
Abstract
Significance:
Cancer treatment impacts young adults' (YA) biological and psychosocial health, with over >50% reporting unmet needs. Physical activity (PA) offers symptom mitigation, risk reduction, and critical independence to YA (age 18–39 years) affected by cancer. When tailored to YA, PA guidelines can facilitate PA integration into survivorship care. However, no current expert consensus on PA use in YA exists.
Aim:
To describe expert consensus and opinions on the application of PA as a biopsychosocial health promotion strategy for YA cancer survivors, guided by the Revised Symptom Management Theory.
Methods:
A four-round modified Delphi study was conducted with international multidisciplinary experts (round I/II, n = 18; round III, n = 57; round IV, n = 45) in exercise oncology, symptom management, survivorship care, and adolescent-YA cancer care. Qualitative content analysis, descriptive statistics (% agreement, SD, mean), and inter-rater reliability (Kappa) were calculated.
Results:
Experts reached a consensus on the following: PA should be integrated into YA cancer care as part of supportive oncology to mitigate symptoms of fatigue, cardiometabolic health, muscle mass loss, altered body composition, and anxiety/depression; PA improves functional capacity and wellbeing; at all points on the care continuum YA should be asked if they would like guidance on PA use; PA interventions should be tailored for personal facilitators, barriers, and motivations, to maximize survivorship adaptations.
Conclusion/Implication:
The results of this study identified areas of expert consensus that warrant PA implementation in YA survivorship care to guide future research and clinical endeavors.
Introduction
Cancer survival rates in adolescents and young adults (YA) have increased to >80% owing to diagnostic and treatment improvements.1–3 However, cancer morbidity remains three times higher among 15- to 29-year-olds than among children.4,5 Cancer and its treatments impact multiple biological and psychosocial systems6–9 with effects appearing decades after treatment.6,9,10
The YA life stage (age 18–39 years), represents a critical transition to independence that is essential to physical and psychological wellbeing. 7 Diagnosis and treatment of cancer can introduce late and long-lasting disruptions and vulnerabilities to YA's biopsychosocial health.8–11 Adolescent and young adult (AYA) (age 15–39 years) cancer survivors face significant more risk of developing chronic conditions than those without cancer.10,12,13 Increased chronic disease burden for YA often requires additional mental health and pain management services. 14 More than 50% of YA cancer survivors report unmet needs surrounding self-management of symptoms and survivorship.10,15 Although some YA may experience growth/greater resilience because of their cancer experience, others are presented with a myriad of physical and emotional quality-of-life (QOL) challenges.16,17 More than 60% of YAs express a lack of age-appropriate support related to lifestyle behavior, mental health, and fertility services. 17
Research indicates that physically active YAs may require less social support to experience growth and adaptation from the cancer experience. 18 Most YA survivors report interest in physical activity (PA) both during and after cancer treatment.8,19,20 However, they are often less physically active than their noncancer peers .8,19 Cancer therapies and symptoms impact PA; additional factors contributing to lower PA include limited dialog between health care teams regarding PA use,21–23 and inadequate access to supportive services tailored to YA's needs and preferences.10,15,24,25 Furthermore, there is limited research on YA survivorship,4,10,15,26,27 and especially research specific to PA.28,29 Evidence regarding PA use as a health promotion strategy originates mostly from adult survivors, with findings indicating positive impacts on physical function, QOL, predictive biomarkers, comorbidities, and mortality.21,22,30–33 An American College of Sports Medicine panel established PA adult guidelines and summarized benefits and research efforts related to PA use in survivorship care.30,34
Precision health entails health care tailored to individuals to optimize health and wellbeing,35,36 and has the potential to foster greater independence and self-management to YA at a critical life stage.28,37 Integration of PA into YA survivors' cancer care may improve overall survival and symptom burden, while improving adaptation to the cancer experience. Therefore, a precision health approach to YA cancer survivorship should include health-promoting supportive care to mitigate late and long-term effects of cancer therapies and to reduce the risk of cancer reoccurrence. 38
Our recent scoping review revealed a lack of guidance, research, and consensus on the role of PA as a component of YA survivorship. 39 This knowledge gap represents a significant barrier to the operationalization of high-quality, patient-directed, precision health care, hindering advocacy, and practice integration. Therefore, this research aims to describe expert consensus on the application of PA as a biopsychosocial health promotion strategy for YA cancer survivors.
