
Abstract
Germ cell tumors (GCTs) represent the most common form of testicular neoplasms. Metastasis is common in testicular GCTs with lungs, liver, and brain being the common sites of distant tumor spread. Cutaneous metastasis is, however, seldom encountered in testicular GCTs. Herein, we report a rare case of testicular mixed GCT in a 28-year-old male presenting with cutaneous metastasis after orchiectomy. Moreover, the tumor was characterized by estradiol and human chorionic gonadotropin (hCG) cosecretion. Although hCG secretion is not uncommon, autonomous estradiol secretion from GCTs is an extreme oddity.
Introduction
Germ cell tumors (GCTs) represent the most common form of testicular neoplasms. 1 Metastasis is common in testicular GCTs, especially in nonseminomatous subtypes, with lungs, liver, and brain being the common sites of distant tumor spread. 2 Cutaneous metastasis is, however, seldom encountered in testicular GCTs. Dermatologic spread from primary genitourinary malignancies has been noted in only 1.6% of cases with the incidence of cutaneous metastases from the testes being 0.4%. 3 Herein, we report a rare case of testicular mixed GCT presenting with cutaneous metastasis post-orchiectomy. To make things all the more interesting, the tumor was characterized by estradiol and human chorionic gonadotropin (hCG) cosecretion. Although hCG secretion is not uncommon, autonomous estradiol secretion from GCTs is an extreme oddity.
Case Presentation
A 28-year-old male presented to our institute in November 2019 with right-sided testicular swelling that had been gradually increasing in size over the last 8 months. It was associated with dull aching pain and dragging sensation in the right scrotum. He was otherwise asymptomatic. His past medical history was significant. He had a left undescended testis and bilateral inguinal hernia. He had undergone left orchiectomy and bilateral herniorrhaphy in 2014 at a private hospital, the records of which had unfortunately been misplaced by the patient. On enquiry, he gave a history of timely attainment of pubertal events. He did not complain of loss of libido or erectile dysfunction.
On physical examination, he had a right testicular enlargement with loss of testicular sensation. The left scrotum was empty. There were scar marks over bilateral inguinal regions corresponding to the sites of herniorrhaphy. He was well virilized and had no stigmata of Klinefelter syndrome. Scrotal ultrasonography revealed a well-defined solid cystic mass measuring 10x8 cm involving the right testis and an empty left scrotal sac. Contrast-enhanced computerized tomography also showed a right testicular mass; however, there was no retroperitoneal lymphadenopathy or metastatic deposits in the chest or abdomen.
