes. Recovery of CIP-HCL in the PARI nebulizer, airway model, housing assembly, and filter was determined using known volumes of deionized water and quantified using ultra-fast liquid chromatography (UFLC) (See Drug quantification and data analysis section). Airway deposition experiments for each test condition were performed in triplicate.
Adapted in vitro Snapwell system for drug permeation
Suitability and discriminative ability of the Snapwell system for drug permeation
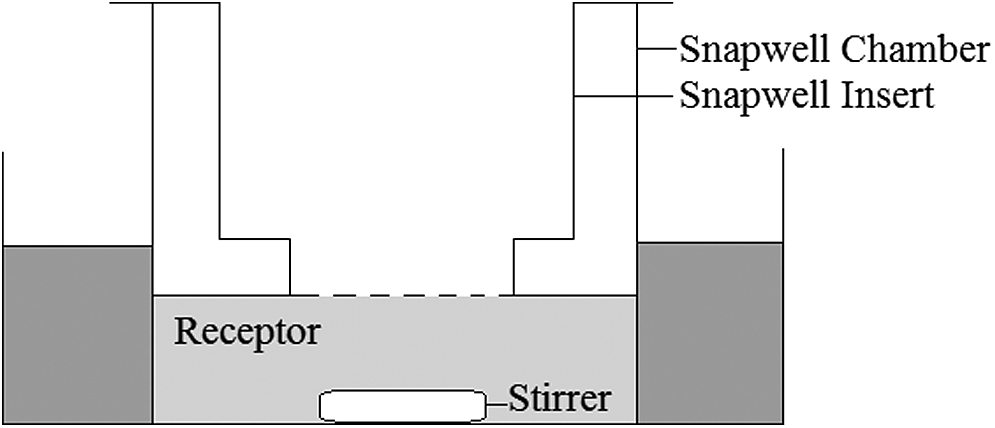
The Snapwell system consisted of a custom-made 3D-printed miniature chamber to accommodate a magnetic bar stirrer (8 × 3 mm, Westlab Group, Victoria, Australia) in the receptor compartment. The system was housed in a water bath at 37°C. A cross-section of the apparatus is shown in Figure 3. Components of the system were manufactured from a clear acrylic photopolymer resin (GPLCL02) (Form 2 Desktop SLA 3D Printer; Formlabs, Inc.).
In vitro experimental setup of the Snapwell test system
To assess the feasibility of the Snapwell test system, the permeation characteristics of the CIP-HCL solution was first assessed across the standard Snapwell PE membrane without any cells. Although the synthetic membrane does not resemble the complex structure of the airway epithelia, inferences regarding membrane permeability behavior can be made using this simplified setup.
Snapwell inserts were presoaked with phosphate-buffered saline (PBS) (Sigma-Aldrich, Sydney, Australia) up to 2 hours before permeation experiments. A 100.0 μL aliquot of 100.0 μg/mL CIP-HCL solution was applied directly on top of the membrane of the Snapwell insert that was placed in the holder chamber at time = 0. The receptor compartment consisted of 2.3 mL of PBS at pH 7.4 and was filled to ensure complete contact with the receptor-side membrane surface. A sample aliquot of 500.0 μL was withdrawn from the receptor compartment using a syringe at different time intervals for a period of 2 hours, with fresh prewarmed PBS replaced immediately to maintain a constant volume of 2.3 mL in the receptor compartment.
At the end of each experiment, the membrane was washed with deionized water to recover any remaining CIP-HCL on top of the membrane. The total amount of CIP-HCL permeated was calculated by determining the cumulative amount collected in the receptor compartment after 2 hours, plus the amount remaining on top of the membrane. The influence of a stirred versus a nonstirred receptor on the permeation behavior was investigated, with and without a magnetic stirrer in the receptor compartment. Permeation experiments for each test condition were performed in triplicate.
To investigate the discriminatory ability of the proposed Snapwell system, modified Snapwell inserts were created by removing the PE membrane from the insert and attaching either a polyamide (PA) membrane (Sartorius™, 0.45 μm pore size) or a layer of a regenerated cellulose dialysis membrane (Cellu-Sep®, regenerated cellulose tubular membrane, 6–8 kDa molecular weight cutoff) onto the insert. A 3D-printed ring was manufactured (Form 2 Desktop SLA 3D Printer; Formlabs, Inc.) to hold the membrane onto the Snapwell insert, using an approach similar to that reported by May et al.(10) Membranes were presoaked in PBS for 2 hours before experiments and 100.0 μL of 100 μg/mL CIP-HCL solution was applied directly onto the membrane. Experiments were tested with and without a stirrer in the receptor compartment. Permeation experiments for each test condition were performed in triplicate.