Methods
We conducted a modified Delphi study (Fig. 1) to elicit expert opinions and consensus on PA use in YA survivorship. The Revised Symptom Management Model informed the initial qualitative interviews, which is framed around three main constructs: symptom experience, symptom outcomes, and symptom management strategies.40–43 The results from the inductive interviews guided the subsequent survey design. Survey development occurred in round I/II with a small sample of initial experts; initial consensus among an expanded sample of experts took place in round III with the final consensus occurring in this expanded sample of experts in round IV.
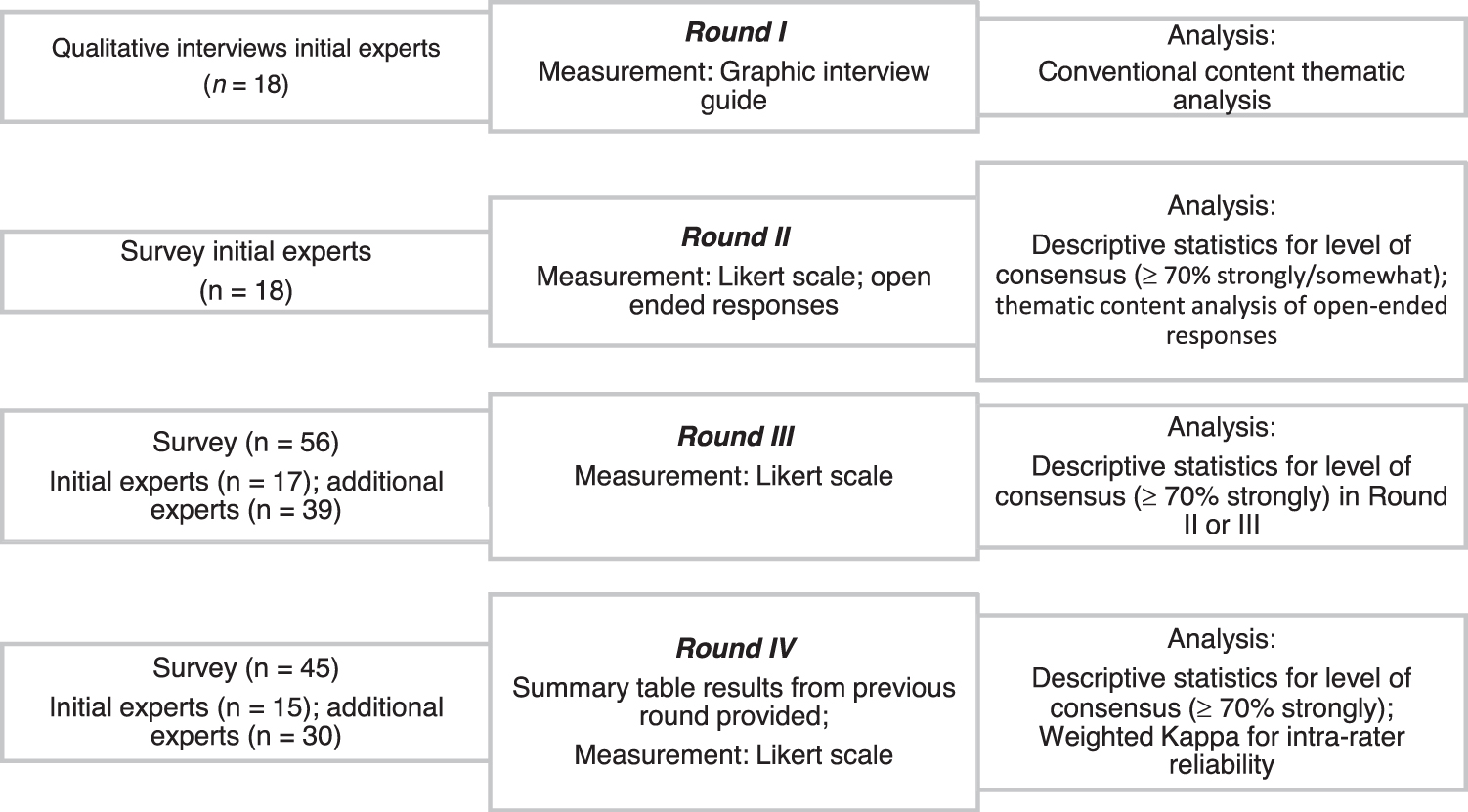
Four round modified-Delphi process.
