
Abstract
Purpose:
To validate the oncological safety of fertility preservation in malignant ovarian germ cell tumors (MOGCTs) and to define the significance of maximal cytoreduction in early stage MOGCTs.
Materials and Methods:
Sixty-nine patients with stage I and II MOGCTs who underwent surgical treatment were included in the study. Fertility-sparing surgery is defined as conservative surgery and hysterectomy and contralateral salpingo-oophorectomy were defined as definitive surgery. Both surgical approaches involved lymphadenectomy and omentectomy. Most patients received platinum-based combinations for adjuvant therapy. Survival outcomes of the conservative surgery group were compared with the definitive surgery group.
Results:
Median age of the study group was 21 years (range: 12–40 years). Median tumor size measured 150 mm (range, 20–300 mm). Surgery type (conservative surgery vs. definitive surgery) and lymphadenectomy (performed vs. not performed) were insignificant for the recurrence (p = 0.758, p = 0.271). However, surgical outcome (maximal vs. optimal and suboptimal) and type of tumor (dysgerminoma vs. nondysgerminoma) determined the recurrence (p = 0.001, p = 0.021).
Conclusion:
Fertility-conserving approach is safe in early stage MOGCTs. However, maximal cytoreduction should be achieved in this group of patients, without conceding fertility-conserving approach. On the other hand, development of chemotherapy options with less gonadotoxic effects, but equal or stronger efficiency in comparison with platinum-based chemotherapy, will certainly facilitate management of this patient group.
Introduction
O
The average age of first childbirth increased by 3.5 years, from 21.4 years in 1970 to 24.9 years in 2000. 5 In addition to advanced maternal age, diagnosing germ cell tumors at an early age due to the very nature of this tissue necessitated an approach of conserving fertility for those tumors. At first glance, 95% of those tumors are unilateral, excluding dysgerminoma, and spread to uterus is rare. 6 On the other hand, platinum-based chemotherapy offers high recovery rate. These features of MOGCTs posed a limitation on requirement of aggressive surgery and made the fertility-conserving approach standard management of malignant germ cell tumors.7–12
In this study, we evaluated the oncological outcomes of fertility-sparing surgery in patients with stage I-II MOGCTs. Our primary aim was to prove the oncological safety of fertility preservation in ovarian germ cell tumors and to define the significance of maximal cytoreduction in early stage MOGCTs.
Materials and Methods
Sixty-nine patients with stage I and II MOGCTs who underwent surgical treatment were included in the study. International Federation of Gynecology and Obstetrics 2014 staging system was used for tumor staging. Demographics, intraoperative findings, data on pathological examination of surgical specimen, recurrence, and survival data were derived from patient files, pathology reports, and electronic database of gynecologic oncology clinic. In case of recurrence, time and location of the recurrence and cause of death, if any, were also noted.
A median infraumbilical incision was used for initial exploratory laparotomy. Peritoneal cytology was sampled from ascites or peritoneal lavage fluid if there were no ascites. An oophorectomy or cystectomy was performed to excise the ovarian mass. Material was intraoperatively assessed with frozen section examination. If MOGCT was reported, incision was extended above the umbilicus. Then, peritoneal and retroperitoneal compartments and abdominal viscera were carefully explored and palpated to determine the extent of the tumor spread.
Fertility-sparing surgery is defined as conservative surgery. Definitive surgery includes hysterectomy and contralateral salpingo-oophorectomy. Both surgical approaches involved lymphadenectomy and omentectomy. In addition, cytoreductive surgery techniques were performed in patients with intra-abdominal spread (pelvic spread), irrespective of the fertility-conserving approach. The type of surgical approach was at the senior surgeon's discretion with reference to age of the patient and the future plan of pregnancy. All surgical procedures are performed by gynecologic oncologists. Maximal debulking was defined as no gross residual tumor after primary or recurrence surgery, and optimal and suboptimal debulking were used for patients with residual tumors of ≤1 cm and >1 cm, respectively.
Intraoperative findings and paraffin section results of patients were discussed in gynecologic oncology tumor board after surgical treatment. Patients with stage IC disease or above, patients with immature teratoma or high-grade tumors, and patients with residual disease after cytoreductive surgery were offered to receive adjuvant chemotherapy. Platinum-based combinations constituted the mainstay of adjuvant therapy. Disease-free survival (DFS) is defined as the time elapsed until postoperative recurrence or last contact, while disease-specific survival (DSS) is defined as time elapsed until death due to the disease or last contact. Deaths within postoperative 1 month were not regarded as death due to the disease.
