
Abstract
Background:
Osteosarcoma (OS) is the most common primary bone sarcoma in childhood. High-dose methotrexate, doxorubicine, cisplatin, and/or ifosfamide combinations are used as standard treatment in chemotherapy and could cause serious toxicity. Another alternative chemotherapy protocol is consisting of epirubicin, ifosfamide, and cisplatin (ECI), which we use in our center. The aim of this study was to evaluate the patients with OS who were treated with ECI protocol, retrospectively.
Methods:
Forty-three patients with OS diagnosed at our center between December 1995 and September 2017 were evaluated retrospectively.
Results:
The mean follow-up period was 31 months (5–145 months). Recurrence was detected in 15 of 43 patients. When the factors affecting relapse are examined, recurrence was higher in patients who were older than 10 years at the time of diagnosis, upper extremity involvement, osteoblastic, and chondroblastic subgroups, but there was no statistically significant difference. Five-year and 10-year overall survival rates were 67.4% and 58.9%, and event-free survival rates were 54% and 47.3%, respectively. While 5-year overall survival rate was 86.7% in nonrecurrent cases, this rate was 40.9% in recurrent cases and this difference was statistically significant (p = 0.023). Just two patients died because of the toxicity.
Conclusion:
The prognosis of OS is still poor in relapse cases, so the choice of chemotherapy for neoadjuvant and adjuvant therapy is vital. When the risk of toxicity is also considered, the first step of ECI protocol is seen as a preferable treatment option because the survival rates are similar to the literature.
Introduction
Osteosarcoma (OS)
The most important prognostic factors are whether the disease is metastatic at the time of diagnosis, the response rate to neoadjuvant chemotherapy, and total resection of the tumor.5,6 According to Huvos necrosis grading system, the rate of necrosis in the tumor after neoadjuvant chemotherapy is >90%, indicating that it is a chemosensitive tumor and has a better prognosis. 7 Survival rates are 60%–70% in nonmetastatic diseases8–10 and 10%–30% in metastatic diseases.11–16
High-dose methotrexate (HD-MTX), doxorubicin, cisplatin, ±ifosfamide combinations are used as a standard treatment in chemotherapy. 17 The recommended dose of MTX for OS is 8–12 g/m2, and these doses can cause severe toxicity, and even some side effects may be fatal. 18 The main toxicities are nephrotoxicity, hepatotoxicity, neurotoxicity, and severe mucositis preventing enteral feeding, significant and prolonged myelosuppression. 19 Doxorubicin is the other effective drug for treating OS; however, one of the considerable toxicity is cardiovascular toxicity. These problems may require interrupting chemotherapy and disrupt treatment. Another alternative chemotherapy protocol that does not include high-dose methotrexate and doxorubicin is the protocol consisting of epirubicin, ifosfamide, and cisplatin (ECI),20,21 which we use in our center. Epirubicin is another anthracycline antibiotic that induces cardiac problems, but its cardiotoxicity is less than doxorubicin cardiotoxicity.
This study aimed to evaluate the overall and event-free survival, factors affecting survival and toxicity of patients with OS who were treated with ECI protocol retrospectively. We hypothesize that this protocol can be used in patients who cannot receive high-dose methotrexate with less toxicity without affecting survival rates.
Materials and Methods
Forty-five patients with OS were diagnosed at our center between December 1995, and September 2017. 03.01.2020–09.2020.102 numbered Ethics Committee approval was obtained. The treatment scheme is presented in Table 1. The diagnosis of all cases was made by histopathologic examination after the biopsy. Neoadjuvant three or four ECI treatment cycles were applied to all patients with metastatic or nonmetastatic OS who did not receive treatment before. The response was evaluated according to the World Health Organization (WHO) criteria. Patients were considered to have a complete response (CR) if there was no sign of disease. A partial response (PR) was defined as at least 50% decrease in all measurable lesions (primary or metastases). Progressive disease (PD) was defined as at least 25% increase in the size of any lesion or appearance of any new lesion. Stable disease was defined as the absence of CR, PR, or PD. Objective response was defined as CR plus PR.