The project was determined Not Human Subjects Research by the University of Massachusetts Amherst Human Research Protection Office (Determination #20-60).
Study design
The research team purposefully identified a set of multidisciplinary clinical experts with established national reputations on this topic. Round I consisted of recorded audio/video interviews to gather insights from experts on the use of PA in YA survivorship care. Analysis of round I interviews identified themes that guided the structured survey used in subsequent rounds with a larger group of experts (Fig. 1). The round II survey, a developmental round, was used to generate consensus with the same initial experts and establish content validity. Therefore, items in round II were included in the following round III, if >70% of respondents chose “strongly agree” or “somewhat agree,” indicating consensus on the benefit of PA. In rounds III/IV, the consensus was defined as >70% of respondents choosing to “strongly agree.” The Delphi process includes multiple consensus building rounds by providing results from the previous round to increase credibility. Therefore, the results of round III were provided to experts, for their review, before the administration of the round IV survey, as recommended for Delphi consensus-building methodologies. After IRB approval from the University of Massachusetts, Amherst, participants consented electronically. The study took place over 22 weeks in 2020. Experts were given an identification number with results reported in aggregate form. Percent agreement was calculated for initial experts and all experts (rounds III/IV); inter-rater reliability, using the Kappa statistic, accounted for a chance agreement not captured in percent agreement.44,45 Consensus was defined as >70% of respondents choosing to “strongly agree.”
Exercise oncology refers to a transdisciplinary field of study that examines responses to PA in persons with or at risk for cancer and spans from the molecular to environmental responses.46–49 Symptom scientists refer to nurse scientists trained in both clinical and research that examine the biological and behavioral mechanisms of symptoms to improve the lives of patients.50,51
Consensus results
As noted in Table 1, experts represented multiple clinical backgrounds: exercise oncology, survivorship care, symptom science/management, AYA, and YA cancer. Emergent themes from content analysis of qualitative data are found in Table 2. Complete descriptive results (% agreement, sample size, SD, mean), survey statements, and Kappa statistics are given in Tables 3–6. Supplementary Tables S1, S2 include item modifications to the rounds II and III survey.
Distribution of Experts' Role in Cancer Care
(Additional roles) AYA mental health specialist; behavior change researcher, breast cancer, specialist care models and implementation of care models, medical nutrition therapy/dietetics, physiotherapy rehabilitation (cancer specific), psychologist, supportive care, cancer survivor, AYA survivor.
Emergent Themes from Content Analysis of Qualitative Data
Consensus: Symptom Management
Indicate ≥70% agreement.
Ranking: 1: strongly agree, 2: somewhat agree, 3: neither agree/disagree, 4: somewhat disagree, 5: strongly disagree.
Consensus: Person-Centered Care
Indicates >70% consensus.
Ranking: 1: strongly agree, 2: somewhat agree, 3: neither agree/disagree, 4: somewhat disagree, 5: strongly disagree.
