
Abstract
Purpose:
Financial concern is a major issue for adolescent and young adult (AYA) cancer patients. Furthermore, unaddressed oncofertility challenges (e.g., infertility) are linked to psychological distress and decreased overall quality of life. Little is known about how financial concern in terms of oncofertility (i.e., concern regarding affording fertility preservation [FP] services) impacts AYAs' decision making and experiences.
Methods:
AYA cancer patients (n = 27) aged 12–25 years whose cancer treatment conferred risk of infertility were recruited through electronic health record query. Participants completed semi-structured interviews, which were recorded, transcribed, and deductively coded for themes related to information needs, knowledge of treatment effects on fertility, and reproductive concerns after cancer. Emergent, inductive themes related to financial concern were identified. The Institutional Review Board at the University of Michigan approved this study (HUM#00157267).
Results:
Financial concern was a dominant theme across the qualitative data. Emergent themes included (1) varied access to health insurance, (2) presence of parental/guardian support, (3) reliance upon financial aid, (4) negotiating infertility risk, and (5) lack of preparation for long-term costs. AYAs relied heavily upon parents for out-of-pocket and insurance coverage support. Some participants sought financial aid when guided by providers. Several participants indicated that no financial support existed for their circumstance.
Conclusions:
Financial consequences in terms of oncofertility are a major issue affecting AYA cancer patients. The incidence and gravity of financial concern surrounding affording oncofertility services merits attention in future research (measuring financial resources of AYAs' parental/support networks), clinical practice (strategically addressing short- and long-term costs; tailored psychosocial support), and health care policy (promoting legislation to mandate pre- and post-treatment FP coverage).
Introduction
Economic distress resulting from cancer treatment can yield a variety of negative financial impacts including bankruptcy, asset depletion, medical debt, poor treatment adherence, and poor disease outcomes.1–4 The high cost of treatment, the impact of disease on vocational and educational attainment, and difficulty to access health insurance coverage create conditions that often preclude affordable treatment. 5 Entry-level salaries, student loans, tuition costs, and lack of health insurance particularly hamper adolescent and young adult cancer (AYA) patients (aged 15–39 years). 4 Compared with older peers, AYAs may encounter additional treatment-related expenses, such as the cost of fertility preservation (FP) and use of assisted reproductive technology (ART) for family building. 6
Risk of infertility is a significant source of uncertainty and distress.7–16 FP/ART are inconsistently covered by health insurance and out-of-pocket oncofertility costs constitute some of the highest medical expenses for AYAs. 2 In the United States, FP options for men (e.g., sperm banking, testicular sperm extraction, electroejaculation) costs between $1000 and $12,000 and options for women (e.g., egg, embryo, or ovarian tissue freezing) range from $10,000 to $15,000, before annual storage fees. 17 The average cost of a single IVF cycle is $12,400, with total costs ranging from $40,000 to $60,000 per live birth by IVF. A gestational carrier may cost between $100,000 and $150,000, and domestic adoptions may range $30,000–$40,000.5,18–21
To manage costs, AYAs have demonstrated increased reliance upon crowdfunding campaigns on platforms such as GoFundMe.22,23 Financial assistance programs offer some support to eligible patients for pretreatment FP.24–26 Many AYAs rely on their parents’/guardian's health insurance, which are mandated by The Affordable Care Act to cover dependents until the age of 26. 27 Yet, even with parental/guardian support, many AYAs lack adequate insurance for FP services.28,29
Little is known about how significantly these financial pressures and barriers impact AYA decision-making surrounding FP, or about the varied experiences of oncofertility and associated financial effects across the AYA age range. This study aimed to explore the overall experiences of AYAs who encounter potential iatrogenic infertility, and the ways in which financial concerns impact FP decision-making strategies. The “AYA” population contains three theoretical subgroups: mid/late adolescence (15–17 years), emerging adults (18–25 years), and young adults (26–39 years). 30 Because young adult ages 26–39 are more likely to already have children or to pursue conception immediately, and because FP is feasible as soon as postpubertal, we focused on AYAs aged 12–25.31–34
Methods
Sample
Figure 1 provides the sampling process. Participants were recruited from adult and pediatric oncology units within an NCI-Designated Comprehensive Cancer Center from October 2019 to August 2020. Eligibility criteria included the following: age 12–25 years, diagnosed within the previous 2–12 months, and at-risk for infertility owing to diagnosis or prescribed curative treatment exposures (e.g., solid tumors, surgeries, cytotoxic and radiation therapies that affect reproductive organs, and/or hormonal levels)35–37 .
