
Abstract
Sighting a case of subcutaneous panniculitis-like T cell lymphoma (SPTCL) in cytology is very rare in a clinical scenario. Among the differential diagnoses (D/D) of a subcutaneous nodule undergoing fine needle aspiration cytology (FNAC), it is hardly considered in the list. The common D/D on cytology would be panniculitis or a non-SPTCL lymphoma. To make a correct cytological diagnosis, the pathologist has to meticulously observe the type of inflammatory infiltrate, their morphology, the intimate admixture of the fat lobules, and background necrosis or macrophages. This article describes the cytological picture, D/D, and the prognostic factors associated with SPTCL in a young male. He was suspected of SPTCL after FNAC and later confirmed on histopathology with specific immunomarkers. We do not recommend the confirmation of SPTCL on cytology however, we would like to stress that it can be picked up and differentiated from its mimickers on FNAC.
Introduction
Subcutaneous panniculitis-like T cell lymphoma (SPTCL) is a sporadic lymphoma comprising 1% of all cutaneous lymphomas; however, it is the most prevalent type of lymphoma involving the subcutaneous tissue. 1 The commoner cutaneous lymphomas described on fine needle aspiration cytology (FNAC) are anaplastic large cell lymphoma, diffuse large B cell lymphoma, and mycosis fungoides; however, the morphology of SPTCL on FNAC has seldom been described in the literature. Uncommonly a subcutaneous panniculitis nodule may be subjected to FNAC that has to be differentiated from SPTCL. Manosca et al. in 2004 have attempted to describe the cytomorphological features of this entity. 2 We want to contribute our experience with this case to enrich the limited knowledge available on this rare entity.
Case Report
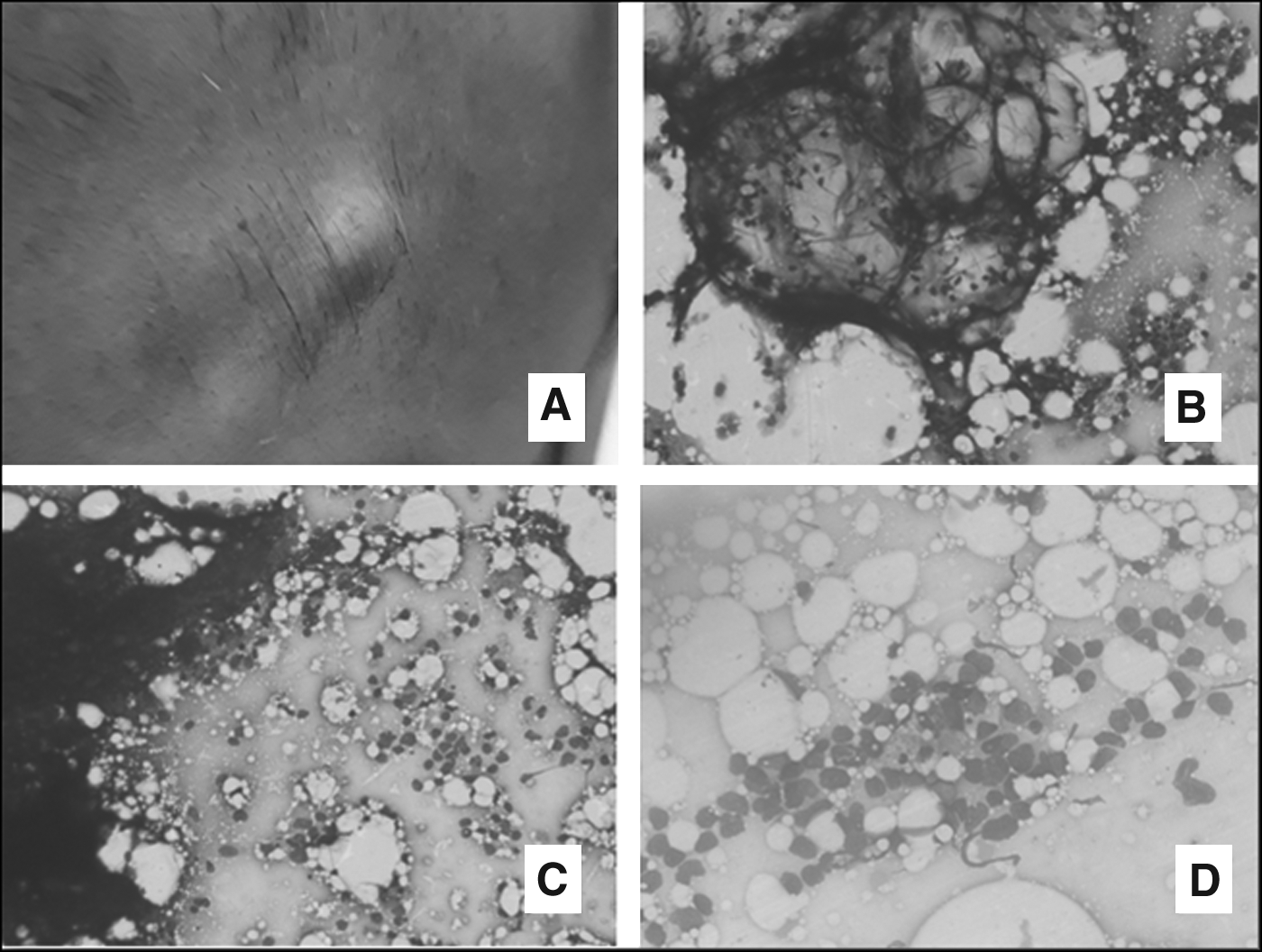
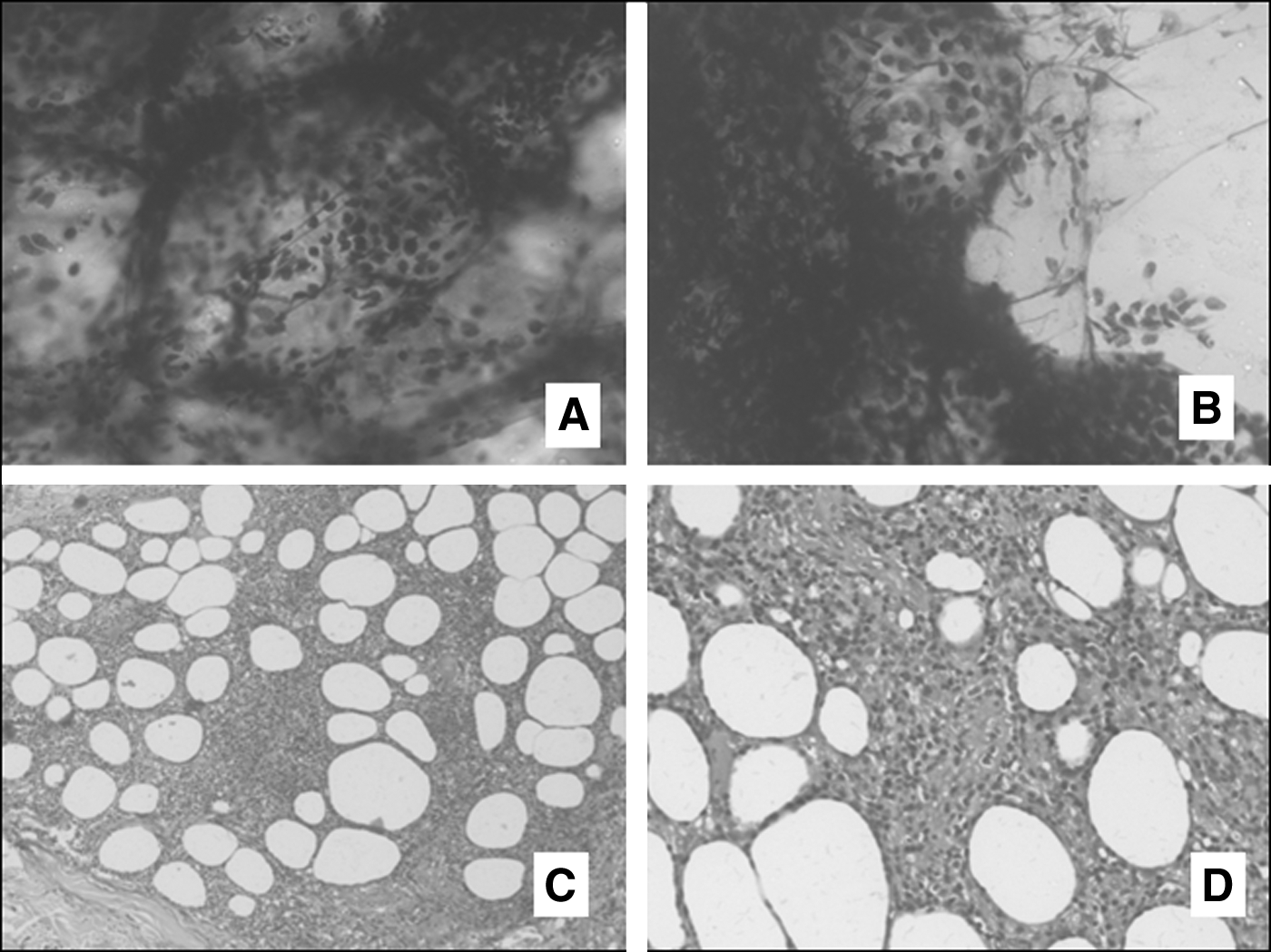
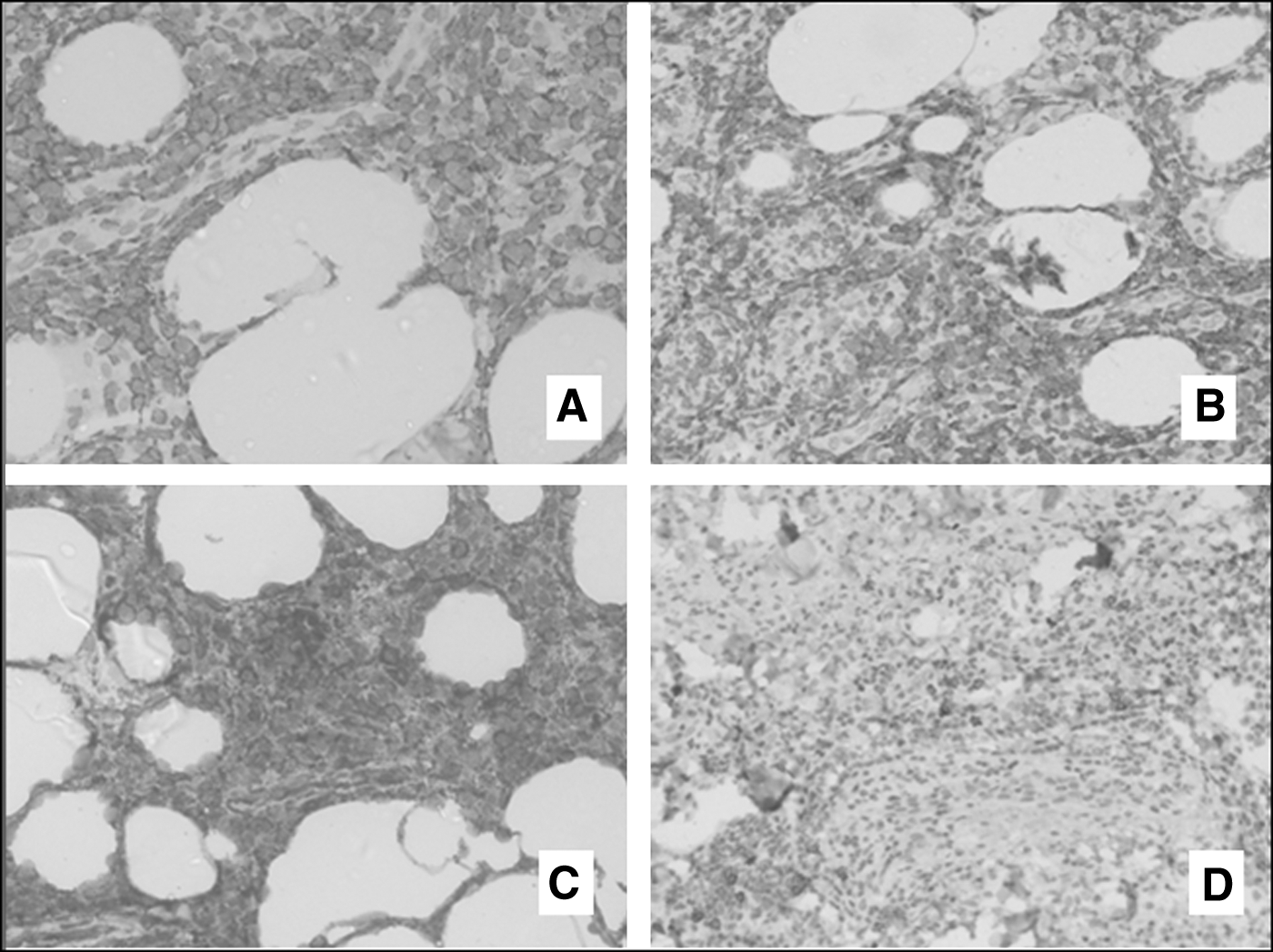