Results When Strongly and Somewhat Agree Were Included: Symptom Management
Ranking: 1: strongly agree, 2: somewhat agree, 3: neither agree/disagree, 4: somewhat disagree, 5: strongly disagree.
n/a, non applicable.
Inter-Rater Reliability Scores: Symptom Management and Person-Centered Care
Round I
Qualitative results
Inductive thematic saturation was achieved when no new core categories or themes were detected40–42 at interview 15; however, data collection continued with all 18 scheduled interviews. The coding process resulted in a list of initial codes (e.g., fatigue, pain, wellbeing, functional status, tailored care, unmet needs, measurement, control, motivation, flexible care models, cancer care continuum, health disparities, telehealth, and health care providers). These initial codes coalesced into seven categories with three overarching themes (Table 2). This article includes results from two themes: PA use for symptom management and person-centered cancer care in YA cancer survivors.
Round II
In round II, a 104-item survey was developed based on emergent codes and themes from round I. The survey was circulated to the initial set of experts from round I (n = 18); experts were asked to respond to each item using a 5-point Likert scale (1: strongly agree, 5: strongly disagree) with open text space for opinion expansion.
Symptom management
Experts offered their opinion on PA use for addressing a collection of symptoms and reached a consensus that PA integration in YA cancer care is part of supportive oncology (Table 3). More than 70% of experts recommended (“strongly agree”) PA use for the following: fatigue (88.9%, n = 16), cardiometabolic health (94.4%, n = 17), loss of muscle mass (100%, n = 18), excess body fat (88.9%, n = 16), low bone mineral mass (72.2%, n = 13), anxiety/depression (83.3%, n = 15), and cognitive health (72.2%, n = 13). Additional areas from developmental round II showed >70% consensus (ranked “strongly agree,” “somewhat agree”) (Table 5): PA use for pain (72.2%, n = 13), chemotherapy-induced peripheral neuropathy (72.2%, n = 13), mitigating inflammatory processes (72.3%, n = 13), creating a sense of normalcy (88.9%, n = 16), improvement of symptoms of distress (94.4%, n = 17), and lessened frailty (100%, n = 18).
Person-centered cancer care
All items, related to control and independence through PA use, reached >70% consensus by the experts; YA should be asked if they would like guidance on PA at the various stages on the cancer care continuum: prehabilitation (83.3%, n = 15), active treatment (88.9%, n = 16), post-treatment (94.4%, n = 17), and long-term survivorship (88.9%, n = 16); PA facilitates adaptation to cancer survivorship (83.3%, n = 15), identification of facilitators (94.4%, n = 17), and barriers (94.4%, n = 17) to PA (Table 4). There was consensus on conducting tailored PA assessments (72.2%, n = 13), interventions (77.8%, n = 14), and motivational assessments (77.8%, n = 14) to provide tailored PA interventions to YA cancer survivors.
Round III
Based on analyses of round II, a revised 107-item Likert survey with open response options was disseminated to the initial set of experts and an expanded sample. The sample of expert responses (n = 56) was analyzed using descriptive statistics for areas of consensus.
Symptom management
Consensus was reached that PA integration in YA cancer care is part of supportive oncology (94.7%, n = 54). More than 70% of experts recommended PA use for the following: fatigue (89.5%, n = 51), cardiometabolic health (91.2%, n = 52), loss of muscle mass (86.0%, n = 49), excess body fat (75.4%, n = 43), low bone mineral mass (70.2%, n = 40), anxiety/depression (91.2%, n = 52), cognitive health (80.7%, n = 46), and improvements in functional capacity (82.5%, n = 47) and wellbeing (78.9%, n = 45).
