
Abstract
Purpose:
Fertility preservation discussions with pediatric and adolescent cancer patients can be difficult for clinicians. This study describes the acceptability of a fertility clinician decision support system (CDSS).
Methods:
A cross-sectional study of clinicians at The Royal Children's Hospital, Melbourne. Participants were trained on CDSS purpose, contents, and use. A survey captured the perceived benefits and weaknesses of the CDSS.
Results:
Thirty-nine clinicians participated. Over 90% felt the CDSS aims and format were clear, and understood the components. Over 80% felt it would enable adherence to clinical pathways, policy, and standards of care.
Conclusions:
The CDSS provided significant perceived benefits to oncofertility care.
Introduction
T
International bodies recommend the discussion of fertility risks and preservation options before commencing cancer treatment as part of routine care.4,5 However, clinicians involved in these discussions report a number of challenges, making these consultations difficult. 6 Many of these difficulties stem from a dearth of center-specific multidisciplinary guidelines, pathways of care, and clinician resources to facilitate these discussions. 6
There are additional complexities surrounding the provision of fertility care in the pediatric and adolescent cancer setting. Numerous clinical teams are involved in the care pathway and require coordination. Several preservation options with differing safety and efficacy profiles may be available to each patient. 7 Postpubertal oocyte or sperm salvage is of proven efficacy. However, procedures for prepubertal females (ovarian tissue cryopreservation) have only rarely resulted in birth of live progeny, and procedures for prepubertal males (testicular tissue cryopreservation) are currently considered experimental in humans, although positive outcomes are reported in animal species. 7 In addition, fertility discussions and decisions to pursue or forego a preservation procedure are time sensitive and need to occur soon after diagnosis and before the commencement of gonadotoxic therapy. Therefore, clinicians need to balance the provision of fertility care with the need for timely diagnosis, disease staging, and commencement of treatment.
In 2013, The Royal Children's Hospital (RCH), Melbourne, developed a fertility preservation program, with discussions and preservation procedures offered under three levels of governance: (1) institutional governance as a novel technology; (2) research governance for collection of safety and efficacy data; and (3) clinical ethics governance for individual cases. 8 To facilitate fertility discussions, a fertility toolkit was introduced, containing a suite of resources for clinicians, including instruction booklets, checklists, referral forms, reference information, and information resources for families. 9
Clinicians involved in fertility care were surveyed to evaluate the perceived impact of the toolkit on fertility discussions and satisfaction with the toolkit after use. 9 Survey results were encouraging, with 100% of respondents indicating they would use and promote the toolkit, and 100% satisfied or extremely satisfied with fertility discussions using the toolkit. 9 However, only 63% of clinicians were satisfied with the toolkit itself. The most common reasons for dissatisfaction were missing documents, complex organization of the documents within the toolkit, and the perception that the volume of written information could overwhelm clinicians. 9
To address these issues and further facilitate fertility discussions, the format and content of the toolkit were revised and simplified into a clinician decision support system (CDSS), which was then integrated within the hospitals electronic medical record (EMR). The RCH introduced an EMR system in 2016. The EMR provides improved access to information, supports clinical decision-making, and improves patient safety.
CDSSs are computer applications designed to aid clinicians in making decisions in patient care. 10 They offer providers actionable, patient-specific recommendations or guidelines for clinical practice at the point of care. CDSS can include a variety of tools and interventions such as computerized alerts and reminders, clinical guidelines, clinical pathways, order sets, patient data reports, documentation templates, diagnostic support, and clinical workflow tools. 11
The aim of this study was to evaluate clinician responses before the introduction of the fertility CDSS and their perceptions on its acceptability and efficiency in facilitating FP discussions.
Methods
This cross-sectional study was conducted at The RCH, Melbourne. Research ethics approval was obtained through the RCH Human Research Ethics Committee (HREC 36016).
