
Abstract
Psychological support services for adolescent and young adults (AYAs) with cancer are moving online and are increasingly peer based. It is unclear whether online service delivery impacts critical therapeutic elements such as collaborative patient–therapist rapport and group cohesion. AYA cancer survivors (N = 39) participating in a six-week online cognitive-behavioral therapy group program—“Recapture Life”—rated their perception of therapeutic alliance and group cohesion. Participant-rated alliance and group cohesion were high throughout the program, and therapist-rated participant openness, trust, and motivation strengthened over time. The findings provide further support for the expansion of AYA cancer support services to the online domain.
Background
A
With this shift toward the online delivery of psychological support services, it is essential to consider the implications of online group-based formats for intervention efficacy, the quality of the therapeutic relationship, and consumer and therapist satisfaction with care. 7 While the effectiveness of one-on-one internet-delivered psychological interventions has been well-examined across various settings, 8 a number of gaps in the literature remain. Although there is robust evidence of the efficacy of group psychological interventions for mood and anxiety disorders and distress related to medical conditions, 9 there have been very few rigorous trials of group psychotherapy delivered online. 10 The state of the evidence with regards to online group therapy for adolescents is similarly scant.11–13
Furthermore, the nature of therapeutic processes in the online space warrants consideration in determining the acceptability of online models of psychosocial care. 14 Therapeutic alliance, defined as the collaborative element of the patient–therapist dyad, is one process that has been studied across numerous face-to-face interventions and is an important predictor of stronger eventual improvements on outcomes (e.g., distress).15,16 In group therapy “group cohesion”, the quality of interpersonal processes between group members and between group members and therapist(s) is also an important predictor of positive intervention outcomes. 17 The clinical processes that underpin the development of good therapeutic working relationships, and foster positive therapeutic group environments, are critical to understand beyond their impact on outcomes; however, individuals who feel more positively about their relationship with their group therapist and group members experience greater insights through the course of interventions and are less likely to drop out of interventions prematurely. 18 These processes therefore play a critical role in supporting individuals' long-term engagement with psychosocial care. Characterizing whether these processes can be successfully navigated within online interventions, and clarifying the potential empirical and conceptual overlap between alliance and cohesion in group settings, is striking a gap in the current evidence base.
Therapeutic processes warrant particular consideration in AYA psychosocial cancer care. For developmental reasons, AYAs may perceive greater stigma related to mental illness compared to younger and older patients and are less likely to engage with support services. 4 AYAs' preferences for peer-support models of care 4 justify an examination of the translatability of alliance and group cohesion factors to the online setting. Therapeutic groups (led both by professionals and laypersons) are a highly prevalent model of psychosocial support for individuals with cancer, yet with little data on how and how well they work.19,20 We need to better understand these processes as the capacity to develop rapport with a therapist and to perceive mutually supportive relationships with peers within a group context which may therefore form the ‘gateway’ to AYAs' ability to engage with, and benefit from, support in the longer term.
It is also crucial to take into account therapist perspectives. Although there is growing evidence of therapists' positive attitudes toward online therapies, 21 ongoing concerns, including managing distress and risk remotely 22 and liability/confidentiality issues, 23 may impact therapist satisfaction and perceptions of clinical processes. For example, therapists may rate lower therapeutic alliance in one-on-one videoconferencing-based services compared with traditional face-to-face therapy. 24 There is a need for further research into therapists' perception of clinical processes in online groups.
Our team recently completed a trial of an online evidence-based cognitive-behavioral group intervention for AYA cancer survivors, which aimed to improve their quality of life and reduce distress in the early months posttreatment. 25 Using data from this trial, we examined in this study participant-reported therapeutic alliance and group cohesion, levels of therapist comfort, and therapist-perceived group cohesion. We investigated whether ratings changed over the course of the intervention and the relationship between participant-rated alliance and group cohesion scores.
Methods
Study design
This report presents an analysis of therapeutic process data from a now completed phase-II randomized-controlled trial (RCT) “ReCaPTure LiFe” (
Participants and procedures
Ethical approval was obtained from the South Eastern Sydney Local Health District Human Research Ethics Committee. Participants recruited to the Recapture Life trial were aged between 15 and 25 years, less than 12 months off-treatment, and not experiencing severe mental health problems (e.g., suicidality) at study intake. Informed consent was obtained from all participants. Participants were recruited from hospital sites around Australia and from charitable organizations targeted at supporting young people with cancer.