Patients were followed up with pelvic examination, abdominal ultrasound, complete blood count, and biochemistry profile at quarter intervals for the first 2 years following adjuvant therapy, at semiannual intervals up to year 5, and at annual intervals thereafter. Chest X-ray is ordered at annual intervals or in case of clinical suspicion. Computed tomography of thorax and abdomen was performed in cases with possible recurrence. CA-125 was used for follow-up, although not routinely.
Statistics
Statistical analyses were performed using SPSS (SPSS, Inc., Chicago, IL), version 17.0. Patient characteristics of the conservative surgery group were compared with the definitive surgery group by chi-square test for the categorical parameters and by ANOVA Table Test for continuous parameters. Kaplan–Meier method was used for calculation of DFS and DSS. The cutoff for statistical significance was set at p-value <0.05.
Ethics approval
This study was approved by the Etlik Zubeyde Hanım Training and Research Hospital Ethics Committee.
Results
Sixty-nine patients with stage I-II MOGCTs were available for analyses. Median age of the study group was 21 years (range; 12–40 years). Main symptom was abdominal pain and 36 patients presented with this complaint. An incidental adnexal mass was found in 10 patients during routine examination. Median tumor size was 150 mm (range, 20–300 mm). Thirty-five patients had stage IA disease, 4 patients had IB, 15 patients had IC, 5 patients had IIA, and 1 patient had stage IIC disease. In addition, stage could not be determined in nine patients, who were regarded as stage I since no sufficient data were available.
Thirty-one (45%) patients had dysgerminoma and 38 patients had nondysgerminoma germ cell tumors. Of these, 12 (17.3%) patients had yolk sac tumors, 17 (24.6%) patients had immature teratoma, 4 (5.8%) patients had mixed germ cell tumor, 1 (1.4%) patient had choriocarcinoma, 1(1.4%) patient had embryonic carcinoma, 1 (1.4%) patient had gonadoblastoma, and 1 (1.4%) patient had malignant struma ovarii.
Malignant cells were present in 5 of 54 patients who had peritoneal cytology data. The ovarian mass lesion was ruptured in 12 patients. Of these, three had preoperative ruptured mass and nine patients had intraoperative iatrogenic rupture. Tumor rupture data were not available for 11 patients. The tumoral mass had adhesions to surrounding tissues in 16 patients. While tubal involvement was found in four patients, uterine serosal involvement was observed in three patients. Nineteen patients manifested ascites. Three patients with gonadoblastoma had bilateral tumors in both ovaries and conservative surgery was performed for both sides. The disease in contralateral ovary was managed with cystectomy in those two patients. Pathology of the lesion in contralateral ovary was a biopsy-proven dysgerminoma.
Fifty-one patients underwent lymph node dissection and 33 patients with unilateral tumors underwent contralateral ovarian biopsy. Fifty-six patients were treated with conservative surgery, while definitive surgery was required for 13 patients. Two patients required rectosigmoid resection to achieve maximal cytoreduction. While maximal cytoreduction was ensured for 67 patients, surgical outcome was optimal for 1 patient and suboptimal for 1 patient. Clinical and surgical pathological factors for patients are presented in Table 1.
BEP, Bleomycin + Etoposide + Cisplatin
Patients with fertility-sparing surgery and patients who had definitive surgery were similar regarding surgical pathological factors and adjuvant therapy usage (Table 2). Patients who had definitive surgery were older than patients with fertility-sparing surgery. Mean age was 21.7 years (range; 12–40 years) in the group of conservative surgery and 27.3 years (range; 18–39 years) in the group of definitive surgery (p = 0.020).
Patients with dysgerminoma and nondysgerminoma showed no significant differences in demographical, surgical, and pathological factors, except adjuvant therapy usage and tumor rupture (Table 3); 51.6% of patients with dysgerminoma received adjuvant therapy compared with 75% of patients with nondysgerminoma germ cell tumors (p = 0.047). Ruptured tumors were significantly more common in patients with nondysgerminoma germ cell tumors (24% vs. 4.2%; p = 0.046).
Forty-three patients received adjuvant chemotherapy. Of these, 31 patients received the bleomycin + etoposide + cisplatin (BEP) protocol. Three cycles of BEP protocol were given to 18 patients, while 13 patients received 4 cycles. Median number of chemotherapy cycles was five for other platinum-based regimens (range; 2–6). Two patients received adjuvant pelvic radiotherapy.