Materials
Clinician decision support system
The CDSS was created by the Fertility Preservation Taskforce at The RCH, Melbourne, a collaborative association of oncologists, fertility specialists, gynecologists, and pediatric providers. The CDSS had two main components:
An electronic clinical oncofertility pathway, in the form of two comprehensive and interactive flowcharts, one each for male and female patients (Supplementary Figs. 1 and 2; Supplementary Data are available online at www.liebertpub.com/jayao). The pathways were color coded to differentiate responsibilities of the departments involved in care, and contained clear descriptions of roles and responsibilities of each department from diagnosis through long-term follow-up. E-links provided access to more detailed guidance, including infertility risk tables, direct links to patient information handouts, and consent forms. “Alert” boxes were included containing important best practice recommendations. Step-wise guidance within the EMR, directing clinicians through the oncofertility pathway. This included (1) a systematic grouping of relevant steps and orders to be worked through, providing guidance through a fertility discussion; (2) prompts for referrals to relevant hospital departments; and (3) template fertility discussion notes, so that all relevant information is documented. The template contained “soft stops,” where the clinician was prompted to provide clinical information if it was not given, or to justify a clinical decision. The clinician could override these prompts, so there was no disruption to clinical care. “Hard stops,” prompts that cannot be overridden, were not included.
Procedure
This study was carried out between March and September 2016. All clinical staff involved in oncofertility care at the RCH, Melbourne, and collaborating centers were invited to participate. Clinical staff were excluded if they were only involved in fertility care for non-oncology patients. All participants attended education sessions where they were familiarized with the CDSS and trained on its concept, contents, and use.
Participants completed a questionnaire adapted from a previous study, consisting of 26 questions divided into three sections: (1) demographic information; (2) involvement in fertility care; and (3) understanding of and perceived benefits and weaknesses of the CDSS. 9 Responses were recorded on a five-point Likert scale ranging from “strongly agree” to “strongly disagree,” or with free text. Results were summarized and reported as a descriptive study.
Results
Thirty-nine of a potential 63 (61.9%) recipients responded. Ten were nursing staff, 22 medical staff, and 7 allied health or supportive care; 31 (79.5%) were female; 35 (89.7%) were from The RCH and 4 (10.3%) from collaborating centers; and 28 (73.7%) had been involved in fertility care for less than 10 years. This is representative of the intended participant group. The denominator changed during the survey as some participants did not answer certain questions or responses were not applicable.
Twenty-eight (72%) always, often, or sometimes discussed the impact of cancer treatment on fertility. No significant difference in discussion frequency was seen between male and female respondents. Seven (17.9%) had involvement in over 100 fertility discussions; 10 (25.6%) were involved in 11 to 50 fertility discussions; and 22 (56.4%) were involved in less than 10 fertility discussions. Most participants (33/35, 91.7%) indicated that they would like to improve their ability to discuss fertility and provide resources to families.
Thirty-seven (94.9%) participants indicated that they felt the aims of the CDSS were clear, with 30 (83.3%) agreeing that it was created to encourage clinicians to discuss fertility with their patients. Most participants (37/38, 97.4%) reported an understanding of the overall fertility pathway and CDSS components; 33/36 (91.7%) understood the steps specific to their role; 36/39 (92.3%) stated the CDSS format was clear; 32/38 (84.2%) liked or very much liked the CDSS design; 29/35 (82.9%) thought the CDSS was of appropriate length, with 6 (17.1%) indicating it was too long; and 31/35 (88.6%) indicated that they were willing to always or often use the CDSS for fertility discussions, with 25/26 (96.2%) willing to lead a fertility discussion using the CDSS.
Figure 1 describes the participants' opinion of the expected impact of the CDSS on clinical practice. Most (32/37, 86.5%) felt the CDSS would enable adherence to consistent clinical pathways, and 30/37 (81.1%) felt it would enable adherence to policy and standards of care. However, only 17/37 (45.9%) felt it would help improve clinician satisfaction in the area.