Permeation characteristics of nebulized CIP-HCL droplets collected on the modified model
To assess the permeability behavior of nebulized CIP-HCL droplets, two standard PE or modified Snapwell inserts (PA and dialysis membranes) were placed within the modified TB airway model (MOD#2) before realistic airway deposition experiments, to collect deposited nebulized CIP-HCL droplets onto the synthetic membrane inserts. Before airway deposition experiments, the inner walls and internal surface of the Snapwell inserts were covered with a removable thin 3D-printed sheet (Form 2 Desktop SLA 3D Printer; Formlabs, Inc.) as recommended by May et al.,(10) to allow for more accurate quantification of drug deposited onto the synthetic membranes. Airway deposition experiments were carried out using the same test conditions as described previously.
After deposition, the two inserts were transferred onto the Snapwell test system to assess the permeation characteristics through the different membranes, with a magnetic stirrer placed in the receptor compartment. Work from Arora et al. placed additional dissolution medium on the drug-deposited membranes to further facilitate the dissolution and permeation of the collected corticosteroid particles through the membrane.(11) Henceforth, additional experiments were conducted to assess whether the permeation of nebulized CIP-HCL droplets can be further facilitated through the membrane by adding 100.0 μL of deionized water on top of the drug-deposited membrane. Permeation experiments for each test condition were performed in triplicate.
Drug quantification and data analysis
Drug quantification of CIP-HCL was performed using the Shimadzu Prominence UFLC system (Shimadzu Corporation, Kyoto, Japan). The system consisted of an SPD-20A UV-vis detector, LC-20AD liquid chromatography, SIL-20A HT Autosampler, and Luna C-18 (2) 100A column (3 μm, 150 × 4.6 mm) (Phenomenex Pty, Ltd, Lane Cove, Australia). Chromatography conditions were conducted using a mobile phase composition of methanol and 0.1 M sodium dihydrogen phosphate at a 30:70 (v/v) ratio, with pH adjusted to 3.30 with phosphoric acid. The flow rate was set to 0.8 mL/min and 20.0 μL of each sample was injected into the column, with the column temperature set to 40°C and the detection wavelength of 275 nm. Linearity was obtained between 0.1 and 50.0 μg/mL (R2 > 0.999) at a retention time of 6.55 minutes. All solvents used were of analytical grade (Chem-Supply Pty Ltd, South Australia, Australia).
The statistical profile comparison employed unpaired two-tail t-test, where p < 0.05 was considered to be significant.
Results and Discussion
In vitro realistic airway deposition of nebulized CIP-HCL solution
Mass quantification, expressed as percentage total recovered dose of CIP-HCL remaining in the PARI nebulizer device, deposited on the MT and TB models, and ex-TB (determined by the drug recovered from the housing chamber and filter) using the modified and unmodified airway models are shown in Figure 4. Collectively, deposition on the modified TB model was determined by the drug recovered on the TB model, Snapwell inserts, and 3D-printed sheets.