Median follow-up period was 65 months (range; 3–273 months) and recurrence was found in four patients (5.8%). Median time to recurrence was 11.5 months (range; 7–15 months). One patient recurred in pelvis lymph nodes, one patient had para-aortic lymphatic recurrence, and one patient had liver parenchyma metastasis. Recurrence localization data were not available in one patient. All patients with recurrent disease were diagnosed with having dysgerminoma. Three patients had conservative surgery and one patient had definitive surgery. No residual disease was achieved at initial surgical procedures of patients except one patient with optimal cytoreduction (Table 4). Five-year DFS was 94% in the entire cohort. This rate was 94.9% for stage I and 83.3% for stage II (p = 0.215).
Surgery type (conservative surgery vs. definitive surgery) and lymphadenectomy (performed vs. not performed) were insignificant for the recurrence (Table 5). However, surgical outcome (maximal vs. optimal and suboptimal) and type of tumor (dysgerminoma vs. nondysgerminoma) determined the recurrence-free interval (Figs. 1 and 2). Five-year DFS was 95.2% for patients who achieved maximal cytoreduction, but the corresponding rate was 50% for patients whose surgical outcome was optimal or suboptimal (p = 0.001). Recurrence was observed 7 months after optimal cytoreduction was achieved, while no recurrence was noted for patients with suboptimal outcome of surgery in 34-month follow-up. Tumor type was dysgerminoma for those two patients who failed maximal cytoreduction. Five-year DFS was 86.5% and 100% for patients with dysgerminoma and patients with nondysgerminoma, respectively (p = 0.021). Fertility-sparing surgery did not increase the likelihood of recurrence in this group of patients. Five-year DFS was 94.3% for patients who underwent fertility-sparing surgery, while the corresponding rate was 92.3% in the definitive surgery group (p = 0.758).
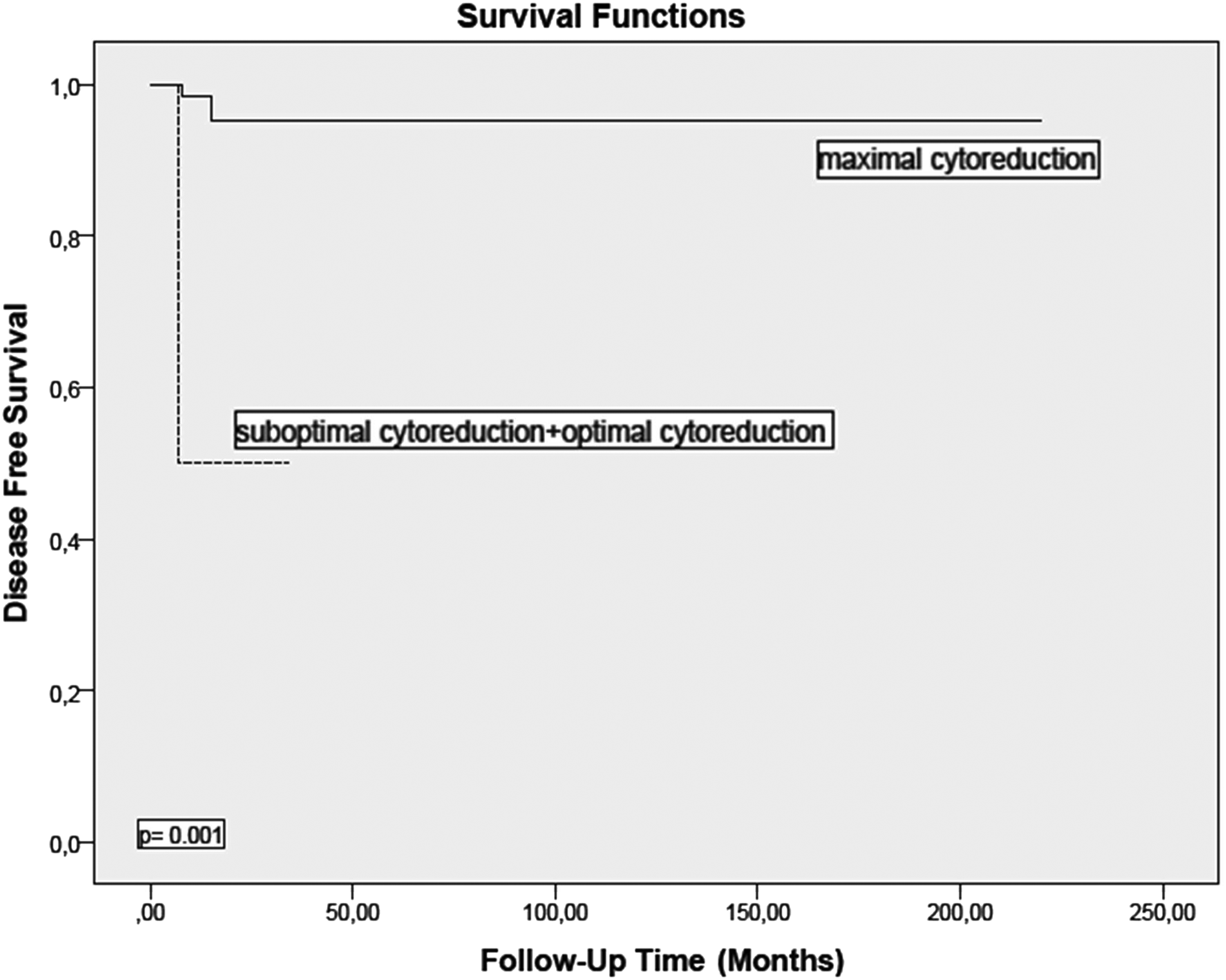
The effect of surgery type on disease-free survival.
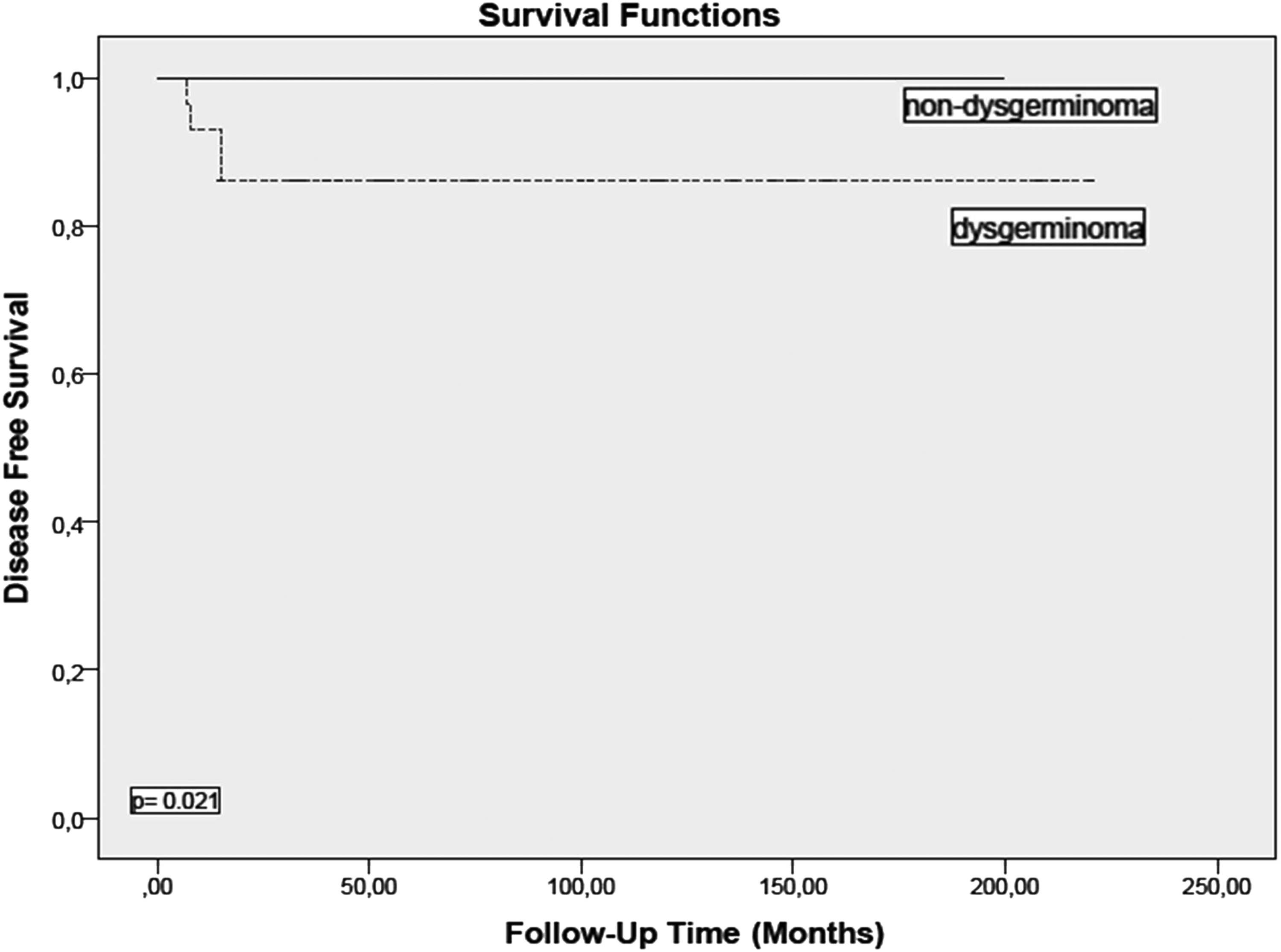
The effect of tumor type on disease-free survival.