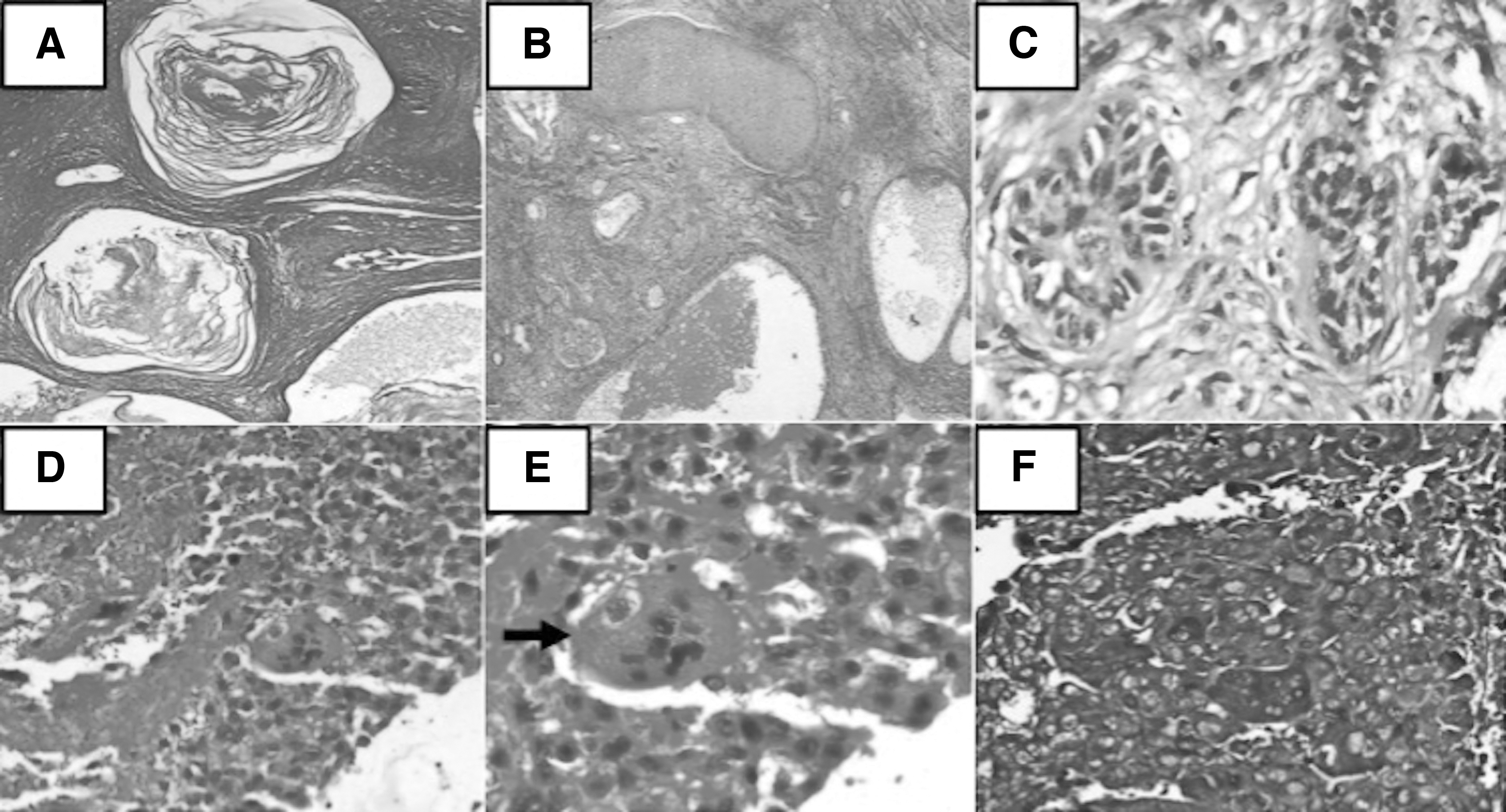
Serum human chorionic gonadotropin (β-hCG) was markedly elevated (67,820 mIU/mL), while serum levels of alpha-fetoprotein, lactate dehydrogenase, and alkaline phosphatase were normal. He had a normal male karyotype (46 XY). Accordingly, he was clinically diagnosed as having right testicular GCT and underwent right radical high inguinal orchiectomy in December 2019. The perioperative period was uneventful. Histopathology was suggestive of a 12 × 8 × 7 cm mixed GCT composed of immature teratoma (96%) and choriocarcinoma (4%) (Fig. 1). The spermatic cord was not involved by the tumor; however, lymphovascular space involvement was noted.
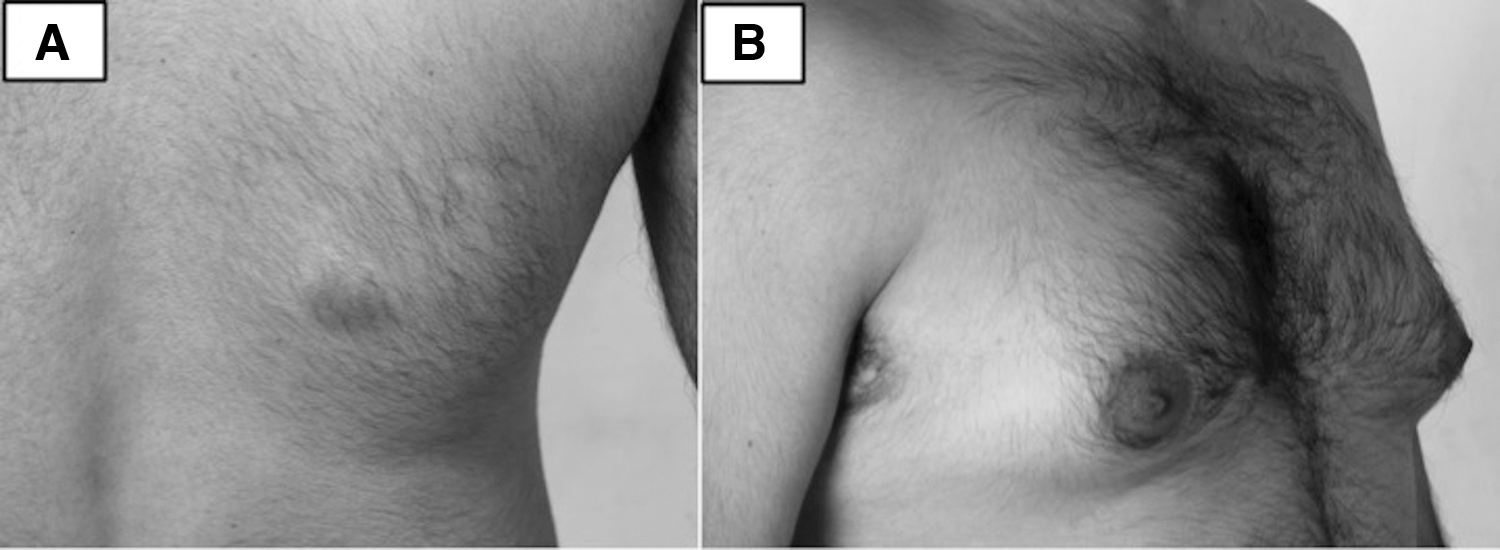
The patient presented a month later with the complaints of a new-onset swelling over his upper back (that was brought to his notice by his mother) as well as a recent increase in the size of his breasts. Examination showed a 2 × 2 cm violaceous, nodular, well-defined swelling over the right upper back (Fig. 2A). He had bilateral gynecomastia (Simon Grade IIa) 4 (Fig. 2B). The serum level of β-hCG was further raised (>300,000 mIU/mL). In addition, serum estradiol was remarkably elevated (634 pg/mL); on the contrary, serum testosterone (0.740 nmol/L), luteinizing hormone (LH: 1.39 mIU/mL), and follicle-stimulating hormone (FSH: 0.320 mIU/mL) were low.
18 F-fluorodeoxyglucose (FDG) positron emission tomography–computed tomography (PET-CT) revealed multiple pulmonary, abdominal lymph nodal, and vertebral (thoracic) metastatic deposits along with a hypermetabolic subcutaneous soft tissue lesion in the right upper back, corresponding to the location of the newly emergent swelling. Fine needle aspiration (FNA) from the lump also revealed mixed GCT, confirming it to be cutaneous metastasis (Supplementary Fig. S1). The patient was finally diagnosed as metastatic mixed GCT, stage pT2N1M1bS3 (AJCC 8th edition), composite stage IIIC, and categorized as being poor risk.
He was started on 3-weekly chemotherapy with a modified bleomycin (30 IU on day 1), etoposide (100 mg/m2 on days 1–5), and cisplatin (20 mg/m2 on days 1–5) regimen. 5 The patient tolerated the regimen well with no significant toxicity. Following the first cycle, there was a noticeable reduction in the size of the skin lesion. Hitherto, he has received all six cycles of chemotherapy. The skin lesion has disappeared and gynecomastia has subsided. Concomitantly, there has been a parallel reduction in serum β-hCG and estradiol with each cycle of chemotherapy, which has been summarized in Table 1.
