
Abstract
Multiple osteolytic lesions are usually associated with metastatic involvement of the bone; however, metabolic bone diseases should also be included in the differential diagnosis. In this study, we describe a case of primary hyperparathyroidism (
Introduction
P
Herein, we report a case of PHPT presenting with full-blown osteolytic lesions that was initially confused with metastatic bone involvement.
Case Report
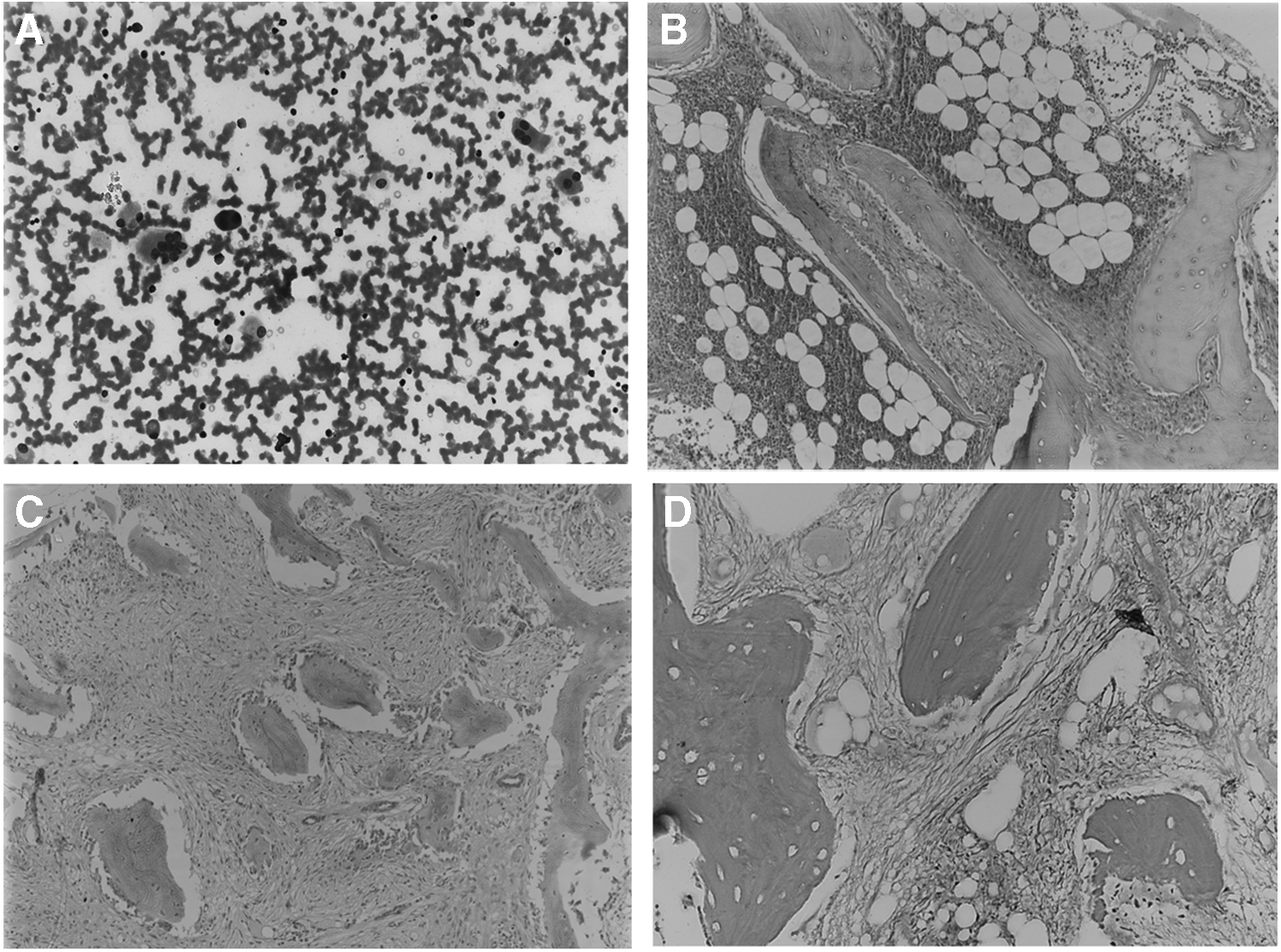
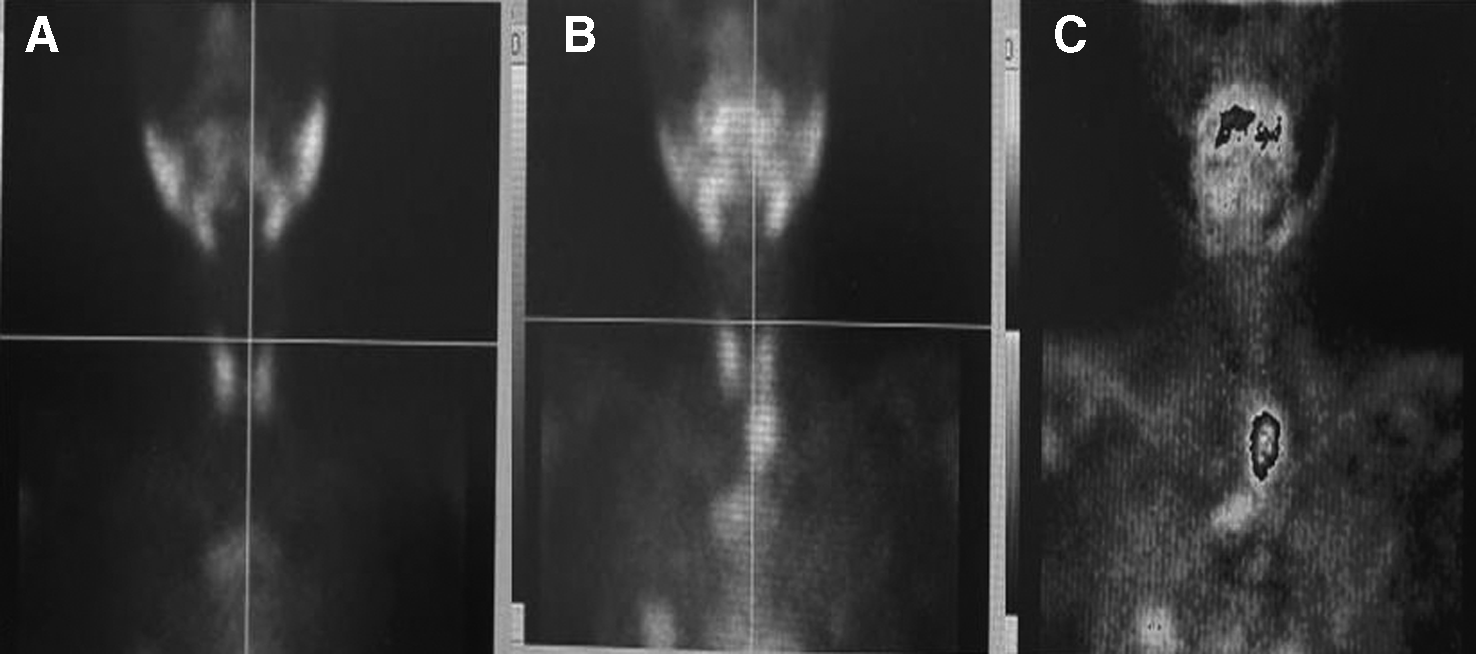
A 19-year-old boy was referred to our hospital with a history of fracture to the neck of the right femur due to a fall on the floor. He consulted an orthopedic surgeon, and intramedullary fixation (IF) was done. He presented with persistent right hip pain and inability to walk. The radiograph of the pelvis showed multiple lytic lesions, and a provisional diagnosis of metastatic bone malignancy was made. In our hospital, the patient was investigated further. The complete blood count showed hemoglobin, 9 gm/dL; total leukocytes count, 12,000/mm3; and platelets, 260,000/mm3. Biochemical investigations revealed markedly raised calcium, 17.6 mg/dL (8.6–10.2 mg/dL); and raised alkaline phosphatase, 806 U/L (40–129 U/L). Vitamin D levels done were low, 12 ng/mL (30–60 ng/mL). The tumor markers, namely CA15.3, CA19.9, CA72.4, CEA, and AFP, were negative. Ultrasonography of the whole abdomen showed multiple dense calcific foci in renal pyramids of both kidneys. Magnetic resonance imaging (MRI) of the pelvis revealed fracture of the femoral neck with IF in situ and normal right hip joint space. The observed bones showed