Discussion
Fertility-sparing surgery became the standard of care in patients with malignant germ cell tumors of ovary after the introduction of platinum-based chemotherapy and the documentation of high chemosensitivity of these tumors to platinum.7–9
Park et al. studied MOGCTs in pediatric and adolescent age groups of all stages and observed that 5-year DFS was 85.5% and 5-year overall survival was 97% for the fertility-sparing approach. Authors observed that recurrent disease correlates with complete surgical staging, lymphadenectomy, lymph node metastasis, stage, tumor type, peritoneal cytology positivity, and adjuvant chemotherapy. 13 Ali Husaini et al. studied histological tumor type of dysgerminoma—all stages were included—and found that oncologic outcomes did not vary between patients who underwent conservative surgery or definitive surgery. Authors found that adjuvant chemotherapy extended only DFS, but not DSS (p = 0.034). 14 In our study, which included only patients with stage I/II MOGCTs, we also observed that surgery type (conservative surgery vs. definitive surgery) did not influence the oncologic outcomes. In our study, 5-year DFS was 92.3% for the definitive surgery group and 94.3% for the conservative surgery group (p = 0.758).
It is not clear whether lymphadenectomy should be included in surgical treatment of patients with MOGCTs. Kleppe et al. conducted a review on risk of lymph node involvement in clinical stage I and II MOGCTs and reported that lymphatic metastasis was present in 10.9% of patients (n = 103/946) and this rate was 18.1% (n = 40/221) for patients with dysgerminoma. 15 Kumar et al. evaluated patients with MOGCTs who underwent lymphadenectomy and demonstrated lymph node metastasis in 18.1% of patients (n = 111/613) and 28% of patients with dysgerminoma (n = 69/244). 16 Since our study population included surgically staged patients with only stage I and II disease, we could not report any lymphatic metastasis at initial surgery. However, two patients in our study had recurrent disease in the lymph nodes. Recurrence was located at the para-aortic region in one patient and sigmoid colon, rectum, and pelvic lymph nodes in the other patient (Table 4). Both patients with nodal recurrence underwent systematic lymphadenectomy in their initial surgery, and pelvic and para-aortic lymphadenectomy was performed for both patients. The number of lymph nodes excised was 33 for the pelvic region and 19 for the para-aortic region in the first patient. Number of retrieved lymph nodes was not available for the other patient. Similarly, Lin et al. observed recurrence in three of seven patients who were clinically staged as stage IA. 17 While two patients had isolated para-aortic nodal metastasis, the other patient had both pelvic and para-aortic nodal recurrent disease. Although the propensity of early stage MOGCTs to recur in lymph nodes seems to indicate the necessity of lymphadenectomy, it is not clear how lymphadenectomy should be performed (complete vs. sampling). In our study, lymphadenectomy was performed in 74% of patients (n = 51/69). However, addition of lymphadenectomy to the surgical procedure did not improve the DFS.
Cicin et al. observed that nondysgerminoma histology was associated with an increased risk of recurrence in patients with MOGCTs who had conservative surgery. In the dysgerminoma group, 1 recurrence was found in 36 patients, while 10 recurrences occurred in 34 patients of the nondysgerminoma group (p = 0.002). In addition, overall survival decreased from 97% in patients with dysgerminoma to 60% in patients with nondysgerminoma (p < 0.001). 18 Authors also showed residual tumor after initial treatment was correlated with overall survival in the nondysgerminoma group. Overall survival was 70% for patients with no residual tumor; however, overall survival was 25% in the presence of residual tumor (p = 0.015).