Person-centered cancer care
More than 70% of experts recommended PA use for the following: YA should be asked if they would like guidance on PA during prehabilitation (80.7%, n = 46), active treatment (86.0%, n = 49), immediate post-treatment (87.7%, n = 50), and long-term survivorship (93.0%, n = 53); PA facilitates adaptation to cancer survivorship in the immediate post-treatment phase and long-term survivorship (87.7%, n = 50); the identification of both facilitators (86.0%, n = 49) and barriers (93.0%, n = 53) to PA and conducting tailored PA assessments (75.4%, n = 43) and interventions (77.2%, n = 44) received consensus. Areas with <70% threshold of agreement in round III are included in Table 5.
Round IV
Complete responses from experts (n = 45) were analyzed. Percent consensus was established in 53 of 62 remaining statements (14 ≥ 90%; 23 ≥ 80%; 16 ≥ 70%; and 9 statements not achieving consensus).
Symptom management
Consensus was reached regarding PA integration in YA cancer care as part of supportive oncology (91.1%, n = 41). More than 70% of experts recommended PA use for the following: fatigue (91.1%, n = 41), cardiometabolic health (88.9%, n = 40), loss of muscle mass (86.7%, n = 39), excess body fat (77.8%, n = 35), anxiety/depression (77.8%, n = 35), improvements in functional capacity (86.7%, n = 39), and wellbeing (86.7%, n = 39). Areas that lacked consensus included the following: recommending PA for low bone mineral mass (60.0%, n = 27) and cognitive health (55.6%, n = 25).
Person-centered cancer care
More than 70% of experts recommended all items related to person-centered care through PA use: YA should be asked if they would like guidance on PA during prehabilitation (88.9%, n = 40), active treatment phase (86.7%, n = 39), immediate post-treatment phase (91.1%, n = 41), and long-term survivorship (97.9%, n = 44); PA facilitates adaptation to cancer survivorship in the immediate post-treatment phase (73.3%, n = 33) and long-term survivorship (86.7%, n = 39). In addition, the need for identification of facilitators (91.1%, n = 41) and barriers (95.6%, n = 43) to PA and conducting tailored PA assessments (71.1%, n = 32) and interventions (80.0%, n = 36) received consensus.
Discussion
With >50% of YA survivors reporting unmet needs, survival is not an adequate or equitable outcome measure for overall health and wellbeing.52,53 Supportive oncology is care given to prevent or treat symptoms to improve the QOL in those affected by cancer. 54 Previous research has reported the need for multifocal (behavioral, cognitive, and social) health promotion interventions for understudied cancer populations that incorporate long-term assessments.55,56 Expert consensus results from this study described experts' opinions on how PA could be utilized to optimize symptom management and person-centered care. This study established a strong consensus from the experts that PA should be integrated into YA cancer care as part of supportive oncology. This research adds to precision health literature by offering expert insights on PA use for symptom management to optimize biopsychosocial health tailored to YA survivors.
Symptom management
In this study, experts offered their opinion on PA use for addressing a collection of symptoms seen in YA survivors. Previous research has indicated that PA is a feasible and promising intervention to promote health and improve QOL of YA survivors.8,57–59 Experts in this study agreed that PA should be recommended to mitigate fatigue (91.1%). Previous research indicates fatigue is common and often debilitating for YA survivors and impacts physical and functional dimensions of QOL.8,60–62 Fatigue often leads to inactivity, which can perpetuate fatigue.19,20,59 This behavior is further complicated by the beliefs of some clinicians, family members, and survivors that resting is the best treatment for fatigue.21,31,62
Experts concluded that PA should be recommended when an individual experiences loss of muscle mass, anxiety/depression, or requests to lose weight. Previous research indicates that risk to metabolic, bone, and muscle health contributes to symptom burden and mortality; altered body composition, most notably excess body fat, reduced bone mineralization, and increased risk for metabolic syndrome, osteoporosis, and frailty are often seen in YA survivors. 63 PA hold promise to positively impact all of these symptoms. There was initial consensus on PA use on symptoms of frailty, but consensus lacked in subsequent rounds. Frailty in YA survivors is associated with impairment in cognitive health. 64 Interventions to combat frailty may mitigate neurocognitive decline in YAs, 65 thereby warrant further investigation.