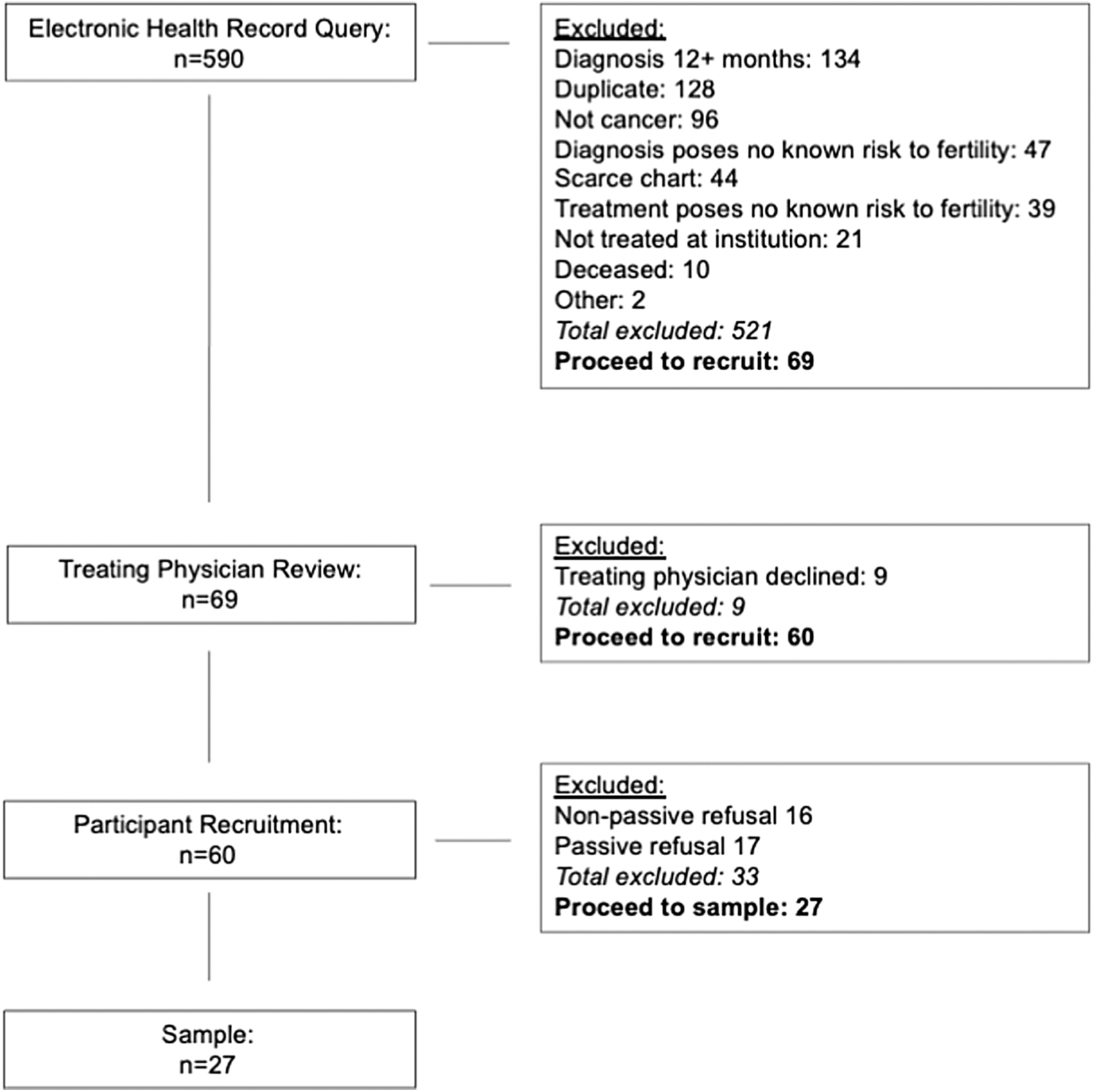
Recruitment of adolescents and young adults. Participants were recruited within an NCI-Designated Comprehensive Cancer Center and were identified via EHR query based upon ICD-10 codes. Query results (n = 590) were screened by medical personnel who eliminated n = 521 ineligible patients. N = 69 individuals were deemed eligible for recruitment. Study staff contacted eligible patients' treating oncologists by email and offered a 7-day opt-out period. Nine eligible individuals were excluded in this manner. Remaining eligible patients (n = 60) were contacted by phone. Active nonrespondents (n = 16), and passive nonrespondents were eliminated (n = 17). A total of n = 27 participants comprise the final sample. EHR, electronic health record.