Treatment Scheme of Epirubicin, Ifosfamide, and Cisplatin Protocol
After radiological evaluation, surgery was performed for local treatment. Histopathological examinations were evaluated by pathologists experienced in bone tumors at our center. Necrosis rates were obtained retrospectively from pathology reports. According to the Huvos grading system,
As we know, the incidence of OS shows a peak with age until around puberty, and it is extremely rare in children younger than 5 years of age. A study that reported the incidence and survival in Argentina with big series analyzed the survival of the patients younger than 10 years of age and 10–14 years of age. 22 So, in our study, the age of diagnosis was divided into two groups as 10 years and younger and older than 10 years, and the effect of the age factor on survival and relapse was evaluated. Five and 10 years of overall survival and event-free survival rates were calculated, and the factors that could lead to survival and relapse were examined. The overall survival was calculated from the time the patient was diagnosed with OS to the date of death or last followed up, while the event-free survival was calculated from the time of diagnosis to the date of death or relapse.
Erythrocyte (Hb <7 g/dL) and platelet transfusion (Plt <20,000/mm3) were performed as supportive therapy. Granulocyte colony-stimulating factor (G-CSF) was not used in every patient as primary prophylaxis. It was used as second prophylaxis only in cases of sepsis or patients with profound and long-term neutropenia.
Statistical analyses were performed using the SPSS software version 17. The patients' demographic and clinical characteristics were presented by using descriptive analyses as percentages, frequencies, medians, means, and standard deviations. The effect of recurrence, metastasis, and sex was investigated using Kaplan–Meier analysis with log-rank test both on overall survival and event-free survival of patients with OS. Overall and event-free survival estimates were also calculated with Kaplan–Meier analysis. Survival rates at 5 and 10 years were calculated. The Kaplan–Meier survival curves were plotted to depict the survival function over time between the predictors' levels. Furthermore, the effect of possible factors on the recurrence of the patients was entered into the Cox regression analysis. Statistical significance was set at two-tailed p < 0.05.
Results
Between December 1995 and September 2017, 45 patients diagnosed with OS were treated with ECI protocol. Patients who were treated with ECI protocol in our center and for whom all the data were available were included in the study. Two of 45 patients treated with ECI were excluded from the study due to lack of data, and 43 patients were evaluated, retrospectively. Patients' characteristics are shown in Table 2. The most common site of involvement was the right femur, with a rate of 32.6% (n = 14). The mean follow-up period was 42.6 ± 37 months. In the radiological evaluation after neoadjuvant chemotherapy, 36 (83.7%) cases were evaluated as regression, 3 (6.97%) cases as stable disease, and 4 (9.3%) cases as PD.
Patients' Characteristics (n = 43)
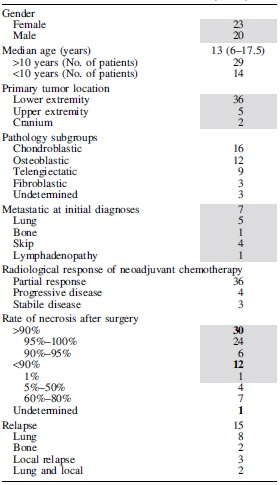
Necrosis rate was below 90% in 8 of 36 cases with regression, and necrosis rate was above 90% in only one of 4 cases with progression. The postoperative necrosis rates of three patients with stable disease in the radiological evaluation were 90% or less. In the histopathological evaluations performed after neoadjuvant chemotherapy, the necrosis rate was 90% or higher in 30 (69.7%) of 43 cases, while it was below 90% in only 12 (27.9%) cases.
Recurrence was detected in 15 (34.8%) of 43 patients. The mean recurrence time after treatment was 11.4 ± 4.1 months. The most common relapse site was lung, with 10 patients (23.3%). Recurrence was 3.5 times higher in patients older than 10 years at the time of diagnosis, but this rate was not statistically significant (p = 0.074). Although recurrence was 2.9 times higher in patients with upper extremity involvement, there was no statistically significant difference (p = 0.220). According to the pathological subgroups, the recurrence rate was 1.2 times higher in patients other than osteoblastic and chondroblastic, but there was no statistically significant difference (p = 0.829).