Measures of therapeutic process
In addition to a battery of validated measures assessing intervention efficacy, 25 participants completed four items from the Working Alliance Inventory (WAI)26,27 after the first and last modules of the intervention. The WAI has established validity and reliability in AYAs as young as 11 years. 28 Participants rated the extent to which ‘My group leader understands what I am trying to accomplish’, ‘I am confident of my group leader's ability to help me’, ‘I feel that my group leader appreciates me’, and ‘I believe that the way we are working with my concerns is correct’ (Scale: 1 = “doesn't correspond at all” to 7 = “corresponds exactly”). Participants also completed four items from the well-validated California Psychotherapy Alliance Scale for Group (CALPAS-G), 29 which indexes group cohesion, after the last module of the intervention: ‘When important things came to mind, how often did you find yourself keeping them to yourself rather than sharing them with the group?’, ‘Do you feel accepted and respected by the group members for who you are?’, ‘How much did you find yourself thinking that the program was not the best way to get help with your concerns?’, and ‘How much did the group members help you gain a deeper understanding of your concerns?’ (Scale: 0 = “not at all” to 6 = “very much so”). Participants were informed that the therapist would not see their ratings.
After each module, therapists rated their level of comfort running the group and their clinical impression of group cohesion across six domains as follows: rapport, openness, mutual trust, peer-to-peer discussion, motivation, and engagement (on a 10-point scale, with higher scores indicating more positive appraisals). Items were purposively developed for the study.
Statistical analysis
Data were analyzed using SPSS Version 24.0. Descriptive statistics was calculated for all measures included in the study. A series of planned paired-samples t-tests (p < 0.05) were used to calculate whether there was a significant change in participant-rated therapeutic alliance (measured by the WAI) and therapist-rated impressions of group cohesion between the first and last module of the intervention. Taking into account participants' scores at the commencement of the intervention, partial correlations (p < 0.05) were conducted between participant-rated therapeutic alliance (WAI) and participant-rated group cohesion (CALPAS) at the last module of the intervention.
Results
Thirty-nine participants completed the Recapture Life intervention (M age: 20.5 years, SD = 2.9, range = 15–26 I ; 51% female), representing a response rate of 17.4%. II On average, participants were 8 months posttreatment (SD = 4.6, range = 1–19 III ) for various cancers (51.3% blood; 38.5% solid; and 10.2% brain/central nervous system).
After the first module of the intervention, participants strongly endorsed all therapeutic alliance items, and these ratings remained high throughout the 6-week program (p > 0.05; Table 1).
Paired-samples t-tests.
N = 39, 12 groups; items from the Working Alliance Inventory rated on a scale from 1 to 7.
Items rated on a scale from 1 to 10.
Statistically significant.
In terms of group cohesion participants at least moderately agreed that they ‘shared important things’ (Item 1; M = 4.8, SD = 1.3) and ‘felt accepted and respected…’ (Item 2; M = 5.0, SD = 1.2) and that the program was the‘…best way to get help…’ (Item 3; M = 5.4, SD = 1.0) and ‘…helped them gain a deeper understanding…’ (Item 4; M = 4.0, SD = 1.4; Fig. 1).