Showing Changes in Biochemical Parameters at Presentation and Thereafter at Different Stages of Treatment
Serum tumor markers could not be done after 5th cycle of chemotherapy.
β-hCG, beta-human chorionic gonadotropin; FSH, follicle-stimulating hormone; LH, luteinizing hormone; RR, reference range.
Repeat PET-CT performed at the end of six cycles of chemotherapy showed a partial response with a significant decrease in the number, size, and avidity of the pulmonary and skeletal metastases. There were no skin lesions. In addition, the retroperitoneal lymph nodes had decreased in size to <1 cm and all were FDG nonavid. The further plan is to follow-up the patient regularly with serum tumor markers and imaging.
Discussion
More than 90% of testicular neoplasms are GCTs. In adults, mixed GCTs represent the second most common type of testicular GCT after seminomas, comprising 30%–50% of the cases. 6 Mixed GCT, as the name implies, is composed of two or more seminomatous or nonseminomatous histologic subtypes in their pure form. The most common histologic subtypes in a mixed GCT in order of frequency are embryonal carcinoma, teratoma, yolk sac tumor, seminoma, and choriocarcinoma. 7 Teratoma as a component of mixed GCT is noted in around 50% of mixed GCT and choriocarcinoma in only 8% of cases.6,8 The combination of choriocarcinoma and teratoma as seen in the index case is not an uncommon entity. However, cutaneous metastasis in mixed GCT is indeed unique. In fact, cutaneous metastasis is rare in solid malignancies. Out of 81,618 primary solid visceral malignancies, only 2369 reported cases of cutaneous metastasis could be identified, amounting to an overall incidence of 2.9%. 3 Skin metastases are most commonly seen in breast cancer (69%), colon cancer (9%), and melanoma (5%) in females, while in males, skin secondaries are common in malignancies of the lung (24%), colon (19%), and melanoma (13%). 9 Chest and abdomen are the most frequent sites of skin metastasis as seen in the index case. 10
Metastatic spread of testicular GCTs to the lungs, liver, and brain is common and in 20%–30% of patients, as in the index case, late metastasis after orchiectomy has also been reported.2,11 Only a few cases of cutaneous metastasis have been reported in GCTs, that too, most commonly in choriocarcinomas.12–17 Hitherto, there are only three reports of cutaneous spread in mixed GCTs.9,18,19 The reported sites of cutaneous metastasis in the aforementioned cases were scalp and upper abdomen, 9 shin, 18 scalp, and upper trunk, 19 respectively.
