
Abstract
Purpose:
Osteosarcoma is a typical malignancy of childhood and adolescence. Recurrences usually occur early, but rarely may arise after decades of remission. Little is known about these very late events and we set out to fill this knowledge gap.
Methods:
The database of the Cooperative Osteosarcoma Study Group (COSS) was searched for patients with a first recurrence of a high-grade central osteosarcoma occurring >10 years after diagnosis of the primary disease. Identified patients were analyzed for demographic, tumor-, and treatment-related factors as well as outcomes.
Results:
Among a total of 1,178 10-year relapse-free survivors, 17 affected patients were identified. Only five of these had a documented good response to initial chemotherapy. No presenting factor was identified to predict these very late events. Prognosis was generally very poor despite intensive multimodal therapy. Inoperability of the recurrences seems to have constituted a major limiting factor.
Conclusion:
Osteosarcoma patients should be followed for potential recurrences for well >10 years from initial diagnosis. Only through such an extended truly long-term follow-up and a structured transition of young patients can these be detected while they are still operable and, hence, potentially curable.
Introduction
High-grade central osteosarcoma is among the most frequent malignant solid tumors of older children, adolescents, and young adults. Prognosis was dramatically improved with the addition of (multidrug) chemotherapy to complete surgical resection. Recurrences mainly involve the lungs and bones, with other organs only rarely involved. 1 The median time to recurrence is brief. In the large experience of our Cooperative Osteosarcoma Study Group (COSS), the median time between biopsy of the primary and first recurrence was found to be only 1.6 years from initial diagnostic biopsy, and only 5% of these recurrences arose after >5 years. 2
The prognosis of patients with recurrence is mainly determined by their ability to achieve a second complete surgical remission. However, long-term survival is related to time to recurrence, with early recurrences being associated with particularly poor survival. Later recurrences seem to be associated with a more favorable prognosis.2–4 However, some patients may develop recurrent osteosarcoma many years or even decades after initial treatment. The natural history of these very late recurrences is poorly understood and limited to case reports,5–7 small subcohorts of relapsed case series, 8 and rare epidemiological studies. 9 Because of their relative infrequency, very little is known about clinical features, tumor characteristics, treatments, and disease-specific outcomes of affected patients.
COSS has performed neoadjuvant osteosarcoma studies and registries since 1980.10,11 As of now, it has registered several thousand high-grade central osteosarcoma patients, with theoretically unlimited follow-up. This allows us to investigate later tumor-related events with reasonable patient numbers. Therefore, we here report our group's experience with first recurrences detected >10 years after initial osteosarcoma diagnosis.
Patients and Methods
The database of the COSS was searched (06/30/21) for all patients with previously untreated primary high-grade central osteosarcoma who developed a first tumor recurrence at any site >10 years after initial diagnostic biopsy. All COSS patients and/or parents, whichever appropriate, had given their informed consent to treatment, data capture, and unlimited follow-up. All study and registry protocols were approved by the appropriate ethics committees.
All patients had originally been treated according to the COSS regimen active at the time of enrolment, consisting of neoadjuvant and adjuvant multidrug chemotherapy and surgery.10,11 Only patients who achieved a complete surgical remission of all affected sites were considered eligible. Affected patients were then analyzed for age at initial presentation, gender, tumor site and size, and primary metastatic status as well as for treatment. Tumor response at initial definitive surgery was coded according to Salzer-Kuntschik et al., 12 with a good response assumed when the tumor was <10% viable. Patients with late recurrences were then analyzed in detail for presenting factors, treatments, and outcomes.
Survival outcomes were calculated using the Kaplan–Meier method. 13 Overall survival was calculated from the date of relapse diagnosis until death from any cause. Event-free survival was calculated until the date of diagnosis of any renewed osteosarcoma manifestation or death from any cause, whichever occurred first. Only patients who achieved a surgically complete (second) remission were considered to have been made disease-free, all others were coded as having suffered an event at day 1 after recurrence. Secondary malignancies were not counted as events, but analyzed separately.
Results
Among a total of 1,178 10-year relapse-free survivors in the COSS-database, a total of 34 with a first tumor recurrence detected >10 years from the original diagnostic biopsy were identified. Among these, four did not have osteosarcoma (two dedifferentiated chondrosarcoma, one solitary fibrous tumor, one leiomyosarcoma of bone), eight had osteosarcoma variants (three low-grade central, three parosteal, one periosteal, and one high-grade surface). Five additional patients had been pre-treated before inclusion into the database and were only registered upon recurrence (four as osteosarcoma and one under an erroneous diagnosis), leaving 17 patients for further analyses (Tables 1 and 2).