Consensus was not reached on the use of PA to mitigate cognitive health issues. However, it is estimated that 75% of AYA cancer survivors experience cognitive changes that impact memory, learning, concentration, and decision-making. Previous observational studies of adult childhood cancer survivors indicate that PA positively impacts depressive and cognitive problems; therefore, our inconclusive finding warrants further research. 66
Person-centered care
Experts indicated that it is imperative to identify personal, structural, and systems-level facilitators/barriers to PA. In turn, consensus was reached on the need for PA interventions that are tailored to the cultural, motivational, environmental, and life-stage characteristics of YA survivors. In a recent study, young survivors articulated the need for care that “fits me.” Results from the Health Outcome and Patient Experience (HOPE) study indicate YA's have unique unmet needs (e.g., oncofertility, emotional and financial independence, body image, social impacts, and control) that are often not understood in YA survivorship care. 59 Results of this study indicate that YA should be asked if they would like guidance on the use of PA at all stages of the cancer care continuum as part of person-centered care. Interventions should be tailored by and for YA to support the critical independence associated with this developmental stage. 67
Strengths/limitations
Strengths of this research include online data collection, which allowed for geographically dispersed multidisciplinary experts from 10 countries. Their insights stemmed from diverse positionalities and care settings. The use of a measurement tool that originated from the interviews with the experts enhanced credibility. Our two-tier expert panel tested the usefulness of the measurement tool with a larger group of experts. Inclusion of open-text responses in rounds II/III provided continuous feedback for further clarification. Statements that exhibited strong consensus can also be used as a starting point by other health care providers to integrate PA in YA survivorship programs.
A potential study limitation includes characteristics of the expert panel, which may have influenced items included in the measurement tool. To assess inter-rater reliability on emerging areas of consensus, considering changes of measures of central tendency and dispersion may offer a more accurate assessment. Therefore, both descriptive statistics and Kappa scores were included. Although overall inter-rater reliability, when measured by Kappa scores, lacked robustness, previous researchers indicate that low Kappa scores are not indicative of poor inter-rater reliability because the goal of a Delphi study is to converge on consensus. 59 The diversity of clinical experts and their confidence to comment on specific issues and the changing composition of the expert panel over the subsequent rounds may have impacted the Kappa scores. Subsequent rounds with the same expanded group of experts would have provided better inter-rater reliability scores. 39 YA cancer survivors were not explicitly included in this study, which may limit the findings' transferability. Any findings herein should be validated with YA for their critical and lived experience with cancer survivorship.
Conclusions
Experts in this study highlighted how PA use in cancer survivorship provides biopsychosocial health benefits while offering autonomy, self-management, and independence critical to the YA life stage. PA should be offered to YA as part of supportive oncology at all stages of the cancer care continuum. Furthermore, as a precision-health measure, interventions should be tailored to accommodate individual facilitators, barriers, preferences, motivation, and stages in the cancer continuum.
Guidance and guidelines are needed to support YA survivors and foster the integration of PA into survivorship care among health care/community teams. Experts articulated that the integration of PA in YA survivorship care goes beyond individual factors and extends into structural frameworks that are needed to disseminate and implement PA guidelines. Given the propensity of unmet needs in YA survivors, areas that lacked consensus in this study (cognitive health, pain, nausea/vomiting, chemotherapy-induced peripheral neuropathy, mitigation of cellular inflammation, low bone mineral mass, symptoms of frailty, a sense of normalcy, and symptoms of distress) warrant further research. These results offer a blueprint to guide future PA symptom management research and clinical endeavors. Key takeaways and additional resources are given in Figures 2 and 3.