Participants were identified via electronic health record (EHR) query using ICD-10 codes. Query results (n = 590) were screened by medical personnel who eliminated n = 521 ineligible patients. Individuals deemed as potentially eligible for recruitment equaled n = 69. Before recruitment, study staff contacted eligible patients' treating oncologists by email and offered a 7-day opt-out period to refuse participation on behalf of their patient, based on the oncologists' discretion given the sensitive nature of the study. Nine eligible individuals were excluded in this manner. Remaining eligible patients (n = 60) were then contacted by phone one time per week for up to 3 weeks. Active nonrespondents who declined to participate (n = 16), and passive nonrespondents who did not respond after three contact attempts were eliminated (n = 17). A total of n = 27 participants comprise the final sample.
Procedure
Participants older than 18 years were emailed/mailed informed consent documents. Guardian consent/minor assent were sent to participants younger than the age of 18 years.
Sixty-minute, audio-recorded interviews were scheduled with one of four interviewers (lead interviewer: NI; interviewing team NJL, DS, AZ). Interviews consisted of administration of a battery of standardized instruments immediately followed by a semi-structured interview via HIPAA-approved confidential video-conferencing software, by telephone, or in person on-site at the outpatient clinic. Three major sections addressed (1) general cancer experience (e.g., Can you tell me the story of how you were diagnosed with cancer?), (2) goals and dreams for the future including desire to have a family someday (e.g., What are some of your goals and dreams for yourself? Do you see yourself having kids and a family one day?), and (3) experiences with FP (e.g., When you were making decisions about preserving your ability to have kids in the future, what was your experience like seeking help from your providers; Is there anything about your decision that makes you uncertain?).
Following conclusion of the interview, participants were provided with a $25 gift card. The Institutional Review Board at The University of Michigan approved this study (HUM#00157267).
Data analysis
Demographic information collected from EHR and self-report included sex, race, age at diagnosis, clinical unit, cancer type, and whether FP occurred. Interviews were professionally transcribed by a HIPAA-compliant transcription service. Research assistants reviewed transcriptions for accuracy and de-identified transcripts. The second and third authors independently coded n = 27 transcripts using a deductive coding schema derived from the empirical literature addressing information needs,38,39 knowledge about treatment effects,39–41 and reproductive concerns after cancer.42–44 Content and codes that emerged inductively were also identified. Coders met monthly to discuss and resolve discrepancies. Final codes were compiled into a master document and the first author reviewed and extracted inductive codes that were then grouped into themes.
Results
Demographics
The sample included 63% male and 37% female respondents. At age of diagnosis, participants were 18–25 years (59%) and 12–17 years (41%). Racially, white participants comprised 78% and nonwhite participants comprised 22%. Roughly half of the sample (n = 14) received treatment in the adult clinical unit. Nonsolid cancers constituted 52% of the cancer types. Most participants aged 18–25 years (n = 11) preserved fertility, as did most participants aged 12–17 years (n = 6) (Table 1).
Demographics of the Adolescent and Young Adult Cancer Patient Sample
Cancer types: Hodgkin's lymphoma n = 9; synovial sarcoma n = 3; osteosarcoma n = 3; acute lymphocytic leukemia, n = 3; acute myeloid leukemia n = 2; testicular n = 2; ovarian tumor n = 1; pineoblastoma n = 1; laryngeal n = 1; nasopharyngeal n = 1; nerve sheath tumor n = 1.
Emergent themes
Varied access to health insurance
Varied access to health insurance emerged as a theme. Ironically, one 24-year-old referred to FP itself as an “insurance policy” for his future fertility. Many participants discussed relying on their parents' health care coverage. As one 24-year-old noted, “I'm still on my dad's health insurance, ‘cause I'm not 26 yet and [I'm] unemployed…But his insurance did not cover it [FP].” Many participants speculated about whether coverage was an option or if their parents used it, noting “[I think] they looked into it, but I don't know if it [FP] was covered.”