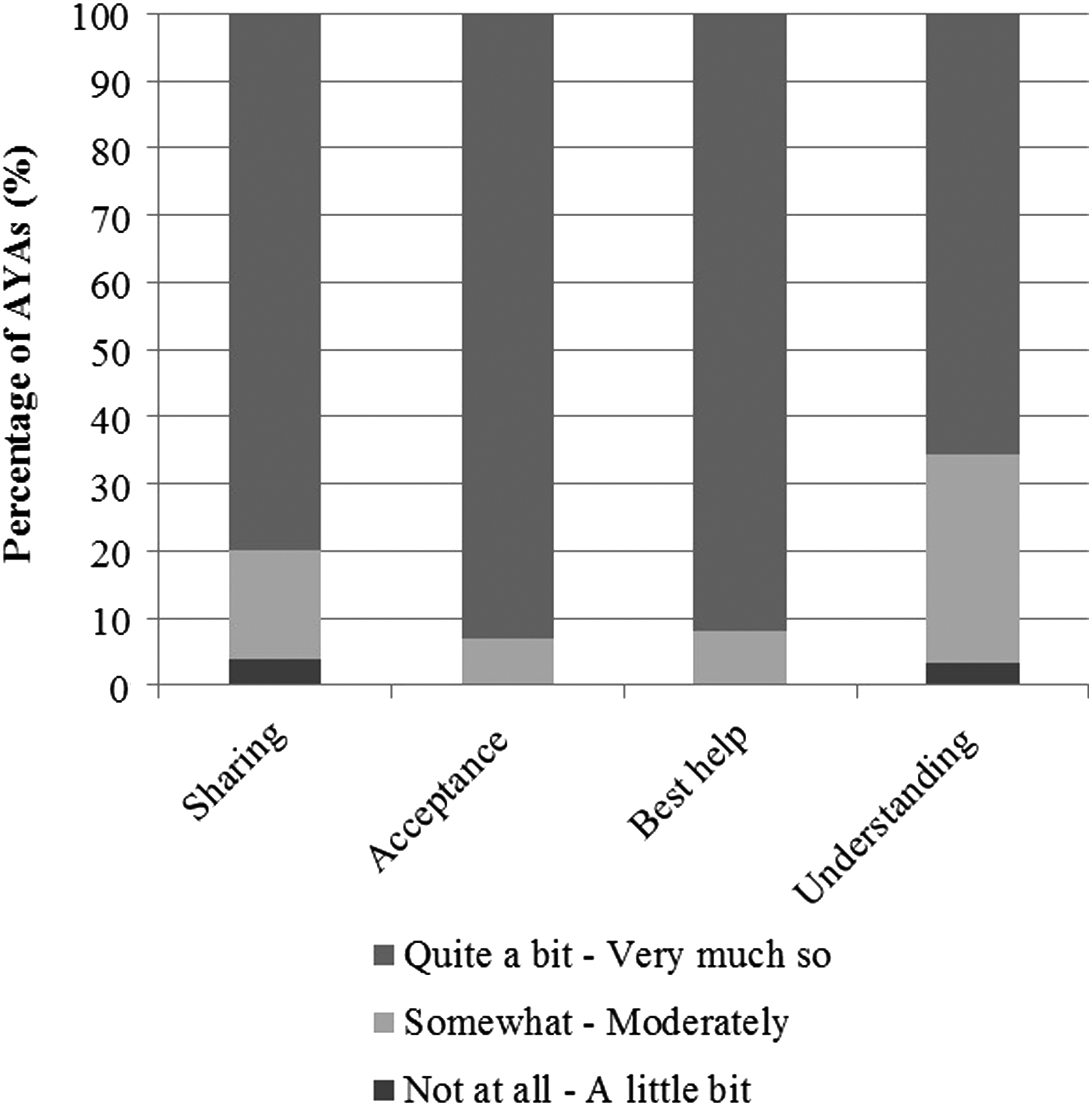
Participant CALPAS-G rating of group cohesion (Items 1–4) after the final module of Recapture Life.
Therapist ratings of participant openness were significantly stronger at the last module of the intervention compared to the first [t(37) = 2.91, p < 0.05], as were therapist ratings of participant trust [t(37) = 2.89, p < 0.05] and motivation [t(37) = 3.39, p < 0.05]. Therapist ratings of their own comfort running the group also increased, although not significantly [t(37) = −1.89, p = 0.066] (Table 1).
At the last module of the intervention, participants' ratings of their comfort sharing important things with the group were significantly correlated with confidence in their group leader's ability to help (r = 0.73, p < 0.001), perceived appreciation by their group leader (r = 0.67, p < 0.01), and belief in the “correctness” of the intervention for addressing their concerns (r = 0.72, p < 0.01). Participants' feelings of acceptance and respect by other group members were significantly correlated with confidence in their group leader's ability to help (r = 0.54, p < 0.05) (Table 2).
p < 0.05.
p < 0.01.
p < 0.001.
WAI, Working Alliance Inventory.