Meisel et al. reported that ovarian dysgerminomas had better DFS compared with other histological types of MOGCTs. Three-year DFS was reported as 89% and 73% for mixed germ cell tumors and immature teratomas, respectively (p = 0.044). 19 Our study differs from Meisel's that dysgerminoma was associated with poor prognosis regarding DFS. Five-year DFS was 86% and 100% in dysgerminoma and nondysgerminoma, respectively (p = 0.021). This fact can be explained by clinical and surgical differences between our patients with dysgerminoma and nondysgerminoma. Stage II disease was more frequently found in patients with dysgerminoma, although not statistically significant. Diagnosis was dysgerminoma for two patients who failed maximal cytoreduction and one of them developed recurrence 7 months after surgery. However, most remarkable difference between two types of tumors was adjuvant chemotherapy. Significantly more patients with nondysgerminoma received adjuvant chemotherapy (75% vs. 51.6%; p = 0.047).
Since high chemosensitivity is observed in germ cell tumors, aggressive surgery is still debated.10–12 Liu et al. compared patients who were clinically assessed during surgery for comprehensive surgery (unilateral salpingo-oophorectomy, complete lymphadenectomy, total omentectomy) or unilateral salpingo-oophorectomy (assessment of peritoneum, omentum, and retroperitoneal lymph nodes, biopsying, complete removal of all visible tumors) and no significant difference was found regarding 5-year DFS. Authors found that 5-year DFS was 87% for the comprehensive surgery group and 97% for the unilateral salpingo-oophorectomy group (p = 0.115). 11 On the contrary, Lin et al. evaluated patients with MOGCTs from all stages and showed that surgical staging (unilateral salpingo-oophorectomy, omentectomy, retroperitoneal biopsy, peritoneal washing, peritoneal biopsy) decreases recurrence in comparison with clinical staging. This finding was also evident in patients with stage IA disease (p = 0.026). 17 In our study, maximal cytoreduction correlated with improvement in the DFS. Five-year DFS was 95.2% in the group of maximal cytoreduction, while DFS decreased to 50% for patients who failed maximal cytoreduction.
Solheim et al. investigated the influence of platinum-based chemotherapy cycles on fertility in patients who underwent fertility-conserving surgery. They compared patients who received ≤3 cycles of platinum-based chemotherapy with those who received >3 cycles. Infertility rate was significantly higher for patients who received >3 cycles of platinum-based chemotherapy (p = 0.040). Pregnancy was achieved in 13 of 20 patients who received ≤3 cycles of platinum-based chemotherapy, while 6/15 patients who had >3 cycles of chemotherapy became pregnant (p = 0.036). 20 Pectasides et al. conducted a review on ovarian germ cell tumors and reported that three cycles of BEP (bleomycin + etoposide + cisplatin) are required for patients with no residual tumor, while bulky residual tumor requires four cycles of BEP. 3 Cumulative doses of platinum may negatively influence fertility due to gonadotoxic effects, and more cycles of platinum-based chemotherapy may lead to ovarian dysfunction.21,22
The most important physician-controlled factor to protect our patients against high cumulative doses of cisplatin seems to ensure maximal cytoreduction. Thus, patients will be exposed to less platinum in adjuvant chemotherapy. In conclusion, while maximal cytoreduction not only decreases recurrence and improves survival, it also suppresses the negative influence on the ovarian function by ensuring that lesser cycle of platinum-based chemotherapy is used. In addition, since risk of recurrence is higher for patients who cannot achieve maximal cytoreduction, and there is a possibility for platinum-based chemotherapy for treatment of relapse in such patients, maximal cytoreduction at initial surgery may have a more important role for preservation of fertility in case of recurrence. In conclusion, fertility-sparing surgery is not simply protecting the uterus and at least one ovary physically, but it does mean protecting the ovarian function by decreasing the need for adjuvant platinum.
The main limitation of this study is its retrospective nature. On the other hand, advantages arise out of the fact that it is a single-center study and all surgeries are carried out by the same surgical team.
In conclusion, fertility-conserving approach is safe in early stage MOGCTs. However, maximal cytoreduction should be targeted in this group of patients, without conceding the fertility-conserving approach. On the other hand, development of chemotherapy options with less gonadotoxic effects, but equal or stronger efficiency compared with platinum-based chemotherapy, will certainly facilitate management of this patient group.
Footnotes
Author Disclosure Statement
No competing financial interests exist.