
Abstract
Purpose:
Survival rate of childhood cancers is now reaching 80% overall. However, early or late complications related to surgery, chemotherapy, and radiotherapy remain at a high rate and greatly increase the risk of late mortality. The objective of this study is to assess the autonomic nervous system (ANS) activity, measured through heart rate variability indices in childhood cancer survivors compared with healthy controls.
Methods:
This prospective study included 51 long-term childhood cancer survivors diagnosed before 15 years of age between 1987 and 1992 and controlled for age and sex with healthy volunteers.
Results:
We observed a significant increase in spontaneous heart rate (beats per minute) (67 ± 10 vs. 60 ± 10, p = 0.001), and all the studied parameters showed a significantly altered ANS activity in cases compared with healthy controls. In both groups, the main cofactors of dysautonomia (tobacco, drugs, cannabis, estro-progestative pills, alcohol, limited physical activity) were analyzed without any significant difference. The effect of cancer treatments received was not analyzed due to the small number of participants.
Conclusion:
The results showed a significant ANS dysfunction in childhood cancer survivors compared with healthy controls and suggested the value of autonomic screening to underscore and possibly quantify the effect of the cancer treatments in a larger cohort. This evaluation could lead to the recommendation to increase physical activity, the most efficient way known to improve ANS activity, as already shown in other pathologies (breast cancer).
Introduction
Autonomic Nervous System (ANS) activity is a strong and precise regulator for many biological functions. The sympathetic and the parasympathetic arms, which regulate the autonomic function, are physiologically linked through a reciprocal influence. The disequilibrium due to an excess in sympathetic activity equals a reciprocal dysautonomia. 1 The parasympathetic activity is protective, whereas disturbance in ANS activity induces highly unfavorable vascular disorders, particularly severe clinical events such as stroke, myocardial infarction, and cardiac heart failure2,3
Heart rate variability (HRV) analysis is a validated and commonly used method to evaluate ANS status in healthy and pathological subjects.4,5 This quantification of beat-to-beat variations provides indices that are representative of sympathetic and parasympathetic activity as well as the ratio between sympathetic and parasympathetic activities, the so-called autonomic balance. Using such analysis in the general population, three longitudinal studies (ARIC, ZUTPHEN, and FRAMINGHAM)6–8 underlined the predictive value of decreased ANS activity for death, mainly cardiovascular. The same predictive value was attributed to a decrease in ANS after stroke or myocardial infarction. 9 More specifically, in animal models, increased sympathetic activity and decreased parasympathetic activity 10 are associated with a higher risk of sudden cardiac death.8,9,11,12 In particular, reduced HRV is independently associated with an increased risk of myocardial infarction, congestive heart failure, death from cardiovascular disease, and total mortality.8,9,11 Experimental evidence also suggests that the ANS is involved in the development of vascular atheroma and occlusion. 13
These factors of cardiovascular disease, associated with an inflammatory response, determine the occurrence of an early hypertension, as shown in the PROOF study. 14 Circulating inflammatory markers are associated with a simultaneous decrease in parasympathetic activity. 15
Survival rate of childhood cancers is now reaching 80% overall. However, early or late complications related to surgery, chemotherapy, and radiotherapy remain at a high rate and greatly increase the risk of late mortality. 16
In Europe, late effects after childhood cancer potentially affect about 500,000 adults. 17 These late effects are diverse and may include educational, behavioral, and social problems, and physical health effects, such as second primary tumors (present in around 4% of survivors), secondary leukemia (in around 0.2% of survivors), cardiovascular disease (as an effect of radiation and chemotherapy agents), and effects on fertility and growth. 18
There are few reports of HRV in childhood cancer survivors.19–21 Because of the potential risk related to radiation on ANS or cardiotoxic chemotherapy agents they received, we decided to explore the ANS function of childhood cancer survivors.
Many survivors have impaired cardiometabolic health status and are at increased risk of long-term cardiovascular disease. The lack of a strong relationship between estimates of cardiometabolic health and cancer type or specific treatments reflects the pathophysiological heterogeneity of individual risk factors. 22
Thus, one can hypothesize that a population treated for childhood cancer might develop ANS impairment despite long-term cure. This population may integrate the cumulated risk factors as shown by the incremental decrease of parasympathetic activity with the increase of metabolic syndrome criteria.22,23
The objective of this study is to assess the ANS activity, measured through HRV indices in childhood cancer survivors, compared with healthy controls.