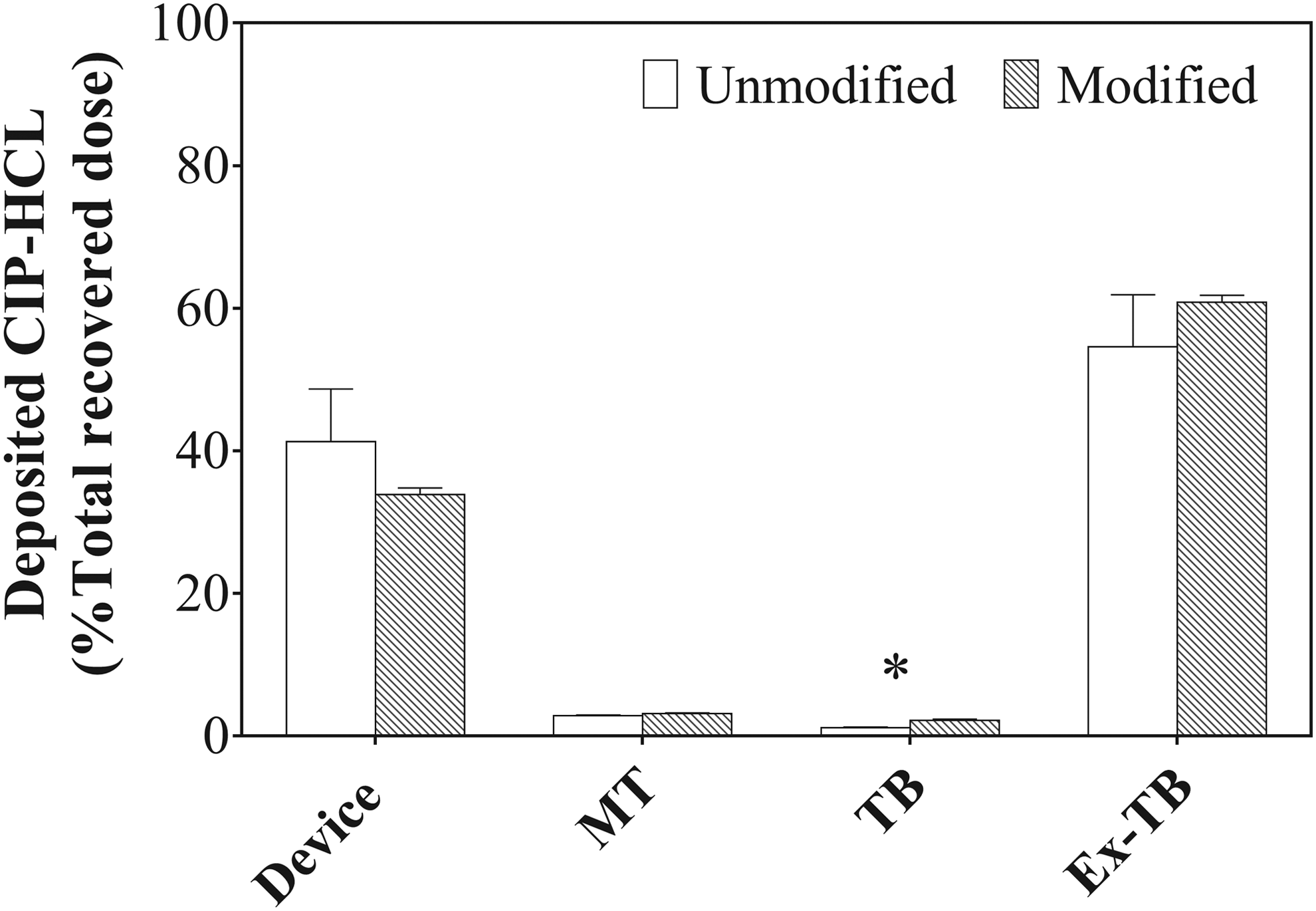
In vitro deposition results of nebulized CIP-HCL in the unmodified (white bars) and modified (gray bars) airway models for a total nebulization time of 5 minutes (n = 3; mean [error bars are ± SD]). Results are expressed as percentage total recovered dose. Ex-TB includes amount collected on the housing chamber and filter. Asterisks (*) indicates a statistically significant difference at p = 0.05.
No significant differences in MT deposition was observed in the unmodified and modified airway models, resulting in mean (SD) CIP-HCL deposition of 2.89% ± 0.06% and 3.13% ± 0.14% of the total recovered dose, respectively (p > 0.05, unpaired two-tail t-test); however, an increase in deposition was observed in the modified TB model (MOD#2), from 1.20% ± 0.075% to 2.18% ± 0.188% (p < 0.05, unpaired two-tail t-test). This observation conflicted with our previous modified prototype (MOD#1), which illustrated no significant changes in TB deposition.(7) It is important to note that the MOD#1 prototype was modified by drilling two holes to place the Snapwell inserts on the outside for complete flush conditions and for quick mass quantification of drug collected at this region; whereas in this study, MOD#2 comprised two cavities to house the inserts within the model and was not completely flush, hence most probably affecting the overall deposition behavior.