Survival
Five-year and 10-year overall survival rates for all patients were 67.4% and 58.9% (Fig. 1), and event-free survival rates were 54% and 47.3%, respectively (Fig. 2). The mean survival time of those without metastasis was 101.87 months (95% CI 78.34–125.40), whereas the mean survival time of those with metastasis was 58.25 months (95% CI 28.30–88.20). When factors affecting overall survival are examined, sex, metastasis status at the time of diagnosis, location of involvement, pathological subgroup, and necrosis rate were not statistically significant. While the 5-year overall survival rate was 86.7% in nonrecurrent cases, this rate was 40.9% in recurrent cases, and this difference was statistically significant (p = 0.023) (Fig. 3). When the factors affecting event-free survival were evaluated, it was found that metastasis at the time of diagnosis (p = 0.044) had a statistically significant effect.
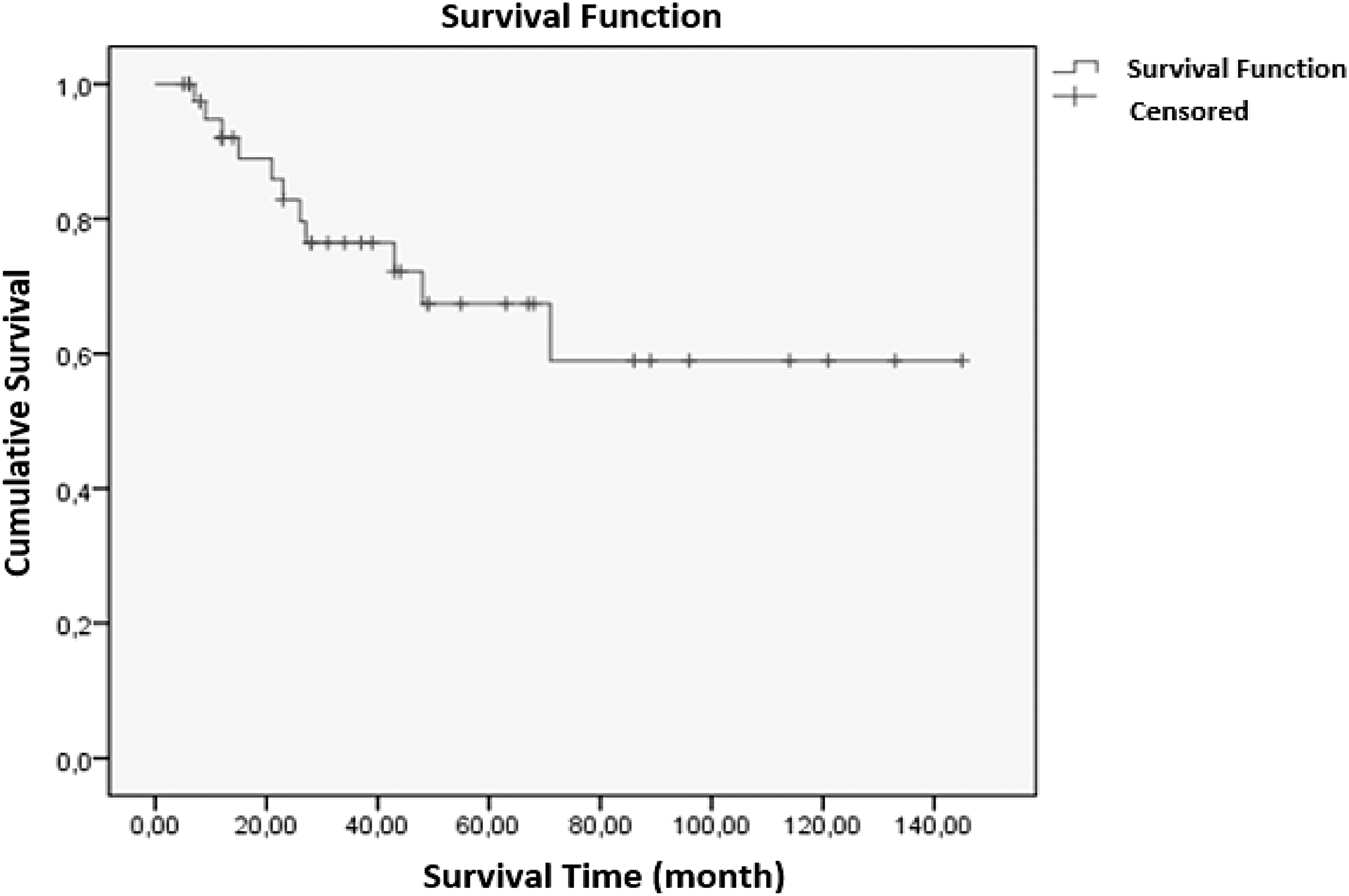
Five-year and 10-year overall survival rates. Five year OS = 67.4% 10 year OS = 58.9%. OS, osteosarcoma.
