
Abstract
Abstract
Background:
Effective delivery of inhaled drugs in chronic obstructive pulmonary disease (COPD) depends on patients' ability to correctly use an inhalation device. Nebulized delivery may be appropriate for COPD patients who cannot coordinate breath with inhalation or generate adequate inhalational force. Until recently, long-acting muscarinic antagonists (LAMAs), used for maintenance treatment of COPD, were available for delivery only via handheld inhalers. Lonhala™ Magnair™ (glycopyrrolate inhalation solution) is a LAMA delivered via the eFlow® closed-system (eFlow CS) vibrating membrane nebulizer. We assessed patient-reported ease of use and satisfaction with the eFlow CS nebulizer in the GOLDEN (Glycopyrrolate for Obstructive Lung Disease via Electronic Nebulizer)-5 study.
Methods:
GOLDEN-5, a phase 3, randomized, open-label trial, evaluated the safety and efficacy of glycopyrrolate/eFlow CS 50 μg twice daily versus tiotropium 18 μg once daily (administered via HandiHaler™) in patients with moderate-to-very severe COPD. Only patients in the glycopyrrolate/eFlow CS group completed a study-specific device use questionnaire, evaluating patients' perceptions about ease of use, confidence in drug delivery, and overall device satisfaction at week 48 or end of study. Responses were summarized by counts and percentages.
Results:
Of 620 patients who received glycopyrrolate/eFlow CS, 454 completed the questionnaire (mean age [standard deviation, SD] 63.3 [8.5] years; mean BMI [SD] 28.45 [6.208] kg/m2). Based on patient-reported perceptions, most patients (83%) were “confident” to “very confident” that the drug was delivered into their lungs with the eFlow CS; >70% rated the eFlow CS as “easy” or “very easy” to assemble, operate, and clean. Most (75%) patients ranked themselves as being “satisfied” or “very satisfied” overall with the eFlow CS nebulizer.
Conclusions:
High levels of satisfaction, confidence, and ease of use were reported with the eFlow CS nebulizer in this study. These findings support the use of the eFlow CS for maintenance treatment of COPD with glycopyrrolate inhalation solution.
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive lung function disorder characterized by breathlessness, excessive sputum production, and chronic cough. COPD affects more than 27 million people in the United States and is associated with a substantial economic burden with the estimated direct medical costs projected to rise to $49 billion in 2020.(1)
Long-acting bronchodilators such as long-acting beta2-agonists (LABAs), LAMAs, a combination of these two classes (LAMA/LABA), or LABAs with inhaled corticosteroids are the mainstay of COPD treatment, and are used for improving lung function and symptoms to reduce costly exacerbations for these patients.(2)
Several inhalational devices such as metered dose inhalers (MDIs), dry powder inhalers (DPIs), soft-mist inhalers (SMIs), or nebulizers are available to administer COPD medications. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines emphasize an individualized approach toward treatment and device selection for COPD treatment, and factors such as a patient's age, cognitive status, visual acuity, dexterity, and ability to coordinate actuation with the inhaler should be considered when selecting an appropriate approach for medication delivery.(2)
While handheld devices such as MDIs, DPIs, and SMIs are suitable for patients with the ability to inhale all medication in a single or few breaths and overall hand/breath coordination,(3) nebulizers could be an appropriate choice for patients with compromised dexterity, very low inspiratory flow rates, and poor hand/breath coordination.(4) Currently available nebulizers include jet, ultrasonic, and vibrating mesh/membrane devices. Jet nebulizers vary in size, are typically less portable, and may take up to 20 minutes to administer medication. Ultrasonic and vibrating mesh/membrane nebulizers typically have shorter administration times and are more portable than jet nebulizers.
Lonhala™ Magnair™ (glycopyrrolate inhalation solution; Sunovion Pharmaceuticals, Inc., Marlborough, MA) is a U.S. Food and Drug Administration (FDA)-approved drug/device combination that uses the eFlow® closed system nebulizer (hereafter referred to as eFlow CS; a registered product of PARI Pharma GmbH; Starnberg, Germany) to deliver glycopyrrolate 25 μg twice daily (BID). It is the first and only nebulized LAMA currently approved for COPD.