It is important to realize that large variations in whole lung deposition have been reported in healthy human subjects with gamma scintigraphy studies revealing high variations ranging from 20% to 60% of the total metered dose for a single test inhaler(12); furthermore, work by Delvadia et al.(8,9) has effectively captured this large variation seen in vivo by scaling the medium-sized VCU MT-TB airway model to generate small and large versions, and coupling these models with clinically relevant inhalation maneuvers; therefore, it could be concluded that the observed 1% increase in TB deposition lies within the expected variation observed in vivo. Although large variations seen in vivo are likely due to the range of airway geometries and differences in inspiratory maneuvers, the variations observed in this study are likely due to the structural changes within the airway model, that is, integration of the Snapwell inserts and 3D-printed sheets.
Nevertheless, the main aim of this study was to develop and modify the realistic medium-sized VCU MT-TB upper airway model primarily to collect aerosolized drug onto Snapwell inserts in a more representative model for postdeposition evaluation. Successfully, 8.2 ± 1.7 and 13.2 ± 2.2 μg of CIP-HCL were deposited on the front and back Snapwell inserts, respectively, when nebulized for 5 minutes. Collectively, approximately 25.0 μg of CIP-HCL was collected on the individual 3D-printed Snapwell sheet covers.
Adapted in vitro Snapwell test system for drug permeation
Suitability and discriminative ability of the Snapwell system for drug permeation
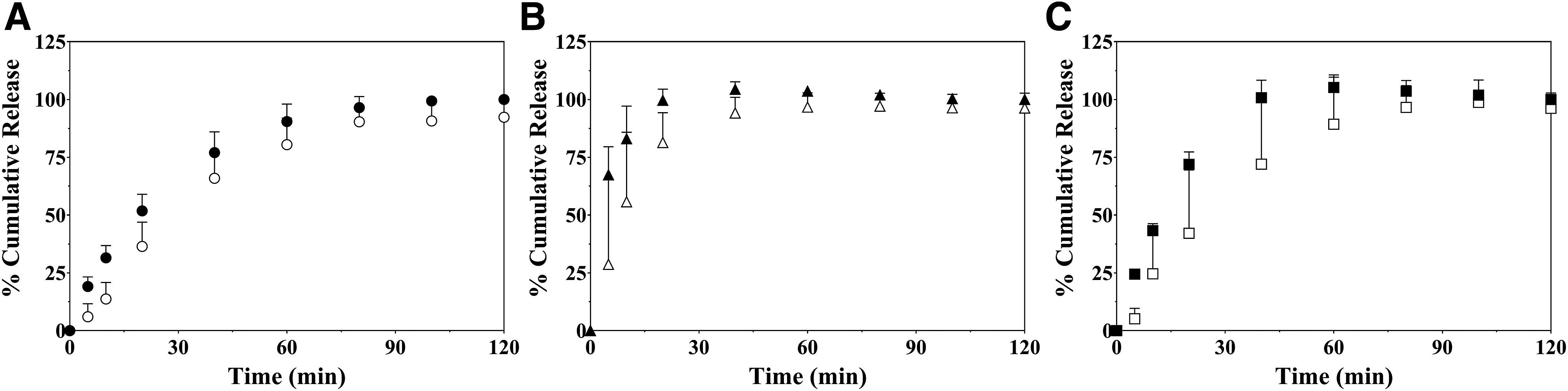
The percentage cumulative mass of CIP-HCL solution permeating through the PE, PA, and dialysis membranes into the receptor compartment, tested under static (no stirrer) and agitated (stirrer) conditions is shown in Figure 5A–C, respectively. It was apparent that the permeation behavior of already dissolved CIP-HCL differed considerably through the selected membranes. For the PA membrane, there was fast initial permeation with complete transfer of CIP-HCL observed after 20 minutes when a magnetic stirrer was placed in the receptor compartment. Slower, yet complete transfer was observed for the other two membranes.
Percentage cumulative mass release of CIP-HCL solution through the
This can be explained by the differences in membrane structure and the physical interactions between the aqueous solution and the material surface. The aqueous solution has a better affinity to the most hydrophilic PA membrane, resulting in complete wetting of the solution onto the whole surface area, whereas with the tissue culture-treated PE membrane and dialysis membranes, poorer surface wettability behavior was observed at the beginning of the experiments when the solution was loaded directly on top of these membranes, which may explain the slower and more gradual permeation through these two membranes. Similarly, May et al.(10) reported slower drug permeability behavior from the PE membrane for a range of drug substances, with scanning electron microscopy images showing PE being less porous and having fewer permeation areas.