Methods
Cases
The SALTO-1 study is a prospective population-based cohort study of cancer survivors (excluding leukemia) diagnosed before 15 years of age between 1987 and 1992 in a French administrative area (Auvergne and Rhône-Alpes) started in 2011. We did not include survivors of leukemia in our cohort because another French study has analyzed the long-term follow-up of these cases (LEA Cohort). Four hundred eighty-one patients were eligible. In this project, we describe the medical and psychopathological status of childhood cancer survivors, in particular thanks to a consultation performed by a pediatric oncologist and/or an internist. Details of this study were published earlier. 24
Five months after the first inclusion in SALTO-1, an ancillary study titled SALTO-ANS started. Then, each patient included in the SALTO-ANS study wore a 24-hour Holter electrocardiogram (ECG) to be sure that the whole sleep period would be registered. The patients also noted their bedtime and wake-up time to confirm the start and end of the sleep period.
We excluded patients presenting neurological or cardiac congenital defects, suffering from cardiac arrhythmias or an absence of sinus rhythm, having undergone general anesthesia within the preceding week, or currently using drugs that have known cardiac effects.
Controls
The control population was based on healthy voluntary subjects from the general population of the same French administrative area with the same exclusion criteria. Compared with the cases, controls were age and sex matched.
All cases and controls signed an informed consent. Recordings were read by an independent team blinded to the subjects' identity. Each record was numbered and anonymized (first two letters of the name and first letter of the first name).
Blinding procedures could be removed, after a cardiological opinion, in the event of unexpected discovery of rhythmic abnormalities, which may be life-threatening. In this case, there was provision for immediate communication of the examination data to the patient's referring physician.
Self-questionnaires
Cases and controls completed a self-questionnaire, adapted to the gender, with the same questions regarding physical activity, tobacco, drugs, alcohol, general anesthesia, current medical treatment, cardiac disease, diabetes, physical activity level, night work, oral contraceptive use (women), including questions from the population physical activity questionnaire (POPAQ) 25 and the Quality of Life MOS SF-36 Health Survey version 2 scale.26–28
HRV analysis
The ANS capacity was assessed by 24-hour cardiac recordings, to be sure to record the whole sleep period, with HRV analysis.4,5 For the analyses, to avoid differences in daily activities, we deleted all the awake period data to keep only the sleep period data. The ECG trace sampled at a frequency of 512 Hz was extracted from NeuroCoach© ambulatory system (NBATechno, Saint-Cyprien, France) by using the built-in export data tool. All calculations were performed with HRV analysis software 29 developed with Matlab 9.0.0 R2016a (The Mathworks, Inc., Natick, MA). First, each R peak was detected on the ECG to provide the RR interval series. The missing beats, isolated extra-systoles, and artifacts were corrected by using a spline cubic interpolation as suggested in the HRV guidelines. 4 The RR signal was then resampled at 2 Hz to obtain a regular sample base-time. Periods presenting with successive artifacts during more than 10 seconds were discarded from the analysis. 29
HRV was estimated by various methods: Time-domain, geometrical, and frequency domain analysis provide indices representing (1) overall autonomic cardiac modulation (standard deviation of normal-to-normal intervals [SDNN], total spectral power [Ptot]), (2) mainly short-term HR variation regulated by parasympathetic activity (percent difference between adjacent normal RR intervals greater than 50 ms; pNN50), square root of the mean of the sum of the squared differences between adjacent normal RR intervals (rMSSD), and high frequencies (HFs), (3) long-term HR variation regulated by both parasympathetic and sympathetic cardiac activity in the low frequencies (LFs) band, and (4) normalized indexes such as the LF/HF ratio, LFnu, and HFnu used to examine this relationship. Non-linear indices such as Poincaré-plot, fractality, and entropy reflect RR signal complexity due to the feedback loops that impact the cardiac function in opposition to random or periodic signals, which represent a loss of complexity. The Poincaré plot is a graphic tool used to visualize a series of RR intervals with SD1 and SD2 calculated as the SD of the distances of the RR intervals from the y = x line and the y = −x + 2 × mean (RR) line, respectively. The detrended fluctuation analysis (DFA) is used to measure the degree of self-similarity (fractality) of the RR signal by calculating the average amount of RR fluctuation at different bin sizes.