Some participants discussed limited aspects of FP falling under coverage. One 23-year-old's parents' insurance covered Lupron injections (“thankfully”) to protect her ovarian reserves but did not cover other aspects of FP treatment, such as egg retrieval and storage. AYAs with access to insurance coverage acknowledged this indemnity as “fortunate,” “lucky,” “working in my favor.” However, many resented that insurance did not cover FP, which is “stupid” according to one 18-year-old. One 23-year-old critiqued the lack of universal coverage of a “normal” health care need such as oncofertility:
It doesn't really make sense that it [FP] is not covered. I guess it's just because—I assume when IVF and sperm banking first became a thing, I would imagine there were people opposed to it, like their religious right. I assume that is part of the reason why insurance still doesn't cover it, like contraceptives and stuff. It felt from my experience, like … this is a normal thing. Everyone in my position is doing it. Why would it not be covered by insurance?… I still have to pay $75 bucks a year [for storage fees]. I guarantee you in Sweden, they don't have to do that.
Unfortunately, in some cases no insurance coverage was accessible. As one 25-year-old described, “My insurance didn't cover it [FP]. I was, like, well, that's not really an option for me right now.”
Presence of parental/guardian support
Several participants discussed the presence of parental/guardian support. In fact, many noted that affording FP was only made possible because of access to guardian support. The common sentiment of gratitude and relief surrounding parental financial support was exemplified by a 24-year-old:
If I was doing this FP on my own, the cost was definitely something that would have been prohibitive, if not for the fact that my parents will cover this [for me] … luckily, I'm blessed enough that my parents had enough money that we didn't have to worry about the cost of storage, so it didn't even really feel like a decision.
Another 19-year-old echoed this sentiment, adding an appreciation for the freedom of reproductive choice that accompanied solvency:
My parents basically covered the cost of all this stuff [FP], so I didn't have to worry about that. I could basically choose the decision that worked best for me and my parents. There wasn't a decision that I was like, ‘Oh, I can't do this because of money’ or something. I was basically free to choose what I wanted. I wasn't restricted.
While many participants expressed gratitude for their parents' means, some also expressed guilt for drawing so heavily upon their family's resources. One 23-year-old clearly articulated this paradox:
I believe it [the cost of FP] was between $1000 and $15,000. They [my parents] said, ‘We're gonna do whatever needs to be done.’ We're lucky enough where my parents both have jobs, and we live a very comfortable life where that was never an issue. Although I will say – and thank God, my parents aren't here [in this interview] ‘cause I would not say this out loud – but I felt a little guilty.
Other participants sensed their parents purposefully shielded them from financial information to preclude feelings of guilt. As one 20-year-old said, “My parents were really vague on not wanting me to know… how much it cost … they just didn't want me to worry.” She noted that “whenever prices and stuff did come up, she [my mom] would just talk to the doctors about it” and added with an awkward laugh, “I don't really know much about that [the financial] part.” Another 17-year-old remarked that her mom quietly “handled” the financial aspect, including strategizing to maximize the investment by storing eggs in a different state “’cause it's cheaper.” When asked about whether the cost of FP affected her decision, she responded “Honestly, I don't know but my mom said it didn't.” Some participants lacked financial support from parents or support networks. As one 21-year-old said, “I wasn't gonna be able to afford it, and I didn't have anyone to help me … so I just let it go.”
Reliance upon financial aid
Several participants raised discussion of financial aid resources. Many reported learning about support programs through providers—especially nurses—or from members of their social networks. Financial aid helped “offset some of the costs…which was huge.” Others paired aid with GoFundMe campaigns. Some strategized with aid organizations to store gametes in states with lower fees. For some, financial aid tipped the scales toward deciding to preserve, saying “I figured [with financial support], I might as well.” As one 17-year-old stated:
Initially when we first heard what it cost, I didn't wanna do it. ‘Cause without any [financial aid] it's $400 to store it or somethin’, which I didn't know if that's worth it especially if I don't know if I wanna use it [preserved sperm] … Fortunately, there were programs to help me, but if there hadn't been… I probably wouldn't have been onboard.