A 33 years old male patient was referred to cytology OPD with multiple painful subcutaneous swellings all over the body for 2 weeks. There was no history of fever/weight loss or lymphadenopathy. FNAC was performed from the largest lesion on the back (Fig. 1A), which yielded creamy and greasy material. The MGG (May Grunwald Giemsa) and PAP (Papanicolaou) stained smears on microscopy were moderately cellular with a predominance of clusters/chunks of mature adipocyte. Also seen was good number of inflammatory cells making panniculitis as the first possible diagnosis, but on higher magnification, these discretely lying lymphoid cells were atypical. They were exhibiting moderate nuclear pleomorphism, oval to irregular nuclei, and scant basophilic cytoplasm (Fig. 1B–D). All the adipocyte clusters were also infiltrated and intimately admixed with the same atypical looking lymphoid cells (Fig. 2A, B). No plasma cells, small lymphoid cells or histiocytes, were seen in the smear making panniculitis a less likely diagnosis. Hence the case was reported as primary cutaneous non-Hodgkins lymphoma suggestive of SPTCL. The hematoxylin and eosin (H&E) sections of the biopsy showed an unremarkable epidermis with subcutis showing lobular panniculitis-like pattern. The infiltrate constituted of atypical small-to-medium-sized lymphoid cells having irregular hyperchromatic nuclei (Fig. 2C, D). These cells exhibited extension into the lower dermis. As evident in cytology, no plasma cells or small mature lymphoid cells were seen in the biopsy. The neoplastic population on immunohistochemistry (IHC) was positive for CD2, CD3, CD8 (Fig. 3A–C respectively), and CD5. These tumor cells were positive for CD4 in focal areas. (Fig. 3D), whereas CD20 and CD56 were negative. IHC for BF1 and TIA1 markers could not be performed due to nonavailability of these antibodies at our center. However, the case was reported as SPTCL. The patient is under follow-up without any treatment for lymphoma because the lesions have reduced spontaneously after 3 months follow-up.