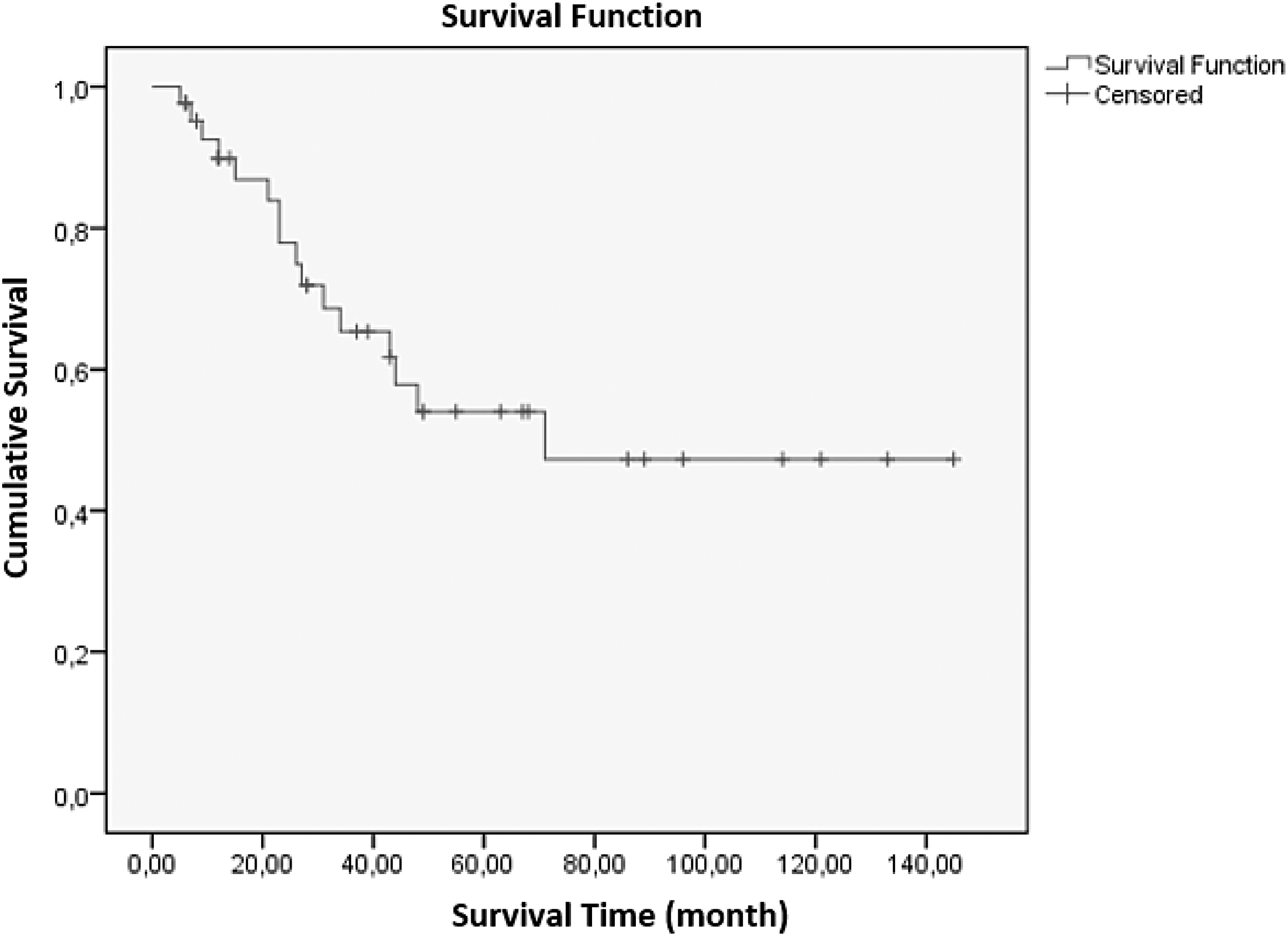
Five-year and 10-year EFS rates. Five-year EFS = 54.0%. 10-year EFS = 47.3%. EFS, event-free survival.