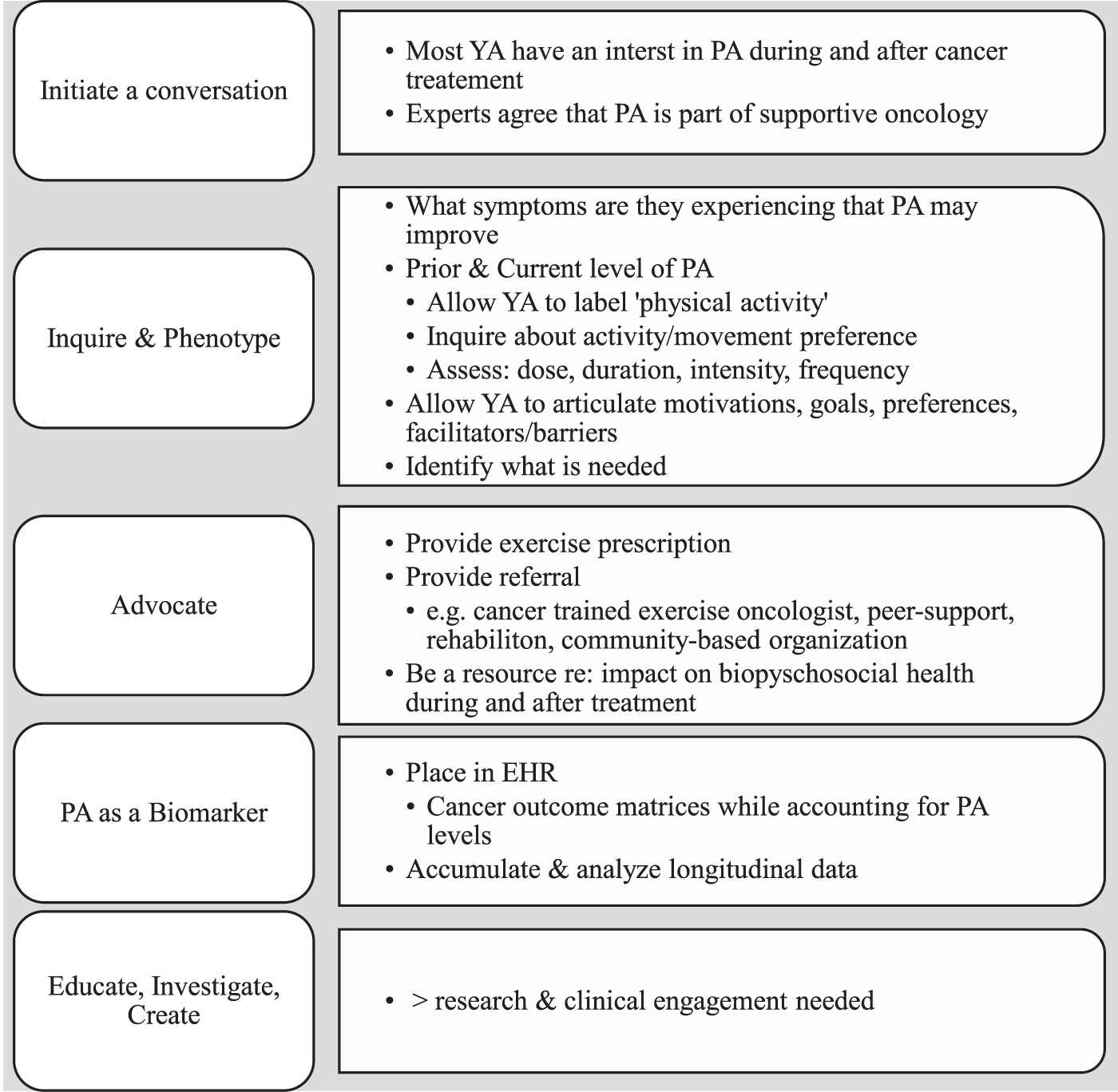
Knowledge translation: key points.