Discussion
In 1991, Gonzalez et al. explained for the first time a different type of lymphoma involving the subcutaneous tissue, 3 which was named as SPTCL. In a study, including a large number of cases of SPTCL conducted by Willemze et al. in the year 2008, it was found that the mean age at diagnosis of SPTCL was 36 years. It was commoner in females than in males, with a ratio of 2:1, respectively. 4 The universal clinical presentation in all their patients was a nodular skin lesion or deep-seated plaque ranging in diameter up to 20 cm. 4 The most common sites involved by SPTCL were legs, followed by arms, trunk, and less commonly the face. A total of 37 out of 63 patients also had some form of B symptoms (fever, night sweats, and weight loss). 4 Aspirate from a subcutaneous swelling of SPTCL shows cellular smears of atypical lymphoid cells, admixed with clusters of adipocytes, 2 whereas FNAC of a nodule of panniculitis would show inflammatory cells comprising lymphocytes, plasma cells, and neutrophils. Also can be seen are aggregates of foamy histiocytes with or without intermingled adipocytes and multinucleated Touton's type giant cells. 5 Hyaline or fat necrosis may be present in some forms of panniculitis. Hence a cytologist has to focus on the type of cell infiltrate along with the adipocyte clusters. The other morphological differential on cytology would be that of non-SPTCL primary lymphoma (nodular mycosis fungoides and cutaneous B cell lymphoma), but these lymphomas do not show the intimate admixture of the tumor cells and adipocyte clusters. On histopathology, SPTCL would show a panniculitis-like pattern of neoplastic elements involving the subcutaneous tissue, with extremely rare involvement of the epidermis. The atypical lymphoid cells are predominantly of medium size but there may be an admixture of a varying proportion of small cells. 6 On IHC of SPTCL, the atypical lymphoid cells are positive for CD3, 7 CD8, and CD2 in most of the cases,7–9 similar to our case, thus confirming the T cell lineage of the neoplastic cells. The neoplastic cells are mostly negative for CD44,10; however, our case showed occasional cell to be positive, which is in concordance with the finding of Weenig et al. in 42% of cases. The neoplastic cells are negative for CD5 and CD56 in 50% of cases, 4 which is the case in our biopsy. In the early phase of SPTCL, the lesions may resolve without any treatment and new lesions may develop either on the same site or on a different site. 10 In the advanced phase of the disease, chemotherapy with cyclophosphamide, vincristine, doxorubicin, and prednisolone form the mainstay of the treatment, with an overall remission rate of 50%. 10 More recently as per the 2016 revision of the World Health Organization classification of lymphoid neoplasms, 11 SPTCL had been differentiated into two subtypes, based on the T cell receptor phenotype: αβ, which is now considered as the only type of SPTCL, and γδ type, which is currently regarded as a separate entity. The two subtypes have also varied prognostic significance. Cutaneous γ/δ T cell lymphoma show epidermal involvement with or without ulceration. The tumor cell infiltrate has an immunoprofile of CD4–, CD8–, and CD56+/–, and poorer prognosis than SPTCL. 4 The immunophenotypical categorization for α/β and γ/δ was not done in our case due to lack of the specific diagnostic modality. As suggested by Willemze et al., SPTCL gamma-delta subtype typically has a dual CD4 and CD8 negative T cell phenotype while the SPTCL alpha-beta subtype shows CD8 positive and CD4 negative neoplastic T cells. Owing to the indolent course of the disease in our patient, it was concluded that the lesion that we encountered was SPTCL rather than cutaneous γ/δ T cell lymphoma, which is an aggressive variant of subcutaneous lymphoma. 9 According to the WHO–EORTC classification for cutaneous lymphomas, the term SPTCL is meant only for SPTCL-ABs, so our case is confirmed to be SPTCL. 4 This conclusion is in agreement with the finding of the study done by Go and Wester. 6 Another point to note is that all cutaneous nodules with greasy aspirates are not lipoma as we found out in this case.
Conclusion
This case describes the rare cytological features of SPTCL that can easily be differentiated from other cutaneous primary and secondary lymphomas as well as panniculitis on cytology. Most general pathologists would miss the correct diagnosis, owing to the unfamiliarity with even this entity. Therefore, propagation of the cytomorphology of this entity will help diagnose more and more of these cases. Nevertheless we do not recommend diagnosing this entity on cytology as it needs the specific architectural pattern on histopathology and a battery of immunomarkers for confirmation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.