The eFlow CS uses a vibrating membrane technology to deliver the 25 μg/1 mL dose of medication in 2 to 3 minutes, with a virtually silent operation. It is administered as a soft aerosol mist, targeting drug deposition to the lungs with regular tidal breathing, and is designed specifically for use with a proprietary blow-fill-seal vial of glycopyrrolate that can be opened only by attaching it to the nebulizer (Fig. 1).(5) This design is intended to minimize the potential for user error or misuse.(6) The reference product used as active comparator in this study was Spiriva HandiHaler®.

Magnair™ nebulizer system.
Glycopyrrolate/eFlow CS has been demonstrated to be safe and efficacious for maintenance treatment of COPD, and these results have been reported elsewhere.(7,8) There is a need to better understand COPD patient perceptions about the ease of use of the eFlow CS nebulizer and satisfaction with this device, both of which could have an impact on patient adherence. In this article, we present findings from a long-term safety study on patient-reported perceptions about ease of use, confidence in drug delivery, and satisfaction with the eFlow CS nebulizer. Analyses that explored the relationships between device satisfaction and key efficacy outcomes are also presented.
Materials and Methods
Study design
The GOLDEN (Glycopyrrolate for Obstructive Lung Disease via Electronic Nebulizer)-5 study was a phase 3, 48-week, randomized, open-label, parallel-group, multicenter safety and efficacy trial of nebulized glycopyrrolate/eFlow CS versus tiotropium in patients with moderate-to-very severe COPD (ClinicalTrials.gov: NCT02276222). The trial consisted of a screening period, a 48-week open-label treatment period, and a safety follow-up telephone call (∼52 weeks total; Fig. 2). Patients were randomized 4:3 to glycopyrrolate/eFlow CS 50 μg BID or tiotropium (Spiriva HandiHaler) 18 μg once daily (delivered via HandiHaler), respectively. The first morning dose of eFlow CS nebulizer therapy was administered in the clinic. The evening dose was administered in the home setting.
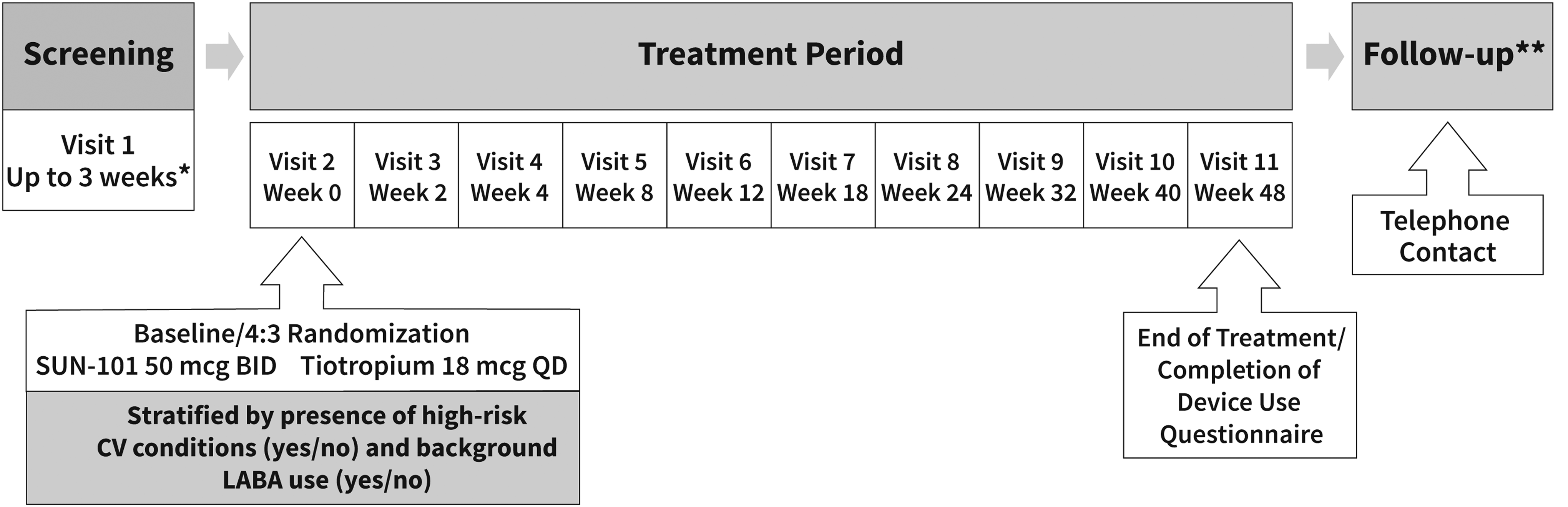
GOLDEN-5 study schematic. BID, twice daily; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; GOLDEN, Glycopyrrolate for Obstructive Lung Disease via Electronic Nebulizer; LABA, long-acting beta2-agonist; QD, once daily. *Visit 1 may have occurred over more than one clinic visit and may have been up to 3 weeks but must have been a minimum of 1 week before randomization (visit 2) to ensure that at least 1 week of rescue medication use and COPD symptoms were recorded before randomization. **All patients were contacted by telephone 5–7 days after the last study visit or end of treatment for a final safety assessment.