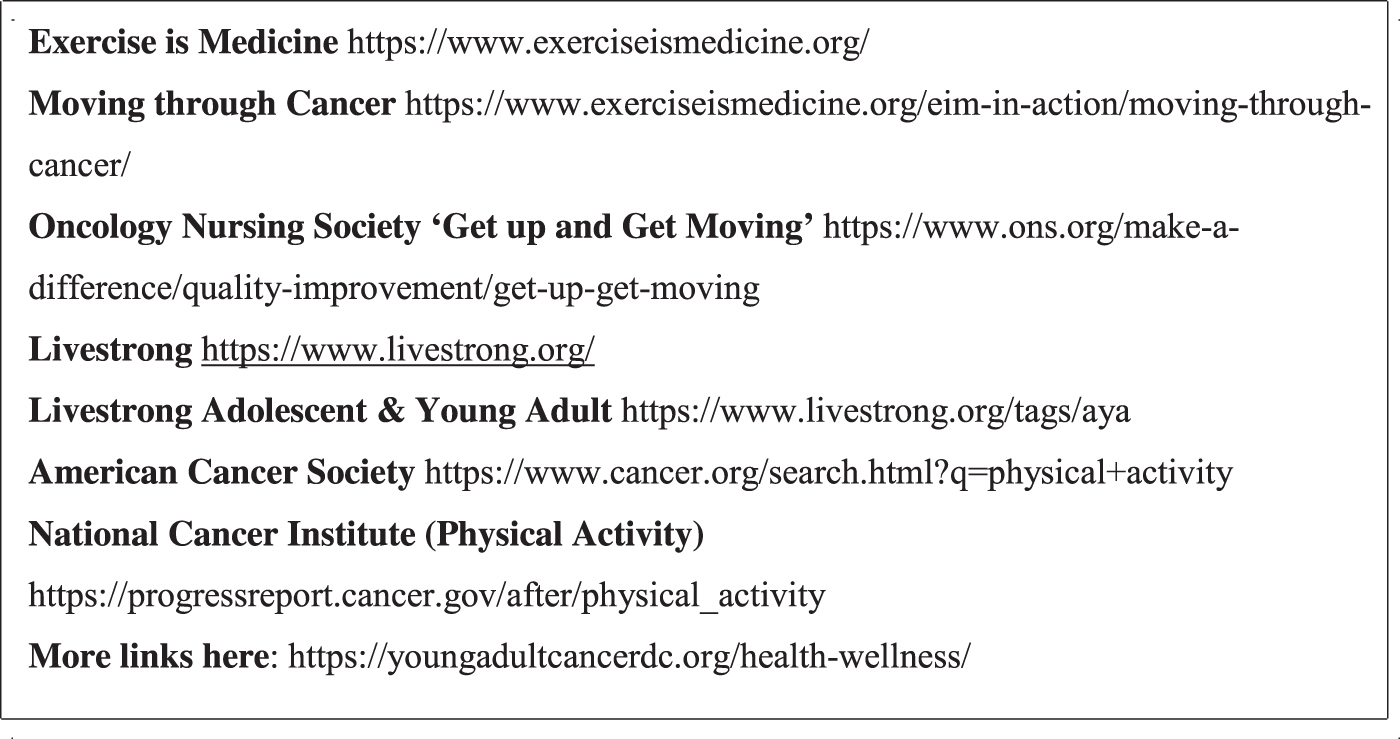
Additional resources related to physical activity and cancer.
Surviving cancer is not enough; precision-health interventions that mitigate the “consequences of the cure” are needed. 68 Clinical guidelines to facilitate PA implementation on the YA cancer care continuum could facilitate its use as a symptom management strategy. Symptom management and person-centered care exist in structural systems that ultimately impact translation from expert recommendations to further research, dissemination, and implementation efforts. There is an urgent need for translational research that addresses structural realities of care delivery and clinical considerations relevant to the facilitation of PA integration into YA survivorship care.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Sigma International Honor Society of Nursing Beta Zeta at-Large Chapter.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.