Characteristics at Initial Osteosarcoma Presentation
Years at initial diagnosis of osteosarcoma.
Of the involved bone.
Li–Fraumeni syndrome.
Preceding liposarcoma.
Rothmund–Thomson syndrome.
Melanoma between osteosarcoma manifestations.
A, actinomycin D; Ca, carboplatin; D, doxorubicin; I, ifosfamide; M, high-dose methotrexate; P, cisplatin; POP, primary operation; prox., proximal; V, vincristine.
Characteristics at Osteosarcoma at Relapse, Therapy, and Outcome
Secondary malignancy (pulmonary adenocarcinoma).
Unilateral.
Bilateral involvement.
Fungal pneumonia.
Pleura involved.
Pleural effusion.
Laterality unknown.
This patient also received pazopanib, denosumab, and zoledronate.
Lung-embolus during osteosarcoma progression.
Local recurrence of the first lung metastasis.
Ca, carboplatin; CR, complete remission; Cy, cyclophosphamide; D, doxorubicin; E, etoposide; I, ifosfamide; M, high-dose methotrexate; P, cisplatin; REC, recurrence; To, topotecan; Tr, trofosfamide.
There were 10 (59%) affected males and 7 (41%) affected females. Two of these (12%) carried a known tumor predisposition syndrome (one Li–Fraumeni syndrome and one Rothmund–Thomson syndrome). The median age at initial osteosarcoma diagnosis had been 17 (range: 3–35) years. The reported symptom interval before biopsy was known for 11/17 patients and was a median of 39 days (range: 10–208). Information on osteosarcoma subtype was available in 13/17 patients (76%). Of these, 6 (46%) were classified as osteoblastic, 5 (38%) as chondroblastic, and 2 (15%) as teleangiectatic.
Primary tumors had involved the distal femur in nine patients, the proximal tibia in three, the pelvis in two (ilium one and ischium one), and the proximal humerus, femur, or fibula in one each. Of 13 patients with available data, 8 primaries (62%) had been <1/3 of the bone of origin and 5 (38%) larger (2 trunk, 2 relative tumor size unknown). Five patients (27%) were reported to have developed pathological fractures. None of the 17 patients had had primary metastases. The duration of time between diagnostic biopsy to initiation of chemotherapy was a median of 6 days (range: 0–24). Primary treatment had involved neoadjuvant and adjuvant chemotherapy in 16/17 (94%) patients and was postoperative only in 1 (6%). Chemotherapy had lasted a median of 272 (141–354, n = 16) days.
Patients were reported to have received a median of four3–6 chemotherapeutic agents. The drugs reported for first-line treatment included doxorubicin, high-dose methotrexate, and cisplatin in all 17 patients (100%), ifosfamide in 15 (88%), carboplatin in 2 (11%), and vincristine/actinomycin D in 1 (6%). No patient had received radiotherapy or targeted therapy first line. Surgical resection and reconstruction of the primary osteosarcoma was reported as rotationplasty in six (35%), amputation in five (29%), and limb-salvage in six (35%, including the two patients with primaries of the trunk). Response to neoadjuvant chemotherapy was available for 15 (88%; 1 postoperative chemotherapy only and 1 no data) patients. Among these, response was good (<10% viable tumor) in 5 (33%) and poor in 10 (67%).
Very late recurrences were detected after a median of 16.7 (10.1–22.7) years from initial diagnosis. Among 12 patients with relevant information available, identification was based on symptoms in 9 (75%; pain 4, swelling 2, and pneumothorax, hemoptysis, and problems associated with paralysis of the diaphragm 1 each), by routine imaging in 2 (17%), and due to laboratory abnormalities in 1 (8%).
The late recurrences affected distant sites in all 17 (100%) patients, 1 patient with a pelvic primary also had a concurrent local recurrence (6%). Eleven (65%) recurrences were solitary and six (35%) involved >1 lesion, four (24%) of the latter in more than one organ system (3 two, 1 three). Metastases affected the lung(s) in 12 (71%; 9 uni-, 2 bilateral, 1 unknown), bones in 6 (35%), and other sites in 4 patients (24%; one each liver, kidney, brain, muscle) each (multiple mentions possible).