Discussion
As evidence-based AYA cancer support services move online and become increasingly peer based, it is paramount to consider the impact on therapeutic processes. 22 Our results indicate that it is possible to build strong therapeutic alliance with AYAs in an online, group-based CBT intervention early on and to maintain this across the course of the program. Alliance scores were equivalent to, or even higher, than reported ratings in face-to-face interventions with AYAs. 28 Furthermore, AYAs in this program generally felt supported and accepted by the group and held positive views about the peer-support model as a setting to express their concerns, with group cohesion scores similar to face-to-face group interventions in adults. 30 AYAs' desire for peer support is well-documented, 4 and these results further indicate that AYAs with cancer feel comfortable receiving this type of support online. The translatability of important group-based therapeutic processes to the online domain adds an additional layer of evidence to efficacy research. Demonstrating that it is possible for these important interpersonal processes to unfold in positive ways in the online realm validates it as a medium for both engaging AYAs in psychosocial support and facilitating the development of supportive peer- and therapeutic relationships. The present study's findings add to a growing body of work supporting the potential for online services to deliver effective, gold standard, and age-appropriate care for AYAs with cancer.
While AYAs reported consistently positive working alliance ratings over the six weeks of the program, therapist ratings of some important alliance and group cohesion factors showed a significant strengthening over time. Although starting high, by the end of the program therapists rated participants as more open, more trusting, and more motivated. Ratings also indicated that the therapists felt more comfortable running the intervention after the final module. The improvements in therapists' ratings may reflect their increased confidence in facilitating the online intervention with repeated exposure. It may be that clinicians' hesitance around using videoconferencing is due to a lack of experience, which is a modifiable barrier to implementing online interventions in practice.
It is important to consider the present findings in the context of the Recapture Life therapists' training and experience with videoconferencing. The finding that the therapists' perceptions of the therapeutic working relationship and their confidence delivering a high-quality online service were positive throughout the intervention, and significantly strengthened over time, underscores the broad potential for online service delivery for psychologists with limited experience with videoconferencing and who may be early in their careers. For emerging AYA clinical services, such online service provision may be viewed as a supplement to the ‘menu’ of traditional, face-to-face clinical services delivered, as a means of expanding access to high-quality care. 31
This study contributes a novel examination of therapeutic alliance and group cohesion among AYA cancer survivors. Significant correlations between some items of the WAI and CALPAS indicate a possible relationship between concepts of alliance and cohesion in group psychotherapy contexts, an idea worthy of further examination. It seems that participants who perceived their group as cohesive also felt a strong alliance with their therapist. As others have suggested, it may be that the participant–therapist relationship is not a distinct concept from the myriad of other relationships within the group psychotherapy environment. 9 However, all results should be interpreted with the caveat that the sample size was small and the measure assessing therapists' ratings of group processes was purposely designed, limiting its potential validity. Nevertheless, this study suggests that therapeutic alliance translates well to the online space. Given the complexity of establishing gold standard, age-appropriate AYA clinical services that has been reported internationally,3,5,6 these findings provide further impetus for the movement of AYA cancer psychological support services to the online domain. A future goal is to evaluate how these data relate to efficacy outcomes from the broader Recapture Life RCT.
Footnotes
Acknowledgments
The authors acknowledge the support of the wider Recapture Life Working Party, including Prof. Phyllis Butow, Prof. Richard Bryant, Dr. Antoinette Anazodo, Ms. Kate Thompson, Ms. Lucy Holland, Prof. Susan Sawyer, Dr. Belinda Barton, Ms. Belinda Matigian, Ms. Lyndal Gray, Dr. Michael Osborn, Ms. Meg Plaster, and Dr. Marianne Phillips. The authors also thank Ms. Helen Wilson for her assistance with the preparation of this article and acknowledge the contribution of Emma Doolan. The Recapture Life study was cofunded by a beyond blue and Cancer Australia project grant (ID: 1022868). Ursula Sansom-Daly is supported by an Early Career Fellowship from the Cancer Institute of New South Wales (ID: 14/ECF/1-11) and an Early Career Fellowship from the National Health and Medical Research Council of Australia (APP1111800). Claire Wakefield is supported by a Career Development Fellowship from the National Health and Medical Research Council of Australia (APP1067501) and an Early Career Development fellowship from the Cancer Institute of NSW (ID:11/ECF/3–43). The Behavioral Sciences Unit is proudly supported by the Kids with Cancer Foundation, by the Kids Cancer Alliance, as well as a Cancer Council New South Wales Program Grant PG16-02 with the support of the Estate of the late Harry McPaul.
Author Disclosure Statement
No competing financial interests exist.