diffuse osteopenia with multiple variable-sized expansile lytic lesions involving bilateral iliac bones, inferior and superior pubic rami, and acetabuli. Edema was seen in surrounding soft tissues and adjoining lateral compartment muscles. Serum protein electrophoresis was normal, and Bence Jones protein was negative. The patient was planned for bone marrow procedure to rule out a possibility of metastatic carcinoma. The bone marrow aspirate was diluted and showed numerous osteoblasts, osteoclasts, and few peripheral blood elements only (Fig. 1A). The bone marrow biopsy section showed a few areas of normal trilineage hematopoeisis along with a few areas of extensive paratrabecular and intertrabecular fibrosis with prominent blood vessels (Fig. 1B, C). There was rimming of woven bone by osteoblasts and prominence of osteoclasts. Reticulin stain showed grade 3 fibrosis (Fig. 1C). In view of hypercalcemia, nephrocalcinosis on ultrasound scan, and bone marrow findings, a possibility of hyperparathyroidism was suspected. The parathyroid hormone (PTH) was highly raised, 2300 pg/mL (0–70 pg/mL). Further, sestamibi parathyroid scintigraphy scan was done, which revealed uptake at the level of the left inferior pole of the thyroid gland, suggestive of parathyroid adenoma (Fig. 2). While he was under investigation, he had another pathological fracture of the right femur shaft, for which he was managed with immobilization cast. During his follow-up at the in-patient clinic, hypercalcemia of the patient improved with intravenous hydration and furosemide. The patient was planned for surgical excision of the parathyroid adenoma.