Therapy for late recurrences included chemotherapy in 11 (73%) (3 only preoperative, 4 only postoperative, 2 both, and 2 no surgery) and 4 (27%) did not (2 unknown). Multiple drugs (median 4, range 2–7) were again employed in all 10/11 cases with available information. Drugs employed in these were ifosfamide and etoposide in eight patients each, high-dose methotrexate in six, cisplatin and carboplatin in five each, doxorubicin in four, cyclophosphamide in two, and trofosfamide and topotecan in the same one patient. The latter also received pazopanib, denosumab, and zoledronate.
Eleven (65%) patients underwent documented surgical resection of relapsed disease resulting in a second complete surgical remission in 10 of the 11 patients. Four additional patients did not undergo surgery and it was unknown in an additional two patients. Radiotherapy ranging from 35 to 63 Gy was administered to 5 (36%) patients, and 9 (64%) received none (3 unknown). Two patients received adjuvant radiotherapy, one radiotherapy after incomplete surgery, and two received radiotherapy instead of surgery.
Follow-up information after recurrence was available for 16/17 patients. These 16 were followed for a median of 4.1 (range: .4–18.9) years from first recurrence, 12 being followed for >1 year and 6 of these for >5 years. At last follow-up, 7 of these 16 patients were alive: 5 (31%) were in complete surgical remission (four in 2nd and one in 3rd remission), 1 (6%) was alive with disease at first recurrence, and for 1 patient the disease status was unknown.
Causes of the nine deaths occurring after a median of 4.8 (.4–12.4) years from relapse were progressive osteosarcoma in six patients (four 1st, one 2nd, and one 3rd recurrence), secondary malignancy during a third remission (adenocarcinoma of the lung, this patient had also developed a liposarcoma between the osteosarcoma episodes), fungal pneumonia during a sixth remission, and pulmonary embolism during second osteosarcoma progression in one patient each. One further patient who later succumbed to the late osteosarcoma recurrence developed a melanoma in the interval between her osteosarcoma episodes.
Median overall survival after late recurrence for all 16 patients with follow-up information was 78% (95% confidence interval: 11%) at 2 years, 53% (14%) at 5 years and 10 years, and 18% (15%) at 15 years. For the 15 patients with information on disease status, 2-year event-free survival was 44% (14%), it was 18% (11%) at 5 years. Only two patients were event-free beyond 5 years, both without further events (Fig. 1).
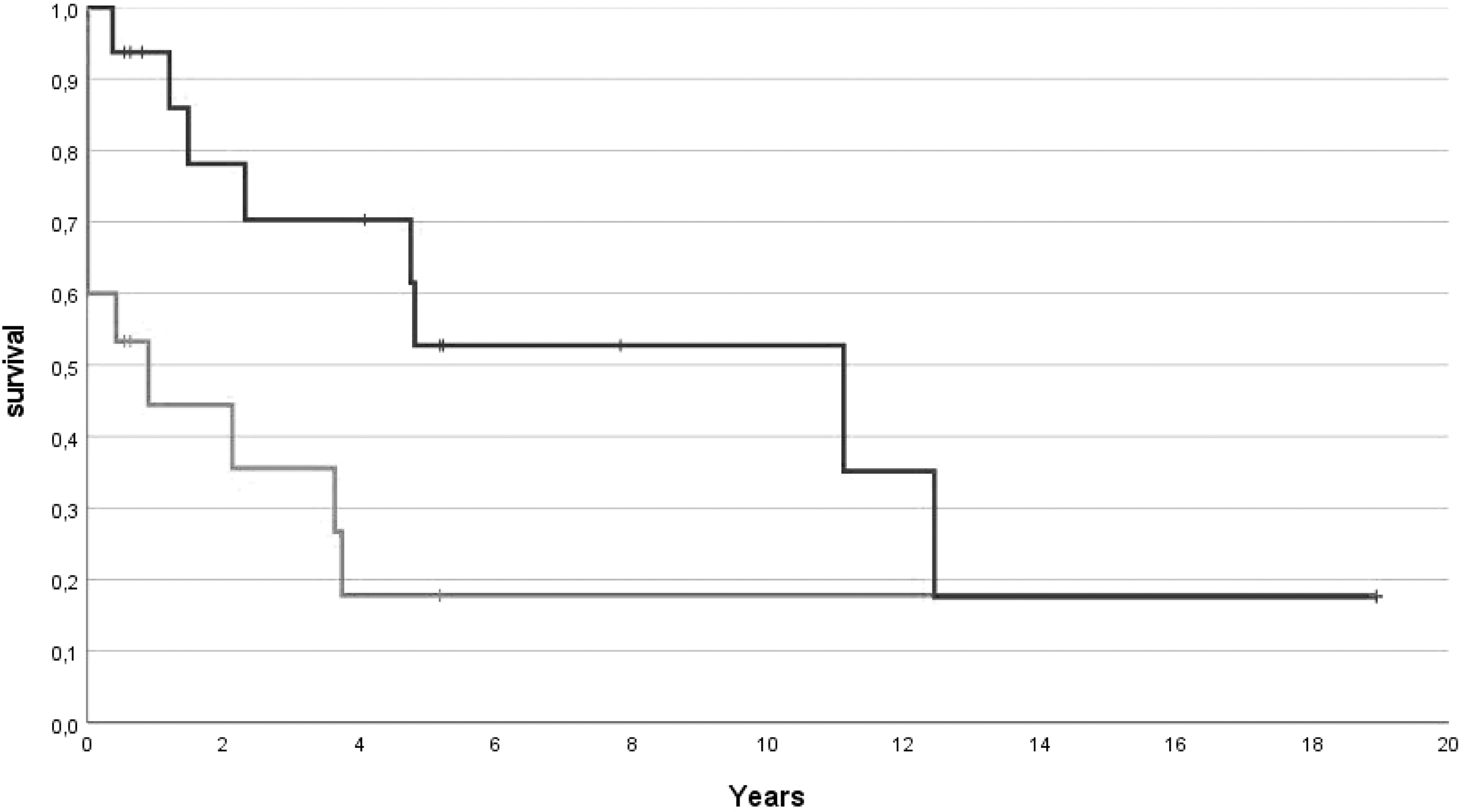
Overall (blue, evaluable: n = 16 patients) and event-free (red, evaluable: n = 15) survival after detection of the late osteosarcoma recurrence.