All study procedures followed the Declaration of Helsinki, and institutional review board approval was received. All patients or their legal representatives provided informed consent.
Inclusion/exclusion criteria
GOLDEN-5 was designed to recruit a representative population of COPD patients, including patients with very severe COPD, cardiovascular risk (defined as patients with pre-existing diagnosis of ischemic heart disease, cerebrovascular disease, peripheral arterial disease, hypertension, clinically significant arrhythmia, or heart failure), and on background LABA treatment (Fig. 2).
Patients were included if they met the following criteria: ≥40 years old, moderate-to-very severe COPD, ability to perform reproducible spirometry as per the 2005 American Thoracic Society and European Respiratory Society guidelines, postbronchodilator forced expiratory volume in 1 second (FEV1) <80% predicted and >0.7 L, FEV1/forced vital capacity ratio of <0.7, and current or former smokers with a smoking history of ≥10 pack-years. Key exclusion criteria were history of unstable cardiac disease or long QT syndrome, prolonged QTc (males, >450 msec; females, >470 msec) at screening, concomitant asthma or other clinically significant respiratory disease (e.g., tuberculosis, bronchiectasis), recent history of COPD exacerbation requiring hospitalization, or need for increased COPD treatments within 6 weeks before screening.
Assessments
Safety endpoints in the trial included the incidence of any treatment-emergent adverse events (TEAEs), discontinuation due to TEAEs, serious adverse events, and major adverse cardiovascular events. Lung function, symptoms, health status, and satisfaction with the eFlow CS nebulizer were other assessments conducted in the trial.
Device use questionnaire
Only patients in the glycopyrrolate/eFlow CS group in the GOLDEN-5 trial completed a device use questionnaire in clinic at week 48 or at an end-of-study (EOS) visit using an electronic tablet device (Bracket Global, Wayne, PA).
The 20-item questionnaire was developed specifically to evaluate patient experience with the eFlow CS nebulizer in the GOLDEN-5 trial. The questionnaire included 12 questions related to patients' overall perceptions on ease of use with the eFlow CS nebulizer, confidence in drug delivery, overall satisfaction with the device, and willingness to use the device (Questions 9–20); 3 questions (Questions 1–3) were regarding the devices that patients used before enrolling in the trial; and 5 questions (Questions 4–8) compared patients' experience and overall satisfaction with the use of eFlow CS nebulizer compared with another nebulizer that they may have used before study entry.
Responses to confidence in drug delivery and overall satisfaction with the eFlow CS nebulizer were measured on a four-point Likert scale (e.g., “not satisfied,” “somewhat satisfied,” “satisfied,” and “very satisfied”); device handling and cleaning were measured on a five-point Likert scale (e.g., “very difficult,” “somewhat difficult,” “acceptable,” “easy,” and “very easy”); and experience and satisfaction with the eFlow CS nebulizer compared with a previously used nebulizer were also measured using a five-point Likert scale (e.g., “much more difficult,” “somewhat more difficult,” “about the same,” “somewhat easier,” or “much easier”).
Secondary analyses
Secondary analyses were conducted to evaluate associations between patient satisfaction with the use of the eFlow CS nebulizer and changes in outcomes, as measured by change from baseline in trough FEV1 and St. George's Respiratory Questionnaire (SGRQ) and the proportion of responders on each outcome, at week 48, or EOS. Each responder subgroup that reported “not satisfied,” “somewhat satisfied,” “satisfied,” or “very satisfied” was measured as a percentage of the total group. An increase of ≥100 mL in FEV1 and a decrease of four or more units on the SGRQ total score are considered clinically significant.(9) In addition, association between satisfaction with the eFlow CS nebulizer and age, gender, and smoking status was assessed.