Discussion
Hypercalcemia in association with lytic bone lesions raises a suspicion of malignancy. Malignancy-related hypercalcemia is common in certain types of tumors such as lung carcinoma and plasma cell myeloma (PCM). In malignancy-associated hypercalcemia, disease is usually symptomatic and hypercalcemia is discovered during evaluation. Occasionally, hypercalcemia may be due to an occult tumor. Hypercalcemia in an adult who is asymptomatic is usually due to
Skeletal changes can occur in both
Hypercalcemia in association with lytic bone lesions as seen in our case raised the suspicion of a metastatic bone involvement. The key screening tools in such cases are the medical history, routine laboratory tests, imaging techniques, and a bone marrow examination to rule out a primary tumor. 5 In our case, biochemical investigations, namely the tumor markers such as CEA, CA125, AFP, and CA19.9, were negative and only serum calcium levels and alkaline phosphatase levels were raised, 17.6 mg/dL (8.6–10.2 mg/dL) and 806 U/L (40–129 U/L), respectively. The PTH was highly raised, 2300 pg/mL (0–70 pg/ml), and a diagnosis of hyperparathyroidism was made that was confirmed by sestamibi scan.
PHPT is a generalized disorder of calcium and phosphate and bone metabolism due to increased secretion of PTH.
6
Increased PTH leads to hypercalcemia and reduced or normal phosphate levels. There is a great variation in the manifestations. Patients may present with multiple signs and symptoms, including recurrent nephrolithiasis, peptic ulcers, mental changes, and, less frequently, extensive bone resorption.
2
The most common cause is a solitary parathyroid adenoma, and surgical excision of the abnormal parathyroid tissue is the definitive therapy.
7
In addition, orthopedic intervention can be necessary in case of pathologic fracture or extensive cortical involvement. The classic imaging features of advanced
Hematological manifestations are less known in PHPT. Anemia has been recognized as a complication of PHPT in 5%–30% of the individuals in various series.12–14
Anemia in PHPT is multifactorial, and marrow fibrosis is one of the causes. The underlying mechanism of bone marrow fibrosis is likely to be related to elevated levels of intact PTH, which promotes the release of cytokines (interleukin-6 and tumor necrosis factor-alpha) that have a stimulatory effect on marrow fibroblasts.
15
The bone marrow biopsy can show varying degrees of paratrabecular and intertrabecular fibrosis with a moderate increase in vascularity of the marrow. Macroscopic cysts and hemosiderin-laden macrophages can also be seen, and this final stage is referred to as osteitis fibrosa cystica
16
; however, this is very rare nowadays in view of earlier diagnosis and treatment. These features are important to remember as bone marrow biopsy is occasionally performed to investigate either hypercalcemia or radiographic lesions suspicious of metastatic carcinoma in patients with unsuspected severe hyperparathyroidism.17–19
There are no specific peripheral blood or bone marrow aspirate abnormalities associated with
Surgery is indicated for all patients with symptomatic
Conclusion
This case report emphasizes the value of accurate diagnosis in cases with osteolytic lesions, especially in youth and adolescents where the causes of metastatic involvement are quite different from an adult or old aged person. The bone marrow biopsy finding of fibrosis should invoke suspicion and a correlation with the clinical and biochemical findings to arrive at the diagnosis. The metabolic bone diseases such as PHPT should be kept in mind before considering the possibility of metastatic bone involvement as the treatment of the two is completely different.
Footnotes
Acknowledgments
The authors wish to thank senior residents and technical staff of the laboratory for their sincere work.
Author Disclosure Statement
No competing financial interests exist.