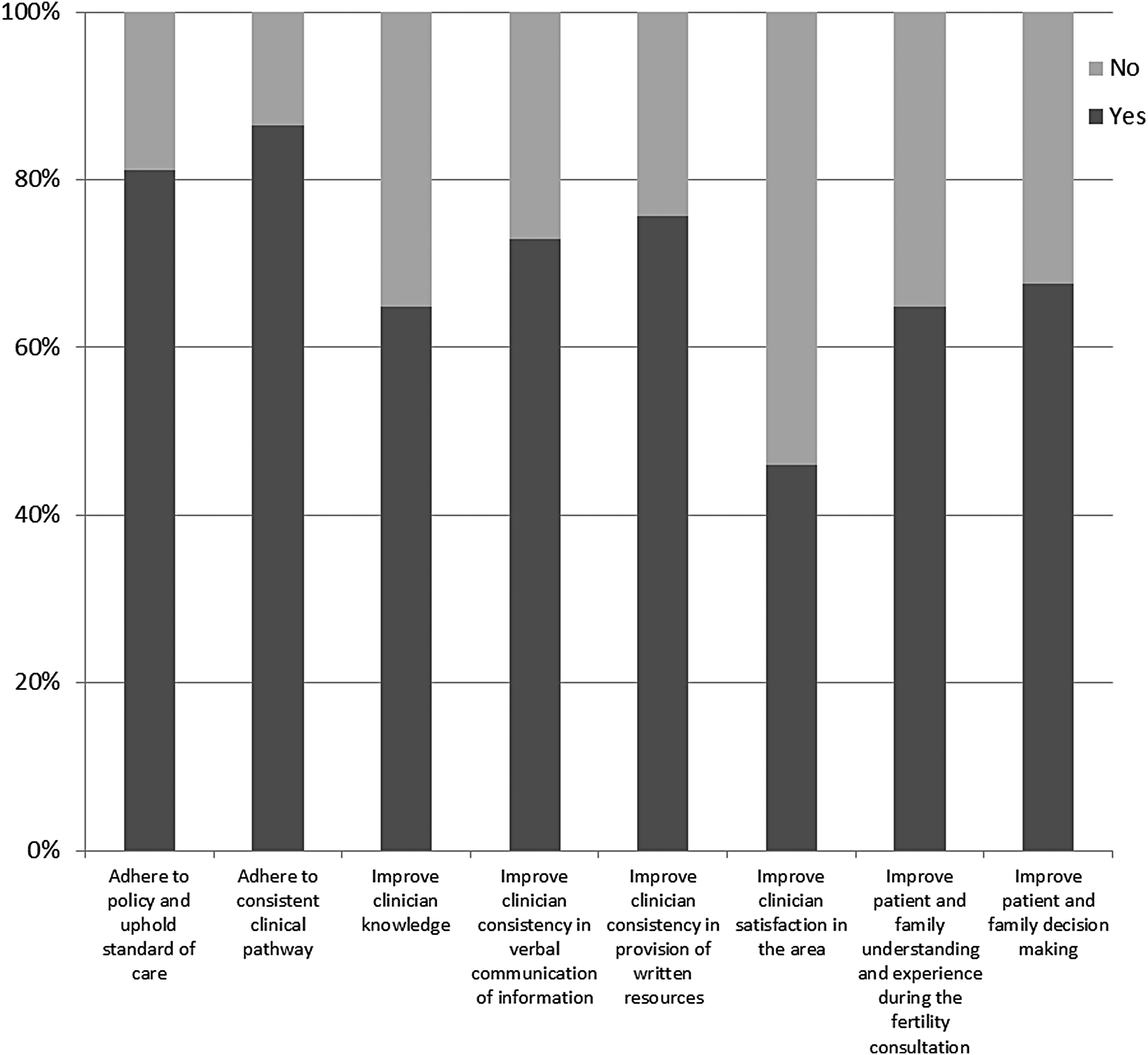
Participants predicted impact of CDSS on clinical practice. CDSS, clinician decision support system.