Statistical methods
Means and percentages were calculated for continuous and discrete variables, respectively. The complete level-by-level percentage of responses for each question was reported for survey Questions 4–20. For purposes of interpretation and reporting, each of the four-point response categories for confidence, satisfaction, and ease of use was combined into fewer categories (e.g., not confident/somewhat confident vs. confident/very confident; very difficult/somewhat difficult vs. easy/very easy).
Chi-square tests were used to test association between level of satisfaction and responders based on FEV1 (defined as a minimum of 100 mL change from baseline in trough FEV1) and SGRQ total score (≥4 U decrease from baseline) at week 48 or EOS. A chi-square test was also used to analyze whether there was a difference in level of satisfaction by age category (<65, 65–74, and ≥75), gender, and smoking status (current vs. former). Association between patient satisfaction and change from baseline in trough FEV1 and SGRQ total score was evaluated using multiple linear regressions after adjusting for cardiovascular risk (high vs. low), baseline severity, and background LABA use. All statistical tests were two sided and used a significance level of 0.05. No adjustments were made for multiple outcomes being assessed.
Results
Patient characteristics
A total of 620 patients received glycopyrrolate/eFlow CS, and 454 (73.2%) patients completed the device use questionnaire at week 48 or EOS. The mean patient age (±standard deviation) was 63.3 years (±8.5); 94% of patients were white, and 53% were current smokers (Table 1). Four of five patients (82%) previously used an MDI or DPI. More than one-third of patients had prior experience with a nebulizer (Table 2).
Baseline Characteristics of Patients in the Glycopyrrolate/eFlow CS Arm in the GOLDEN-5 Trial
High cardiovascular risk conditions include ischemic heart disease, cerebrovascular disease, peripheral arterial disease, hypertension, clinically significant arrhythmia, or heart failure.
In-Check inspiratory flow meter was set to “resistance of HandiHaler.”
COPD, chronic obstructive pulmonary disease; eFlow® CS, eFlow closed system; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GOLDEN, Glycopyrrolate for Obstructive Lung Disease via Electronic Nebulizer; LABA, long-acting beta2-agonist; PIFR, peak inspiratory flow rate; SD, standard deviation.
Device Satisfaction Questionnaire Responses from Patients Using the eFlow CS Nebulizer