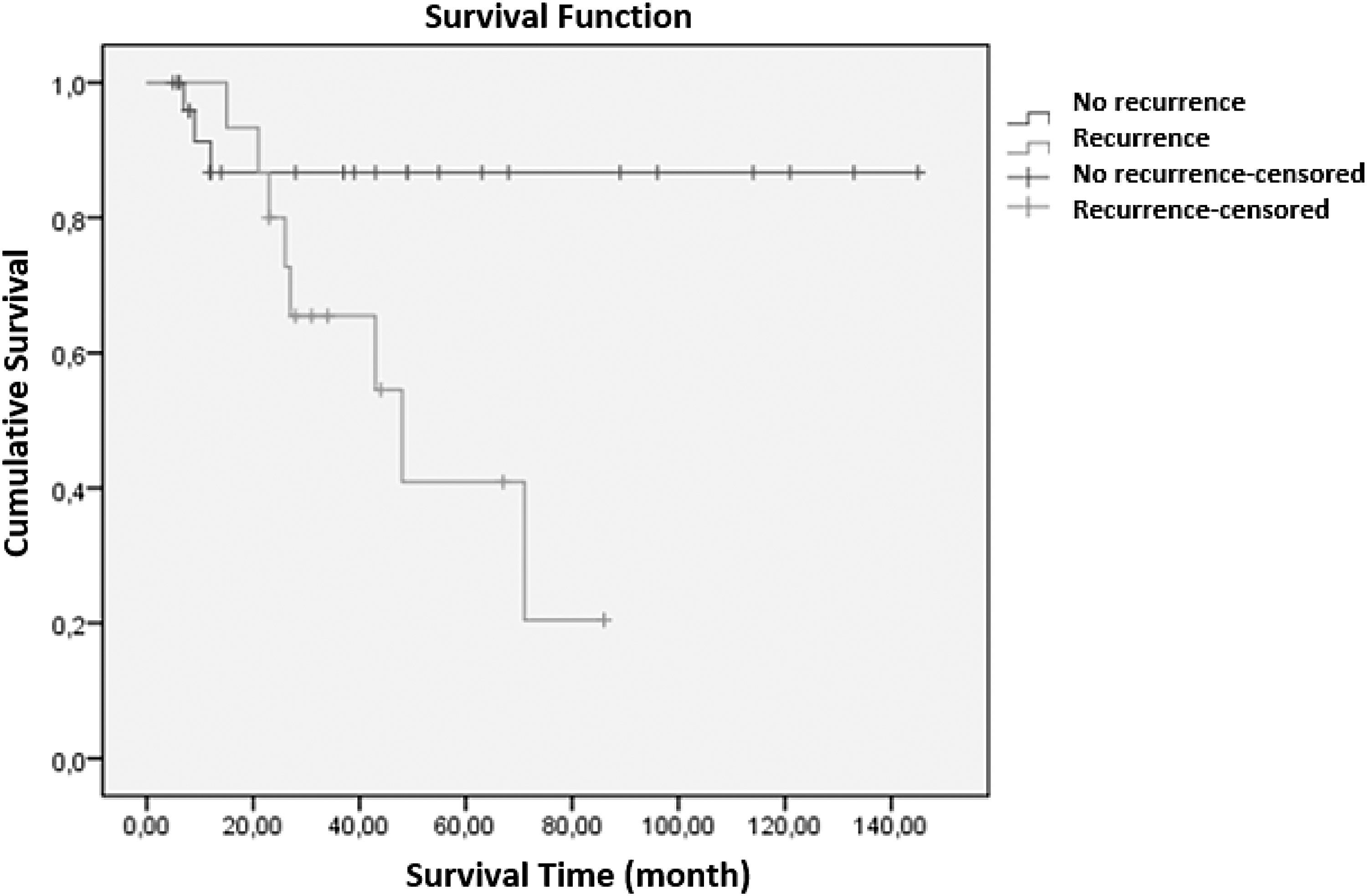
Five-year overall survival rate was 86.7% in nonrecurrent cases, and 40.9% in recurrent cases (p = 0.023).