As expected, stirring in the receptor compartment provided adequate mixing of CIP-HCL solution and PBS in the receptor compartment, resulting in smaller experimental variability.(13)
Permeation characteristics of nebulized CIP-HCL droplets collected on the modified model
The permeation behavior of nebulized CIP-HCL droplets, which have been collected onto the front and back Snapwell inserts in the modified TB airway model, with or without additional water added on the PE, PA, and dialysis membranes is shown in Figure 6A–C, respectively. Only approximately 50.0% of the deposited nebulized CIP-HCL permeated through all the tested membranes without any additional water after a 2-hour sampling period, perhaps indicating that drug deposited as droplets on the membrane surface became dried after evaporation of water.
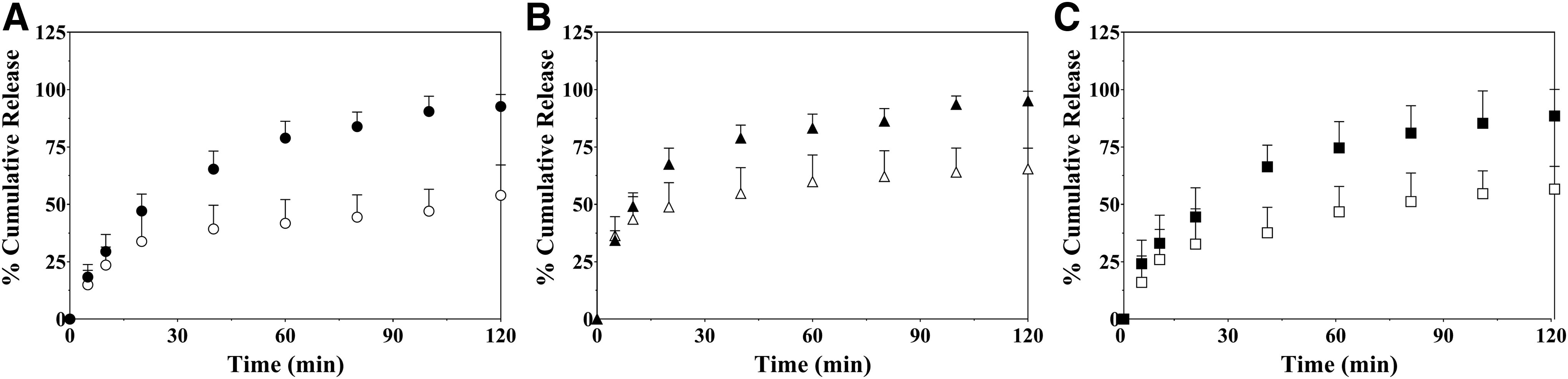
Percentage cumulative mass release behavior of nebulized CIP-HCL droplets permeated through the front and back membranes of the
As expected, additional water on the nebulized droplets increased both the rate and extent of the permeation behavior, with approximately 75%–90% of CIP-HCL permeating through the membrane by the end of the experiment. It is thought that adding water on top of the membrane enhanced the increased dissolution on the donor compartment and spread of CIP-HCL onto the surface membrane, increasing the surface area coverage of CIP-HCL onto the porous areas, hence facilitating the permeation of CIP-HCL into the receptor compartment. As such, the altered rate and extent of permeation may reflect a dissolution step for the deposited nebulized droplets on the membranes.
In conclusion, a modified version of the existing medium-sized VCU MT-TB airway model (MOD#2) has been presented to assess realistic airway deposition and drug permeation behavior of the nebulized CIP-HCL drug across a range of synthetic membranes using the Snapwell test system. Although the synthetic membranes used in this study do not resemble the complex structure of the epithelial airway barrier, we were able to show how different types of membrane materials, presence or absence of a stirrer in the receptor compartment, and aerosol particle collection method can significantly influence drug permeation behavior. Furthermore, the feasibility in adapting the Snapwell test system have provided reproducible and discriminatory permeation profiles for the already dissolved and nebulized CIP-HCL solution.
Future work will focus on expanding this hybrid approach to a cell culture-based setup, by integrating epithelial cell monolayers onto Snapwell inserts before airway deposition experiments. To make in vitro testing more representative of in vivo conditions, the Snapwell system will be placed within a humidified chamber.
Footnotes
Author Disclosure Statement
The authors are faculty and students from the Woolcock Institute of Medical Research and the Virginia Commonwealth University. No conflicts of interest exist.