The Shanon entropy and its derived indices (conditional entropy, corrected conditional entropy, normalized corrected conditional entropy) measure the regularity and complexity of patterns of different lengths. Entropy is high when the patterns are identically distributed and decreases if some patterns are more likely. For a complete description of HRV indices, readers can refer the wide bibliography in the field.4,5,29 The HRV analyses were performed over the night to avoid variations originated by daily environmental factors. We also verified the absence of sleep apnea syndrome by using very low frequency index (VLFI) of HRV. 30
Statistical analysis
Questionnaire data were computerized by using EpiData software (EpiData, version 3.1; The EpiData Association, Odense, Denmark) and analyzed, as well as cancer survivor's characteristics, with SAS software (SAS, version 9.2; SAS Institute, Inc., Cary, NC).
HRV indices data were reported as means ± SD for continuous variables, and as counts and percentages for categorical variables. Data were analyzed by using Statview 5.0 (SAS Institute, Inc.).
Differences between patients and controls for demographic characteristics, risk factors, and HRV indices were assessed by using Chi-square test or Fisher's exact test for qualitative data and Student's t-test for qualitative variables.
The threshold for statistical significance was set at p < 0.05.
Results
Among the 150 patients who participated in the long-term follow-up consultations,24,31 51 (27 women) participated in an ANS evaluation (Fig. 1). Indeed, the ancillary SALTO-ANS study started 5 months after the SALTO-1 study when 98 patients had already come to the consultation. Characteristics of those 51 cases did not significantly differ from the global population of SALTO-1 participants (Table 1). One survivor of a cerebral tumor with resultant moderate mental difficulties participated in the consultation but did not respond to the self-questionnaire.
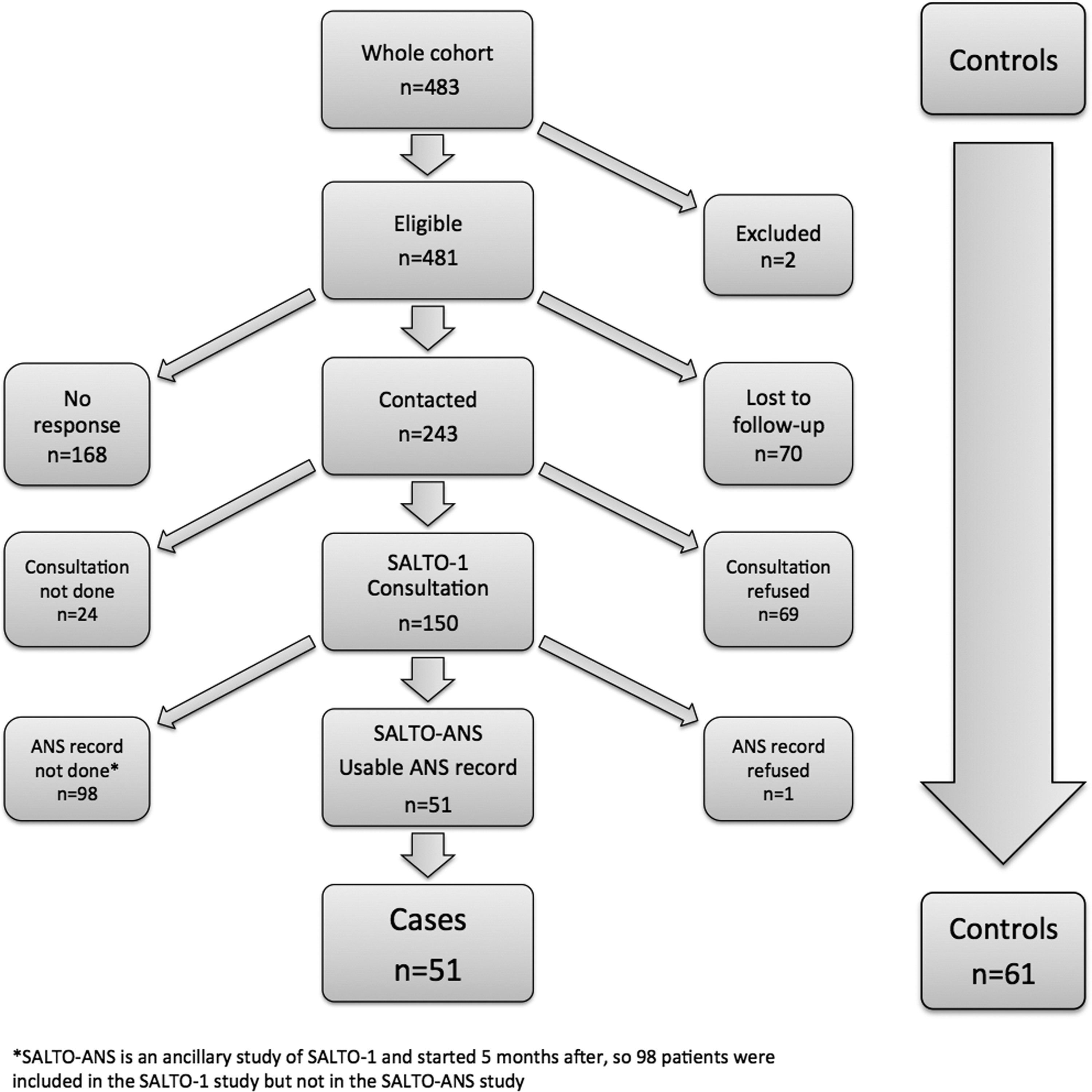
Flow chart of the cases and the controls.
Characteristics of the Whole Cohort of Childhood Cancer Survivors Who Participated in the First Long-Term Follow-Up Study (SALTO-1) and the Fifty-One Patients Who Had an Autonomic Nervous System Record
Other tumors including retinoblastoma, hepatic tumors, germinal and gonadic tumors, carcinoma.
CT, chemotherapy; CSRT, cranial and/or spinal radiotherapy; TBI, total body irradiation; SD, standard deviation; ANS, autonomic nervous system.
Sixty-one controls also participated in the study with a mean age of 28.0 ± 5.2 years. Forty-eight (27 women) of them completed a self-questionnaire, with no significant differences regarding risk factors compared with the 50 cases (Table 2).
Frequency of the Risk Factors in Cases and Controls (at Time of the Study)
nb, number.
Blinding procedures have been removed for one patient for whom sleep apnea had been detected by the Holter examination.
HRV indices
As an example, HRV analysis arising from an SALTO subject (left panel G1) and a control subject (right panel G2) are presented in Figure 2.