Due to rounding errors, values may add up to more than 100%.
DPI, dry powder inhaler; MDI, metered dose inhaler.
Device use outcomes
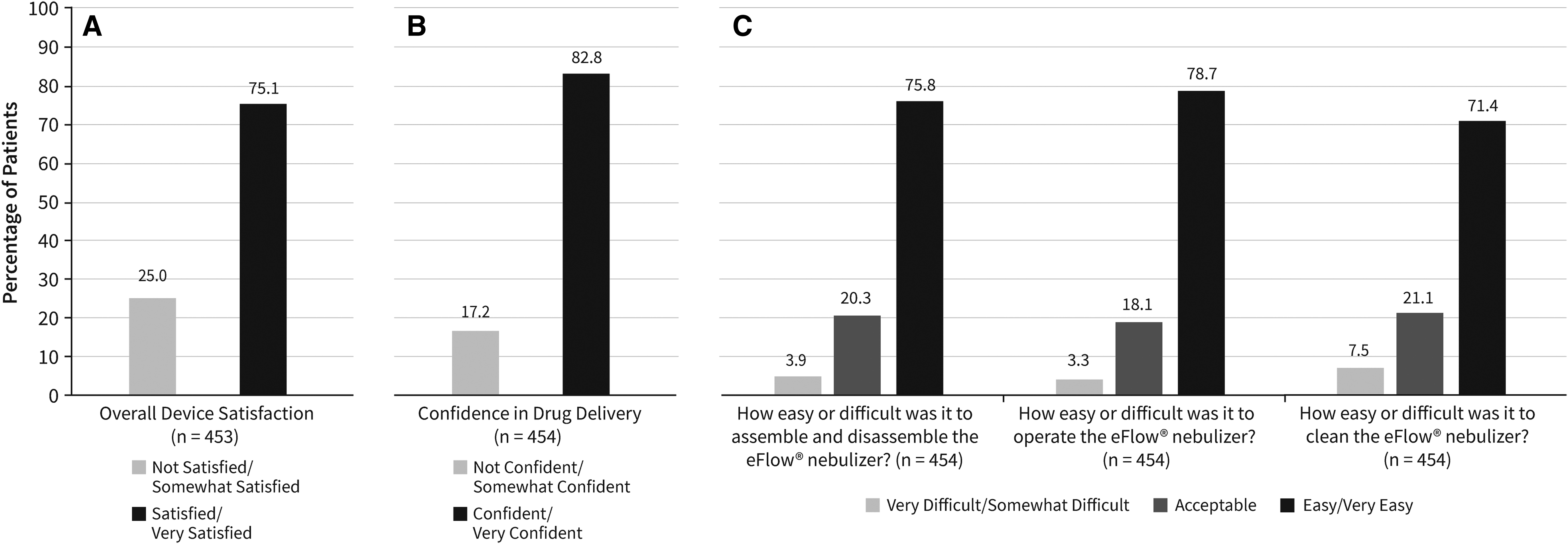
The percentage of patients providing a response to each question, by each response category, is reported in Table 2. Regardless of prior nebulizer use, 340/453 patients (75%) rated their overall satisfaction with eFlow CS as either “satisfied” or “very satisfied” after 48 weeks of use (Fig. 3A; Table 2, Question 14). In addition, 376/454 patients (83%) reported being “confident” to “very confident” that eFlow CS delivered glycopyrrolate into their lungs (Fig. 3B; Table 2, Question 13). A majority of patients rated the eFlow CS as “easy” or “very easy” to assemble (344/454 [76%]), operate (35/454 [79%]), and clean (324/454 [71%]) (Fig. 3C; Table 2, Questions 9–11).
Patient-reported.
A high percentage of patients also rated the device as being lightweight (398/454 [88%]) and the ideal size (402/454 [89%]) (Table 2, Questions 16, 17). Overall, 69% (312/454) of patients reported that they would feel “confident” to “very confident” using the eFlow CS nebulizer every day if it was available (Table 2, Question 20).
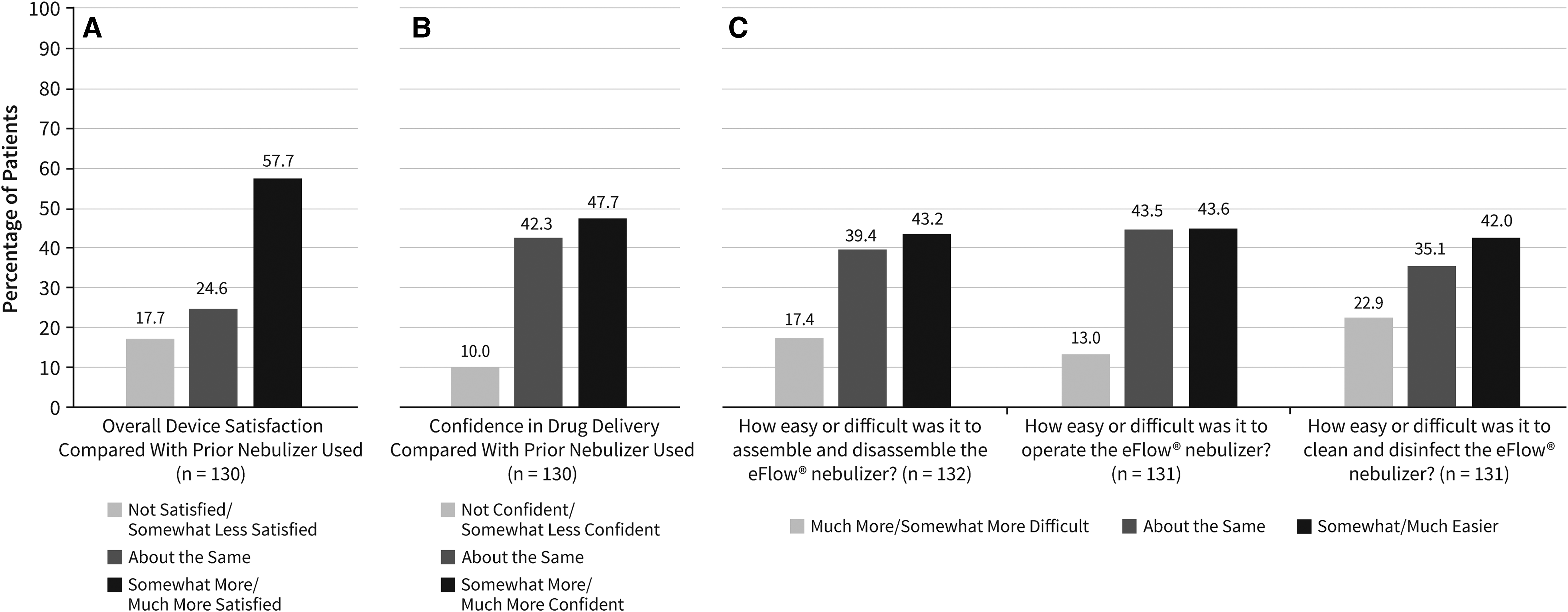
Among patients who had previously used a nebulizer, 58% (75/130) reported that they were “somewhat more” or “much more” satisfied with the eFlow CS than their previous nebulizer (Fig. 4A; Table 2, Question 8). In addition, 48% (62/130) of patients reported being “somewhat more” or “much more” confident in drug delivery with the eFlow CS compared with their previous nebulizer (Fig. 4B; Table 2, Question 7), while 42% (55/130) rated their confidence in the eFlow CS the same as for their previous nebulizer. Many patients reported that the eFlow CS was easier to assemble/disassemble (57/132 [43%]) and clean/disinfect (55/131 [42%]) than their previous nebulizer, and 44% (57/131) of patients reported ease of use to be “about the same” compared with their previous nebulizer (Fig. 4C; Table 2, Questions 4–6).
Patient-reported.
Relationship of device satisfaction with patient outcomes and baseline characteristics