Twenty-one participants provided free text comments about the strengths and weaknesses of the CDSS. The most commonly raised perceived strength (7/21) pertained to the access to documentation, with comments reporting that the CDSS would make it “easier to find documents in a timely manner” and fertility pathways and guidance being “more accessible.” The ease of use of the CDSS was raised (6/21), with comments suggesting the CDSS was “easy to navigate,” “streamlined” and “user-friendly.” The functionality of the CDSS was seen as a “clear advantage” and would “facilitate reminders and discussion.” The most commonly reported perceived weakness was the “incomplete integration of the CDSS” into EMR (3/21), with some components of the CDSS only accessible outside of the EMR system.
Discussion
This is the first study investigating the usability and acceptance of a pediatric oncofertility CDSS. At The RCH, fertility care is provided in the setting of a pediatric center and involves a large multidisciplinary team to provide an ethical service for patients receiving gonadotoxic treatment. In this setting, fertility care is complex and time critical.
Pediatric providers have to consider complex issues around future fertility for young patients having gonadotoxic treatment. Specific guidelines recommending discussion with families around the impact of such treatment on fertility have been published by a variety of organizations.4,12 However, there are still inconsistencies with recommendations around the provision of care. 13 Calls have been made for the development of center-specific multidisciplinary pathways of care and clinician resources to facilitate fertility discussions.14–16 We developed a CDSS containing interactive oncofertility pathways and step-by-step guidance through fertility discussions.
Overall success of a CDSS is largely based on user satisfaction and attitudes toward the system. 17 An evaluation of a CDSS before full-scale implementation is recommended. 17 The overall usability of the CDSS was measured in a variety of ways, including an understanding of components, order, clarity of format, appearance, and length. Over 90% of participants reported an understanding of the overall CDSS components and the department-specific components, and felt that the format was clearly presented. Fewer participants felt that the CDSS was of appropriate length, with 17.1% indicating it was too long, despite the CDSS being a direct representation of the steps necessary to provide optimal fertility care. This likely reflects the desire of some participants to only view the CDSS in the context of their specific role, while others preferred a big picture view.
Results were overwhelmingly positive regarding the use and promotion of the CDSS, with 88.6% of participants reporting they would use and/or promote it, and 96.2% willing to lead fertility discussions using the CDSS, suggesting a high level of acceptance among participants. The majority of participants predicted the CDSS would have a positive impact on clinical care, as indicated by an anticipated increased adherence to consistent clinical pathways, policy, and standards of care. This is consistent with literature suggesting that the use of an electronic system decreases usability problems and increases adherence to guidelines. 18
Research suggests that access to documentation, ease of access, and functionality are significant barriers to the success of a CDSS.19,20 Participants in this study perceived the strengths of this CDSS to include all three factors, indicating clinicians feel that the CDSS can be successfully implemented.
The introduction of a fertility CDSS may result in some unintended negative consequences. Poor CDSS design may result in disruptions to clinical care, clinical errors, and clinicians feeling their autonomy is limited. In addition, clinicians may become deskilled if they rely solely on the CDSS to prompt the different aspects of fertility care. Therefore, while clinician resources and support tools may streamline fertility service delivery, they should be designed so that the care provided is not process driven, but requires individualized discussion and decision-making. The introduction of a support system should not obscure the fact that many fertility options are considered experimental at this point in time.
This study had several limitations. This was a small study and only 61.9% of those involved in oncofertility care participated. However, the study group was representative of the intended participant group. In addition, this study only reports on the acceptability and expected benefits of a CDSS. Although an important aspect of CDSS development is evaluating its acceptability before implementation, clinician feedback after CDSS implementation would be of interest. 17 Furthermore, the CDSS was designed and evaluated in an institution with an EMR and an established fertility team. While the overall system has the potential for use in other centers, aspects of the CDSS may require modification to meet specific institution requirements.
Results of this study show support for the proposed CDSS, with indications of overall acceptability and feasibility. However, due to the known barriers to successful CDSS implementation and the complexities of pediatric oncofertility care, monitoring of clinician feedback after implementation is necessary. The next stage in CDSS development is to survey oncofertility providers after CDSS clinical use. In addition, the development of an electronic tool that can deliver individualized care plans specific to oncofertility discipline and patient would be an important next phase of development.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.