Five-year overall survival rates of patients below 10 years of age and older than 10 years were 75.5% and 59.3%, respectively (p = 0.710). Event-free survival rates of patients below 10 years of age and older than 10 years were 70.1% and 41.3%, respectively (p = 0.401). In patients younger than 10 years of age, sex, metastasis status at the time of diagnosis, location of involvement, pathological subgroup, necrosis rate, and recurrence status had no statistically significant effect on both overall survival and event-free survival. In patients older than 10 years of age, sex, metastasis status at the time of diagnosis, pathological subgroup, and necrosis rate had no statistically significant effect on both overall survival and event-free survival. However, location of involvement had statistically significant effects on event-free survival (p = 0.036) in patients older than 10 years of age. Event-free survival was even worse in those with upper extremity involvement. Overall survival, location of involvement, and recurrence status had no significant effect in this group (p = 0.678, p = 0.179).
Toxicity
Toxicity profiles are shown in Table 3. Grade 3–4 thrombocytopenia, grade 3 anemia, grade 4 neutropenia, and at least one febrile neutropenia attack were present in all cases. G-CSF was used for profound and long-term neutropenia in 9 (20.9%) patients and sepsis in 1 (2.3%) patient. One case had hepatosplenic candidiasis, and another case had pulmonary aspergillosis infection after the sixth cycle of chemotherapy. One patient had polyneuropathy, one had cardiotoxicity, six had tubulopathy, and two of them had acute renal failure.
Toxicity Profiles of the Patients
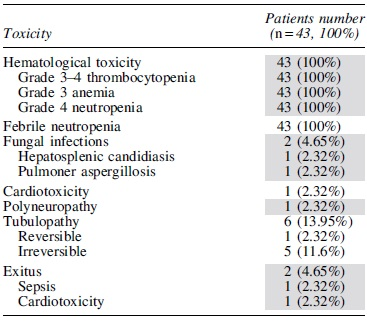
Ifosfamide was not given in the last cycle in only one of the six patients who developed tubulopathy, and the dose was not skipped or reduced because it developed after the sixth cycle in the other patients. Tubulopathy was irreversible in five cases, but three of these cases continued to be treated with relapse chemotherapy protocol due to relapse disease. One of the other two cases died due to sepsis, and one died due to PD. Tubulopathy was reversible in one patient who received only ECI protocol and lived disease-free. In the patient who developed polyneuropathy, neuropathy had a reversible course. In one patient who developed cardiotoxicity, the dose was not skipped because the toxicity developed after the sixth cycle. Nine cases died due to PD, one case sepsis, and one case due to cardiotoxicity.