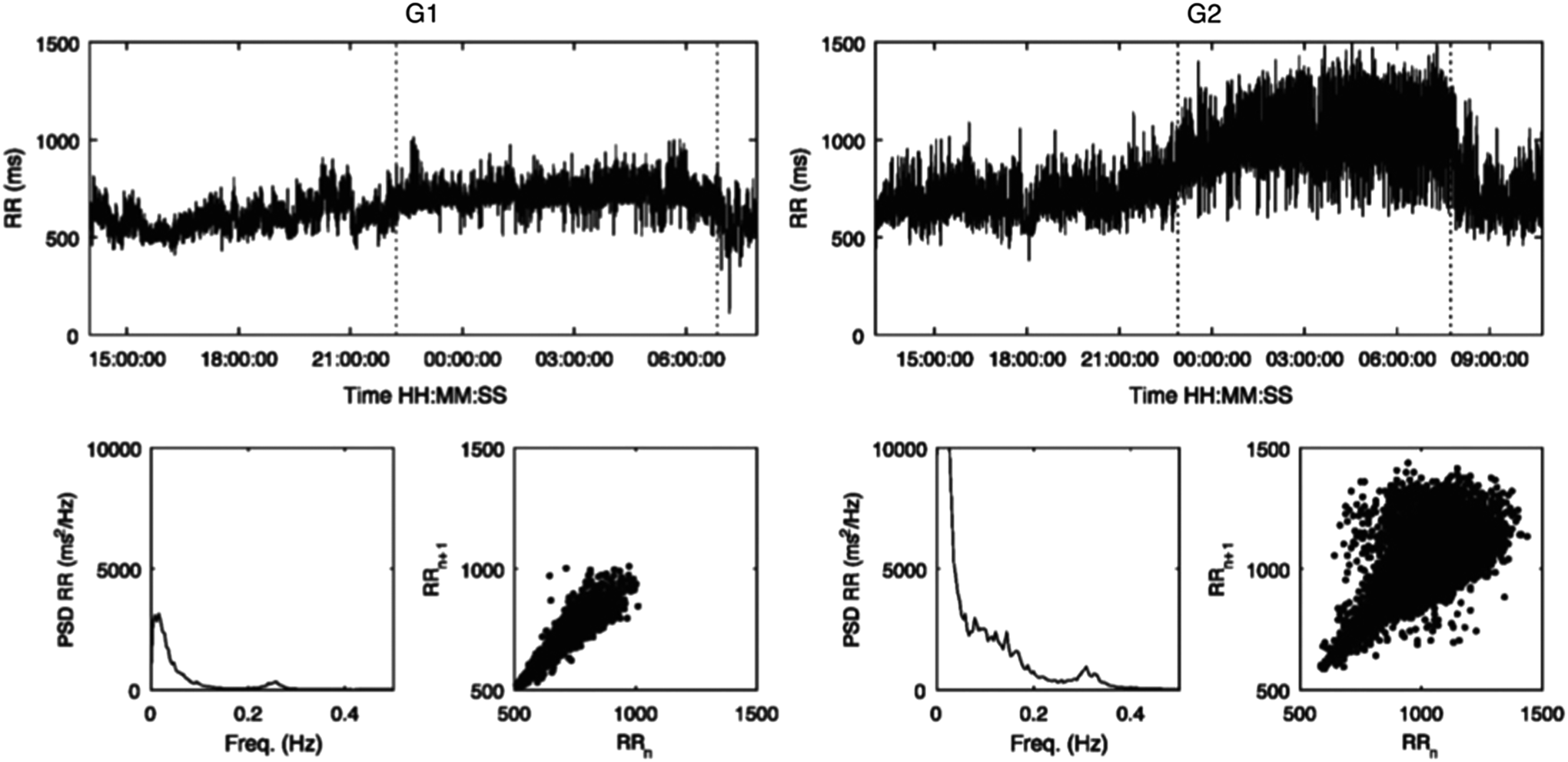
Heart rate variability analysis arising from an SALTO subject (left panel G1) and a control subject (right panel G2). Upper panels: Evolution of 24-hour RR variability. The night period is situated between the two dotted lines. Lower panels: Power spectrum and Poincaré plot of the RR variability nocturnal periods.
The first analysis consisted of paralleling the linear and non-linear variations of the HRV indices in the two groups (G1 [cases, n = 51] vs. G2 [controls, n = 61]) (Table 3). We observed a significant increase in spontaneous heart rate (beats per minute) in G1 versus G2 (67 ± 10 vs. 60 ± 10, p = 0.001).
Heart Rate Variability Indices During Sleep Period of Cases and Controls
HR, heart rate; pNN50, percent difference between adjacent normal RR intervals greater than 50 ms; SDNN, standard deviation of normal-to-normal intervals; Ptot, total spectral power; SDANN index, calculated as the standard deviation of the mean of all normal RR intervals for 5-min segments, quantifies the changes in heart rate due to cycles shorter than 5 min; SDNNIDX index, calculated as the mean of the standard deviation of all normal RR intervals for all 5-min segments, quantifies the changes in heart rate due to cycles shorter than 5 min; VLF, very low frequency; LF, low frequency; HF, high frequency; rMSSD, square root of the mean of the sum of the squared differences between adjacent normal RR intervals; DFA, detrended fluctuation analysis; bpm, beats per minute.