Negotiating infertility risk
Negotiating infertility risk (i.e., weighing risk of potential infertility vs. cost of FP) surfaced as a theme. For many participants, even minimal risk merited FP, regardless of the financial cost. Upon learning of his risk, one 23-year-old “immediately” decided to preserve and said that the cost “didn't matter.” Another 18-year-old said his decision was “not really” affected by the financial cost because he was “going to [preserve]” regardless.
Some participants spoke of strategically maximizing their investment in FP. One 24-year-old noted that he banked sperm twice because the storage cost was a flat rate, and it was only a “marginal increase in cost” to do “one more session.” One 16-year-old discussed weighing the risk of FP expenses if his fertility may not ultimately be impacted, questioning, “‘Do we want to pay this much, or we could save the money’ … was the cost worth fixing that low percent of it [infertility]?”
In some cases, participants felt agnostic about having children in the future and chose not to preserve. One 19-year-old decided not to preserve regardless of the cost. He held a fatalistic outlook on having children (“if it happens for a reason, it happens”). It is notable that solely male speakers raised concern about negotiating infertility risk.
Lack of preparation for long-term costs
Lack of preparation for the long-term costs of ART was an emergent theme. Many lacked a tangible sense of future steps and associated expenses, such as whom to contact, or what processes are involved in using stored gametes, noting “nothing really stuck to me mentally.” Exceptions to this trend were a 25-year-old lesbian woman and a 21-year-old who had a strained relationship with her biological parents. Both participants vocalized keen awareness of the total costs and future implications of FP/ART. The lesbian woman noted that even before cancer, she and her partner would joke:
…having kids as lesbians is something you have to plan out. Like, ‘theoretically if that were to happen, how the hell would that happen?’ … I want to have kids but, I don't know. We're not at a financial place where we could…Was I planning to ever get pregnant, though? I don't know. I do want kids. I do really want kids, I think. Is the kid gonna come out of my body? I really doubt it. I really, really, doubt it because I can't afford that.
The woman whose family-of-origin relations were strained remarked that her parents helped her with the cost of preservation, but she was paying for the storage fees herself and did not want to be “reliant on my family in the near future.” About her necessity to depend upon costly procedures to become pregnant, she said, “I don't really like that, but that is also my reality. I have eggs that are frozen, so if I need to use them, then I will use them, so whatever resources I need, hopefully I will have the financial resources to do any of that.” It is notable that female participants outnumbered male participants when discussing concerns about long-term costs.
Discussion
Our current study provides novel insights into financial concern for AYAs facing iatrogenic infertility and considering FP. Key findings indicate that multiple and interrelated financial considerations factor into AYA experiences and decision making, including ascertaining insurance coverage, presence of parental/guardian support, access to financial aid, negotiating potential risks, and consideration of long-ranging costs. Some participants indicated that no financial support existed for their circumstance and regrettably forewent FP. This study has implications for oncology research, clinical practice, and health care policy
The finding that AYAs relied heavily upon parents/guardians for out-of-pocket and insurance coverage support has bearings for population-level data analysis. AYAs may have very different financial resources through their parents. It is possible that large-scale databases may misrepresent AYAs in big analyses that use generic demographic markers such as socioeconomic status. Moving forward, measurement tools that evaluate AYAs' total financial support network, in addition to patient-level socioeconomic status, may improve research. In addition, validated scales on reproductive concerns are advised to incorporate measures of financial concern.
The finding that some participants sought financial aid when guided by providers—primarily nurses—to do so points to the instrumental role that a trained oncofertility workforce may play.20,45–49 The American Society for Clinical Oncology advises providers to make patients aware of available financial counseling services. 50 Cultivating a workforce of fertility nurse specialists who are specifically trained to address the concurrence of FP and short- and long-term financial toxicity is endorsed.20,45,51
The finding that certain financial concerns were more prevalent for different sexes (i.e., negotiating risk was more prevalent for male participants, long-term cost for female participants) builds upon data that have identified differential experiences of FP across the sexes.52–55 Further studies are needed to develop personalized solutions for differential financial concerns based upon diverse sex, sexual orientation, and gender identity, as well as other patient characteristics such as treatment protocol, age, presence of parental support, partnership status, and goals for future family. Furthermore, implementing tailored psychosocial interventions across the continuum (including well into survivorship) to directly address negative feelings associated with the costs of FP, such as guilt or shame, 22 is suggested as a future direction.