Discussion
OS is the most common malignant bone tumor in childhood, and survival rates have increased with neoadjuvant and adjuvant intensive chemotherapy protocols added to surgical treatment. However, despite multimodel treatment approaches, especially in relapse and metastatic diseases, it still has low survival rates. Macrometastasis is present in 10%–20% of cases at the time of diagnosis, and the most common sites are lung (90%), bone (8%–10%), and rarely lymph node metastasis.23–26 In our study, 16.3% of the cases had metastasis at the time of diagnosis. When the sites of metastasis were examined, the most common site of metastases was lung in five patients (71.4%). Simultaneously with lung metastasis, there was an inguinal lymph node in one case, bone in one case, and skip metastasis in two cases. The survival rate is 10%–50% of the patients with metastatic disease. 27 In our study, 5-year overall survival rates were 41.6% in metastatic cases and 70.7% in nonmetastatic cases. However, this difference was not statistically significant (p = 0.626). The 5-year event-free survival rates of metastatic and nonmetastatic cases were 17.9% and 63.2%, respectively. This difference was statistically significant in accordance with the literature 13 (p = 0.044). When all cases were evaluated, our 5-year overall and event-free survival rates were 67.4% and 54%, respectively. In the EURAMOS group study, where >2000 patients were evaluated, these rates were 71% and 54%. 28 Our study showed similar results with this comprehensive study.
To the best of our knowledge, metastasis status, primary tumor localization, and histologic response are the most important prognostic factors affecting survival. In our study, when the factors affecting overall and uneventful survival were evaluated, it was found that age, sex, involvement, and histological response did not affect survival rates. Metastasis status at the time of diagnosis did not affect overall survival, but event-free survival was significantly lower in metastatic patients (p = 0.044).
Relapse has been reported in 30%–40% of patients with the localized OS. 29 Similarly, 34.8% of our cases developed relapse, and the most common relapse site was the lung, with 66.6% of the relapse cases. The most important factor affecting overall survival was relapse in our study. While the 5-year overall survival rate was 86.7% in nonrelapsed cases, this rate was 40.9% in relapse cases, and this difference was statistically significant (p = 0.023). Although there was no statistical significance when the factors affecting relapse were evaluated, it was observed that the rate of relapse was 3.5 times higher in patients older than 10 years of age (p = 0.074) and those with upper extremity involvement at the time of diagnosis 2.9 times higher (p = 0.220) should be evaluated in more comprehensive studies. Another significant result of our study was that in patients older than 10 years of age group, event-free survival rate was significantly lower in patients with upper extremity involvement (p = 0.036). This result should be evaluated in more comprehensive studies, too.
When the histopathological response results were evaluated, in the EURAMOS-1 study in which MAP was used, 28 viable cell rates were found below 10% in 51.8% of the cases and over 10% in 48.1%. In our study, the necrosis rate was 90% and above in 69.7% of the cases, and it was below 90% in 27.9% of the cases.
OS survival rates and the variety of current treatment methods increase, and long-term survival is possible. However, the reduction of toxicities has also gained importance in treatment. High-dose MTX, which is the standard treatment approach, could have severe and fatal side effects. When the toxicity results of our study were compared with the MAP arm in the EURAMOS-1 study. 30
While neutropenia and grade 3–4 thrombocytopenia were seen in every case in our study, it was observed in 94% of the cases in the EURAMOS study, and thrombocytopenia in 93% of the cases. In the same study, neuropathy developed in 15% of the cases and left ventricular systolic dysfunction in 15% of the cases, while in our study, only one (2.3%) case developed cardiotoxicity, and only one (2.3%) case developed neuropathy. In our study, although severe hematological toxicity was detected in all cases, only one patient died due to sepsis. No toxic death and permanent organ dysfunction were seen, except in one case, who died due to cardiotoxicity.
The limitations of our study are that it is a retrospective and nonrandomized study with a small number of patients. Since in our study, a single-center and a single treatment protocol was applied, we do not have a comparison group. However, we think it contains remarkable results.
Conclusions
OS treatment is still difficult and multimodel treatment is essential. The prognosis is poor in relapse cases, so the choice of chemotherapy for neoadjuvant and adjuvant therapy is vital. When the risk of toxicity is also considered, the first step of ECI protocol is seen as a preferable treatment option because the survival rates are similar to the literature.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There is no funding was received.