For the time domain indices, we found in G1 a significantly lower SDNN value (96.1 ms ±30.9 vs. 108.6 ms ±27.3; p = 0.03), a significant decrease of pNN50 (24.2% ± 18.6 vs. 34.7% ± 21.4; p = 0.007), and rMSSD (47.4 ms ±22.5 vs. 63.3 ms ±29.7; p = 0.002). For the time domain indices, we found in G1 a significantly lower SDNN value (96.1 ms ±30.9 vs. 108.6 ms ±27.3; p = 0.03), a significant decrease of pNN50 (24.2% ± 18.6 vs. 34.7% ± 21.4; p = 0.007), and rMSSD (47.4 ms ±22.5 vs. 63.3 ms ±29.7; p = 0.002).
In the frequency domain, the overall spectral power of the spectrum was also lower in G1 versus G2 (Ptot = 2663 ± 1585 ms 2 /Hz vs. 4206 ± 2552 ms 2 /Hz; p < 0.001) regardless of the period analyzed.
The sympathovagal balance was unchanged with the same ratio LF/HF in the two groups; whereas we observed for G1 a decreased orthosympathetic activity in LF (752 vs. 1110 ms 2 /Hz, p < 0.001), and a decreased parasympathetic activity in HF (425 vs. 632 ms 2 /Hz, p = 0.004).
We also examined non-linear indices such as Poincaré-plot, fractality, and entropy, reflecting RR signal complexity due to the feedback loops that impact the cardiac function.
All the indices pointed out in G1 versus G2 a loss of complexity of the cardiac signal: decreased SD1 index representing short-term variability (33.8 ms ±16 vs. 45.1 ms ±20, p = 0.002) without significant modification of SD2 (reflection of long-term variability).
The indices used for fractal analysis also varied between G1 and G2 in the sense of a significant loss of complexity: HDFA from 0.94 to 0.91 (p < 0.001) whereas alpha1 and alpha2 (DFA) indices were unchanged.
In the same vein, the entropy that evaluates the regularity and complexity of models of different lengths of the RR signal decreased between G1 and G2: from 1.25 to 1.3 (p = 0.04) for approximate entropy and from 1.14 to 1.21 (p = 0.03) for sample entropy.
Finally, the acceleration and the deceleration capacity were significantly altered in the G1 group.
Discussion
These results showed a significant increase in spontaneous heart rate, and a decreased orthosympathetic activity and parasympathetic activity in comparison with the control population. To our knowledge, this was the first study to evaluate ANS function in a representative population of adult childhood cancer survivors (CCS). A strength of this study is that we evaluated in both groups the main cofactors of dysautonomia (tobacco, drugs, cannabis, estroprogestative treatment, alcohol, limited physical activity), 5 and no significant difference was observed. A limitation is that we did not evaluate stress or anxiety in controls, which are also cofactors of dysautonomia as described. 32 Other limitations of this study should be the absence of leukemia survivors in the sample, given that leukemia is one of the most common cancer diagnoses in pediatric patients, and the inability to examine the relationship between treatment/disease characteristics and dysautonomia because of the small sample size. Nevertheless, the detected difference of ANS values should be confirmed in a larger cohort.
In 1989, Hirvonen et al. described HRV reduction in nine children treated for leukemia during and after vincristine treatment (potential neurotoxic drug). 19 In 2002, Postma et al. 20 reported the results of longitudinal cardiac assessments at 9 and 14 years post-treatment in 29 long-term doxorubicin-treated bone tumor survivors. He found no deterioration of systolic dysfunction, but a progressive reduction of HRV. 20 After 27 years follow-up post-treatment, all HRV parameters decreased, leading to a sympathetic dominance, determining an increase in LF/HF ratio, associated to a progressive impairment of systolic and diastolic function. 21 Indeed, the Postma et al. 20 cohort concerns childhood and adult bone tumor survivors. We make the assumption that vinca alkaloids may alter long-term ANS. These drugs inhibit the ability of cancer cells to divide: Acting on tubulin, they prevent it from forming into microtubules, a necessary component for cellular division. Vincristine has been approved to treat acute leukemia, rhabdomyosarcoma, neuroblastoma, Wilm's tumor, Hodgkin's disease, and other lymphomas. The neurotoxicity is mostly distinguished by a peripheral, symmetric, varied sensory-motor and autonomic polyneuropathy. 33
Another group of chemotherapeutic agents such as the anthracyclines could be involved in the dysregulation of ANS. A meta-analysis has well defined all the mechanisms of cardiac toxicity of the anthracyclines. 34 In animal models, anthracyclines also induced nephropathy (focal segmental glomerulosclerosis and tubulointerstitial lesions), endothelial damage, and inflammatory process. Physical training before the doxorubicine injection reduced the renal damage induced by this drug. 35
Inflammation is a local, protective response to microbial invasion or injury. It must be fine-tuned and regulated precisely because deficiencies or excesses of the inflammatory response cause morbidity and shorten lifespan. According to Tracey, “cholinergic neurons inhibit acute inflammation that has qualitatively expanded our understanding of how the nervous system modulates immune responses.” 36 We hypothesize that some late effects observed in CCS could be consequences of such chronic inflammation.