Discussion
This analysis undoubtedly demonstrates that osteosarcoma patients are not safe from their malignant disease even after many years of relapse-free follow-up. Our data clearly show that osteosarcoma recurrences may appear after even more than one or even two decades of remission. This clinically important finding has major implications for long-term follow-up. Our data also demonstrate that affected patients have a high risk of succumbing to these ultra-late events. This argues for a truly extended tumor-directed follow-up and calls for a structured transition of pediatric patients into young and even older adult care.
At present, there is no way to decipher if the first and the later disease bouts were indeed caused by the same osteosarcoma as primarily or were the result of two distinct primary osteosarcomas. The late lung metastases we observed were clearly what their name suggests: Metastases. As others 14 and congruent with our group's data on solitary bony recurrences in general, 15 we can only assume that some of the alleged osseous relapses indeed represented second primary tumors. Their appearance at typical predilection sites for osteosarcoma development would argue in this direction.
It, therefore, seems adamant that all osteosarcoma patients be screened for underlying tumor predisposition syndromes at first presentation. Such were also detected in two of our patients. Recent findings suggest that a genetic tumor predisposition may be present in around a quarter of patients with osteosarcomas, 16 particularly in young children. Whatever the ultimate cause of these untoward late tumor events may have been: Our data demonstrate that former osteosarcoma patients require a truly extended tumor-directed follow-up, beyond the typical 5- to 10-year follow-up period employed by the majority of treating providers and institutions.
It becomes clear that no age or gender is safe from these very late events. The inclusion of several patients who were uncharacteristically young when they first were diagnosed with osteosarcoma again suggests the potential role of a genetic predispositions; however, we also observed ultra-late recurrences in patients initially diagnosed as adolescents and young adults. Also, there was no primary tumor site that seemed to be predictive of late recurrence. The two eldest patients in our series were also those with pelvic primaries. This may reflect the changing distribution of primary tumor sites with age. Primary metastases were notably absent in the analyzed cohort of patients with very late relapses. Affected patients seem to have succumbed to their disease or, in rare cases, were truly cured earlier in the course of their disease.