Chi-square analyses of associations between satisfaction levels and responders based on FEV1 and SGRQ total score (Table 3) at week 48 showed no statistically significant relationship between patients' response on outcomes and their perception of satisfaction with the nebulizer. For instance, 137 of 182 (75%) patients who had experienced <100 mL FEV1 improvement by EOS reported that they were either “satisfied” or “very satisfied” with the eFlow CS nebulizer; this was comparable with the percentage of patients (82%) who reported that they were either “satisfied” or “very satisfied” with the nebulizer among those who achieved an improvement in FEV1 ≥ 100 mL. Similar results were observed for the association between SGRQ response rates and device satisfaction (Table 3).
Chi-Square Analyses of Association Between Satisfaction with eFlow CS Nebulizer, FEV1 and St. George's Respiratory Questionnaire Responders at Week 48
SGRQ, St. George's Respiratory Questionnaire.
The multivariate linear models showed a trend of improved outcomes (change from baseline in mean trough FEV1 and SGRQ total score) among patients who had higher levels of satisfaction, although the models had weak explanatory power (R2 = 0.071 for change in FEV1 and R2 = 0.1135 for change in SGRQ total score) and hence are not reported in this article. Chi-square tests for association between satisfaction and baseline characteristics such as age group, gender, and smoking status did not reveal any significant difference in satisfaction levels by these baseline characteristics (Table 4).
Chi-Square Analyses Evaluating Level of Satisfaction with eFlow CS Device by Baseline Characteristics
Discussion
Glycopyrrolate 25 μg BID delivered via eFlow CS is the first FDA-approved nebulized LAMA medication for maintenance treatment of COPD. As such, glycopyrrolate/eFlow CS bridges the gap in treatment for patients who need LAMA therapy or may have difficulty using a handheld device. Patients appropriate for this therapy may include those with compromised dexterity, low peak inspiratory flow rate, or poor hand/breath coordination. In addition, physicians now have a choice to add a nebulized LAMA treatment for patients who are already on a nebulized LABA but need additional bronchodilation.(3)
The device use assessment findings from the long-term safety trial showed that a majority of patients reported being satisfied with the eFlow CS nebulizer and confident that the device was delivering the medication to their lungs. Furthermore, a majority of patients reported the eFlow CS nebulizer to be lightweight and easy to assemble, operate, and clean. Among patients who had previously used another type of nebulizer, the majority reported they were more satisfied with the eFlow CS nebulizer.