A recent study analyzed the role of different types of treatment in long-term vascular mortality in 4227 French and British patients cured of childhood cancer. 37 After a median follow-up of 29 years, 23 deaths due to cerebrovascular disease had occurred. Patients with high-dose irradiation to the pre-pontine cistern area had a 17.8-fold (4.4–73.0) higher hazard ratio of death from cerebrovascular disease. This publication gave us the opportunity to explore ANS function in this population since, within the brain, ANS is regulated through the hypothalamus and the nucleus solitarii tractus in the brainstem. The nucleus solitarii tractus is located near the pre-pontine cistern area. Other ANS deleterious effects of cancer treatment may be present as 50% of these deaths occurred in patients who did not receive cerebral radiotherapy.
Considering such a potential dysautonomia in case of CCS, we may propose a therapeutic approach with two noninvasive therapies: physical activity and/or vagus nerve stimulation.
Physical activity is the main positive modulator of ANS activity. It is also established that physical activity improves cardiovascular health and prevents cancer, whereas it is a strong positive regulator of ANS activity.38,39 In response to a single session of physical exercise, we can observe, after a transient decrease, a rebound of parasympathetic activity over the pre-exercise value. 40 Thus, from rebound to rebound, the parasympathetic activity level can be considerably increased as shown in young people, 41 in sportsmen, 42 in the general population, 43 and in the elderly. 44 This parasympathetic activity obtained through exercise has been shown to reduce the risk of cardiac death in humans 44 as well as in animals. 45 We, thus, hypothesize that active patients should have less deterioration of their parasympathetic activity than sedentary ones, leading to a protective cardiovascular effect. 6
Another therapeutic approach could be the noninvasive and well-tolerated vagus nerve stimulation, which has been studied in 48 healthy participants. 46 This stimulation of the auricular branch of the vagus nerve, distributed to the skin of the ear, increased HRV, indicating a shift in cardiac autonomic function toward parasympathetic predominance. The same effects were observed in inflammatory chronic diseases such as Crohn disease, 47 or rheumatoid arthritis. 48 This may be an option for those who are unable to increase physical activity levels.
In conclusion, the value of such autonomic screening will underscore, and possibly quantify, the global health of CCS, which are particularly at-risk subjects. This easily feasible analysis of ANS could be an approach for personalized medicine while taking into account the risk factors related to the disease, allowing a patient own-evaluation of his risk factors, and then to manage a personalized care according to the individual risk factors and autonomic status.
This evaluation could also encourage CCS to introduce adapted physical activity and promote a better control of other dysautonomia risk factors.
Footnotes
Acknowledgments
The authors wish to express their sincere thanks to all the survivors who participated in this study and their families; association ADERPS (Saint-Etienne non-profit organization for the pediatric research development—University Hospital of Saint-Etienne—France) for financial support; Prof. Fernand Freycon, ex-president of ARCERRA; Prof. Jean Claude Barthelemy for helpful advice; Alejandra Estanislao for reading this publication's article; Audrey Loubier for help in entering data; and Pr. Dominique Plantaz, Pr. Jean-Louis Stephan, Pr. Justyna Kanold, Dr. Corinne Armari-Alla, Dr. Anne Pagnier, Dr. Didier Frappaz, Dr. Perrine Marec-Berard, Dr. Safia Khenifer, Dr. Sandrine Thouvenin, Françoise Odier, Sandrine Billet, Nathalie Gauthier, Pierre Métral, and Aurélie Chausset for work in each participant center.
Research Involving Human Participants and/or Animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
No competing financial interests exist.