Treatment-related factors that predisposed patients to late recurrences were not detected in our study. All patients received first-line intensive chemotherapy and no patients received radiation therapy, both of which are known to predispose patients to second primary malignancies, including osteosarcoma. 17 The response rate to chemotherapy administered during the primary disease episode seemed rather low compared with our group's general experience. 10 However, such a low response rate may be expected for recurrences in general.2,3
The vast majority of our very late recurrences were detected by clinical findings rather than by follow-up imaging. This may be very relevant for the duration during which the latter should be offered. Usually, imaging is recommended for five or, at the maximum, 10 years after treatment for cancer and then stopped, as the patient is considered cured. However, osteosarcoma metastases, especially those in the lung, will most often not cause significant pain or other symptoms until they have grown considerably, their operability is limited, and their prognosis is, therefore, poor to dismal.2–4 Earlier detection may save lives. We, therefore, again argue for prolonged regular pulmonary imaging, well beyond what is nowadays generally considered adequate.
Several of the known classical osteosarcoma subtypes were affected by these late recurrences, with the notable exception of fibroblastic primaries. Numbers were low, so that it remains speculative if this was truly due to a different tumor biology or a finding by chance. The mainly young adult age distribution at which the osteosarcomas recurred reflected the primarily pediatric and adolescent age of first involvement. About two thirds of the late recurrences involved only one lesion, a fact that has to be considered prognostically favorable, operability presumed. 2
There was only one local relapse, in the trunk, pointing to both the rarity of late local events in general 18 and to a potentially distinct biology of axial osteosarcomas. The distribution of recurrences otherwise broadly reflected that expected for osteosarcoma relapses in general,2–4 with the lungs being the most commonly affected site, followed by distant bones. Somewhat more patients than considered usually expected presented with such osseous involvement, again pointing to the possibility of second primary malignancies.
It is remarkable that most patients again received intensive chemotherapy second line. We generally reserve such for patients with recurrences arising within 3 years from first-line treatment or later relapses with multiple sites of involvement. Nevertheless, patients received at least what would be considered adequate systemic relapse therapy, if not more. Given the rarity of such treatments, we cannot comment on the putative efficacy of newer systemic therapies such as tyrosine-kinase inhibitors. It seems advisable to include eligible patients into clinical trials of innovative drugs, should those be available.
A majority of our patients again achieved a complete surgical remission of their osteosarcoma recurrence and, therefore, what is considered somewhat of a prerequisite for cure. 19 Relapse sites and especially an extensive spread at detection may have interfered in the others. Radiotherapy at varying doses was given as somewhat of a last resort to some. Regardless of their intensive second-line therapy, the prognosis of the patients in our cohort with adequate follow-up data was poor and similar to patients with earlier recurrences.2–4 Again, it seems very important to find these late events earlier, when they are still small, limited, and hence treatable.
In summary, very late osteosarcoma recurrence may occur in a small percentage of adolescents and young adults. They primarily affect the lungs and distant bones. The prognosis of patients with very late recurrences is guarded and they are only potentially curable if complete surgical resection is possible at the time of detection. Our results clearly argue for an extended tumor-directed follow-up through all of adolescence, young, and even later adulthood. Specific survivorship-clinics seem to be an appropriate infrastructure in which such an extended surveillance could be offered. Osteosarcoma groups should think about extending the period during which they recommend tumor-directed follow-up well beyond 10 years.
Footnotes
Acknowledgments
We thank all patients and parents as well as the staff of all participating institutions.
Author Disclosure Statement
L.K. reports having acted as advisory board member for Amgen, Agios, Bayer, and Novartis. T.W. reports grants from Orthopediatrics and Orthofix. S.S.B. reports having acted as consultant and/or advisory board member for Bayer Healthcare, Boehringer Ingelheim, Hoffmann-La Roche, Ipsen, and Eli Lilly. All these financial relationships were outside the scope of submitted study. S.H.-N., T.K., D.B., C.B., G.F., T.v.K., M.K., R.M.-S., R.S., and B.S. report no conflicts of interest.
Funding Information
The studies from which these patients originate were supported by Deutsche Krebshilfe (DKH T10/96/Bi, DKH 70-02160, DKH 50-2723-Bi2), Deutsche Forschungsgemeinschaft (BI 1045/1-1, BI 1045/1–2), Fördergemeinschaft Kinderkrebs-Zentrum Hamburg, and Förderkreis krebskranke Kinder Stuttgart.