The reported lack of preparation to address long-ranging costs may be apprehended at the level of health care policy. At present, only twelve states have mandated insurance laws covering pretreatment FP for cancer patients; financial aid for post-treatment family building is largely nonexistent.2,29,56 Legislation to mandate insurance companies to cover pre- and post-treatment FP/ART costs, and/or adoption costs, would relieve AYAs of potential oncofertility-related financial burden. Federal grants afforded to nonprofit organizations that assist with FP costs would benefit AYAs by increasing coverage to include post-treatment financial aid.24,26,57 Policies to improve access to FP/ART coverage and financial aid advance equitable oncofertility practice for a diverse population of AYAs.58–60
In terms of strengths, this study explored financial concern for an underrepresented group within a vulnerable population (i.e., younger adolescents within AYAs). However, there is still much to learn about how AYAs living under different social conditions may experience FP-associated financial burdens, as earlier studies suggest that being female, unmarried, and nonwhite are associated with greater cancer-related economic burden.61,62 In particular, the experiences of unmarried AYAs older than age 26 who do not have insurance coverage through parents or spouses warrant further investigation. 63 Although parental support loomed large in the data, this study did not interview parents/guardians. Future investigations into financial concern for parents are needed. In addition, this study was conducted before the U.S. Supreme Court overturned the constitutional right to medical abortion (Dobbs v. Jackson Women's Health Organization 64 ). Future studies may consider concerns related to restricted abortion access where relevant, in as much as oncofertility is a function of reproductive justice.
Financial consequences of oncofertility are a major issue for AYA cancer patients and survivors. This exploratory study of AYAs facing iatrogenic infertility illuminates the multidimensional financial concerns about affording short- and long-term FP options.
Footnotes
Acknowledgments
The authors thank the anonymous reviewers for their supportive feedback. The authors also thank Dr. Christopher R. Friese, Dr. Daphne C. Watkins, Dr. Catherine Benedict, Dr. Bridgette Thom, Dr. Jessica R. Gorman, Dr. Lauren Ghazal, and Jackie Pilcowitz J.D. for sharing their insights in the process of writing this article. The authors thank Lisa Kelley, Anca Tilea, Kenneth Piehl, Julie Tumbarello, Dr. Erin Peregrine Antalis and the Master of Social Work research assistants for their contributions to the study. The authors credit Dr. Charles (Nate) Nessle and Dr. Jessica C. Francis for creatively brainstorming the title. The authors thank our study participants for sharing their experiences to advance health care for adolescent and young adult cancer patients and survivors.
Authors' Contribution
N.J.L.: Project Administration, investigation, data curation, formal analysis, writing—Original Draft, visualization; C.Y.T.: software, formal analysis, writing—review and editing; D.S.: investigation, data curation, formal analysis; N.T.I.: conceptualization, methodology, investigation, writing—review and editing, funding acquisition; A.Z.: conceptualization, methodology, investigation, writing—review and editing, funding acquisition; E.E.: conceptualization, methodology, resources, writing—review and editing, funding acquisition; L.A.H.: conceptualization, methodology, resources, writing—review and editing, funding acquisition. M.B.M.: conceptualization, methodology, resources, writing—review and editing, supervision, funding acquisition.
E.B.W.: conceptualization, methodology, resources, writing—review and editing, supervision, funding acquisition. R.C.: conceptualization, methodology, resources, writing—review and editing, supervision, funding acquisition. M.R.H.: supervision, writing—original draft. BZ: conceptualization, methodology, validation, resources, writing—review and editing, supervision, project administration, funding acquisition.
Funding Information
B.Z., R.C., M.B.M., E.B.W., L.A.H., E.E., A.Z., N.I., C.Y.T., D.S., and N.J.L. received funding from a Research Award (Innovation Grant) from the University of Michigan Rogel Cancer Center, under the National Cancer Institute Cancer Center Support Grant Award Number P30-CA-046592. N.J.L. received research support from the National Cancer Institute institutional training grant T32-CA-236621. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the National Cancer Institute. N.J.L. was also supported by a Research Assistantship and by the Bobbe and Jon Bridge Award for Engaged Scholarship from the University of Michigan School of Social Work. A.Z. and N.J.L. received research support from the University of Michigan Vivian A. and James L. Curtis School of Social Work Center for Health Equity Research and Training, Signature Programs Initiatives.
Author Disclosure Statement
The authors declare no conflict of interest.