Nebulizers are generally perceived to be bulky and inconvenient to use with a longer drug administration time.(10,11) Despite this, studies have shown that satisfaction with nebulizer devices is generally high; 80% of COPD patients on nebulized therapy reported that nebulizer use is perceived to be better than using an inhaler alone, specifically with respect to symptom relief (i.e., easier breathing and chest feels more comfortable) and improved quality of life.(12)
Patient preference studies have reported that ease and convenience of use, portability, shorter administration time, and perceived device efficacy are among the most important device attributes that were important for patients.(13–15) In a direct comparison of nebulizer devices, the I-neb Adaptive Aerosol Delivery System vibrating mesh nebulizer (available in the United Kingdom) was rated higher than a previous nebulizer (most often the jet type) used by COPD patients, in terms of reported confidence in drug delivery and overall desirability of the device.(16)
Similarly, in the current study assessing patient-reported perceptions, approximately three of five patients with previous nebulizer use reported being more satisfied with the eFlow nebulizer (vibrating membrane), and approximately one in two patients reported more confidence in delivery of medication into the lungs compared with the previous nebulizer. Whether these findings translate to improved adherence among patients needs to be evaluated.
Study results showed that patient's perception about satisfaction with the eFlow CS nebulizer was not influenced by overall efficacy of the drug/device combination. The results also showed that the level of satisfaction reported by patients with the eFlow CS nebulizer did not differ significantly by age, gender, or smoking status, suggesting that the device might be considered acceptable by a broad group of COPD patients.
Several caveats of the study need to be acknowledged. First, the long-term safety study used a 50 μg BID glycopyrrolate dose, which is not a U.S. FDA-approved dose. Whether the findings about device use and satisfaction would change if studied with the 25 μg dose could not be evaluated. The device use questionnaire was developed for the purpose of evaluating patient experience with the eFlow CS nebulizer specifically for use in the GOLDEN-5 study. While it was ensured that the survey instrument had face validity, formal validation of the survey was not conducted. Given that the survey was specific to the eFlow CS nebulizer, comparisons of device use and satisfaction with the active control group could not be drawn from this assessment. About 27% of the patients did not provide an assessment of the device as they were lost to follow-up and their experience of the device is unknown.
Inherent to surveys and the 48-week study duration, patient responses regarding prior nebulizer use may suffer from recall bias. Hence, the findings on patient-reported readiness to switch or satisfaction relative to previous nebulizer use must be interpreted with caution. A randomized crossover study design in which patients are switched from one nebulizer or inhaler device to the eFlow CS may have been a more appropriate approach to comparing perceived levels of satisfaction and ease of use between one inhaler/nebulizer type and the eFlow CS. Finally, a caveat with regard to the suitability of nebulizers in general for patients with compromised dexterity or cognition could be that these patients would likely need assistance in setting up and cleaning the device.
Conclusions
In an open-label long-term safety study of glycopyrrolate/eFlow CS, patients receiving this treatment reported high rates of overall satisfaction with the eFlow CS nebulizer. The majority of patients rated the eFlow CS nebulizer as being easy or very easy to assemble, operate, and clean, and reported they were confident that the device delivers drug into their lungs. These findings support the use of the eFlow CS nebulizer with glycopyrrolate inhalation solution for maintenance treatment of COPD. Future studies are needed to evaluate the impact of the drug/device combination on patient adherence in the real world.
Footnotes
Acknowledgments
Heather King, PhD, D. Michele Nikoloff, PhD, and Claudette Knight, PharmD, of Percolation Communications LLC provided medical editorial support. Medical editorial support was funded by Sunovion Pharmaceuticals, Inc.
Author Disclosure Statement
Sunovion Pharmaceuticals, Inc. provided funding for this research. E.M.K. has received consultancy and advisory fees from Amphastar, AstraZeneca, GlaxoSmithKline, Mylan, Novartis, Oriel, Pearl, Sunovion, Teva, and Theravance. He has conducted multicenter clinical research trials for ∼40 pharmaceutical companies. J.F.D. has received consultancy and advisory fees from Sunovion Pharmaceuticals, Inc. G.T.F. has received research funding and/or consultancy and advisory fees from Sunovion Pharmaceuticals, Inc., Boehringer Ingelheim, AstraZeneca, Pearl Therapeutics, Verona, Theravance, Mylan, Innoviva, GlaxoSmithKline, and Circassia. V.G., A.O.-G., and K.R. are full-time employees of Sunovion Pharmaceuticals, Inc.
Reviewed by:
Thomas O'Riordan, Laurent Vecellio