Clinically, cutaneous metastases from testicular GCTs are usually violaceous to red (as in the index case), hemorrhagic, and infiltrative subcutaneous nodules and may be confused with more common vascular lesions, such as pyogenic granuloma, hemangioma, and Kaposi's sarcoma. 19 The diagnosis is, however, straightforward in a patient already diagnosed as having an underlying testicular GCT; in the index case, the diagnosis was also aided by PET-CT imaging, showing increased tracer uptake exactly at the site of skin metastasis. Histopathological diagnosis entails the use of skin punch biopsy/excisional biopsy; however, FNA can also lead to rapid detection of cutaneous metastasis. 17 The histopathology of the cutaneous deposit usually resembles that of the primary testicular GCT as in this case; nevertheless, Hapa et al. had reported a case of testicular mixed GCT composed of teratoma and seminoma that had metastasized to the skin as pure choriocarcinoma. 19 The presence of cutaneous metastasis in nonseminomatous GCT classifies the patient as poor risk with a 5-year progression-free survival of 41%. 20
Another oddity in this case was the autonomous production of estradiol by the tumor tissue. One may assume that increased production of hCG by the mixed GCT could have led to paracrine activation of aromatase on Leydig cells, 21 thereby promoting conversion of testosterone to estradiol. In a study involving 20 patients with testicular GCTs, estradiol levels were found to be significantly higher in men with hCG-positive tumors (median 44 pg/mL, range 26–110) compared to men with hCG-negative tumors (median 33.5 pg/mL, range 10–87). Besides, free testosterone levels were also significantly higher in the former group compared with the latter, thereby indirectly implying that aromatization of testosterone was the source of increased estradiol in men with hCG secreting testicular GCTs. 22 However, this was not possible in the index case as the patient had undergone bilateral orchiectomy (first in 2014 and then in 2019) and was left with no endogenous source of testosterone. Accordingly, his serum testosterone post-orchiectomy was low (0.740 nmol/L) and was not sufficient enough to produce estradiol levels as high as 634 pg/mL. Low LH and FSH as were seen in our patient also support the fact that estradiol, being autonomously produced by the metastatic deposits, led to the suppression of pituitary LH and FSH as a part of negative feedback loop.
Autonomous estradiol production and aromatase expression have been reported in seminoma. 23 Estradiol levels as high as 3383 pg/mL have also been reported in mature teratoma. 24 Besides, ‘extremely high levels' of estradiol have been reported in embryonal carcinoma and choriocarcinoma as well. 25 In the index patient, the teratomatous component or the choriocarcinomatous component or both could have been the source of estradiol. Estradiol excess was being clinically manifested as gynecomastia. Reduction in tumor burden with chemotherapy led to normalization of estradiol levels, marked reduction in gynecomastia, and parallel rise in serum LH and FSH. In fact, gynecomastia is a prognostic marker in testicular GCTs. In 45 patients with testicular GCTs, mortality was found to be higher in patients with gynecomastia than in those without. Survival was also strikingly shortened by the appearance of gynecomastia. On the contrary, the disappearance of gynecomastia correlated with good prognosis and corroborated with tumor eradication. 25
Conclusions
Skin is an uncommon site for testicular GCT metastasis. The initial presentation as cutaneous metastasis may pose a challenge to the physician and needs to be differentiated from a primary cutaneous neoplasm. However, the diagnosis should be readily entertained in a patient already known to have an underlying testicular GCT. Although cutaneous metastasis portends a poor prognosis, cisplatin-based chemotherapy remains the cornerstone of therapy.
Patient Consent
Written informed consent was obtained from the patient.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.