
Abstract
Purpose:
This study aims to investigate whether oocyte stimulation outcomes in fertility preservation (FP) vary in patients with different stages of lymphoma.
Methods:
This is a retrospective cohort study conducted at Northwestern Memorial Hospital (NMH). Between 2006 and 2017, 89 patients were identified with a diagnosis of lymphoma who contacted the FP navigator at NMH. Anti-müllerian hormone (AMH) levels and FP ovarian stimulation outcomes were collected for analysis. The data were analyzed using chi-squared and analysis of variance tests. A regression analysis was also done to adjust for potential confounding variables.
Results:
Of the 89 patients who contacted the FP navigator, there were 12 patients (13.5%) with stage 1 lymphoma, 43 patients (48.3%) with stage 2, 13 patients (14.6%) with stage 3, 13 patients (14.6%) with stage 4, and 8 patients (9.0%) where staging information was not available. Forty-five of the patients proceeded with ovarian stimulation before initiating cancer treatment. Patients who underwent ovarian stimulation had a mean AMH level of 2.62 and median peak estradiol levels of 1772.0 pg/mL. Median oocytes retrieved was 16.77, mature oocytes were 11.00 and median oocytes frozen after completing FP was 8.00. These measures were also stratified by stage of lymphoma.
Conclusion:
We found no significant difference in number of retrieved, mature or vitrified oocytes between different cancer stages. There was also no difference in AMH levels in the different cancer stage groups. This suggests that even in higher stages of lymphoma, many patients respond to ovarian stimulation techniques and have a successful stimulation cycle.
Introduction
In 2019,
And for NHL, the most common chemotherapy regimen in the United States is cyclophosphamide, doxorubicin hydrochloride (hydroxydaunorubicin), vincristine sulfate (Oncovin), and prednisone (CHOP) or rituximab, CHOP (R-CHOP), which includes an alkylating agent, corticosteroid, and an anthracycline, which is often combined with an immunotherapy drug such as rituximab. 3 In refractory cases of lymphoma, stem cell transplant with high-dose chemotherapy may be indicated. 3 Because of both the gonadotoxicity associated with chemotherapy and radiotherapy and the improvement of cancer treatments and survival, fertility preservation (FP) has become an important factor in improving the quality of life for women of reproductive age who are diagnosed with cancer.
The ovaries are very sensitive to both cytotoxic drugs and ionizing radiation and, therefore, chemotherapy and radiotherapy can induce premature ovarian insufficiency or decreased ovarian reserve. These conditions may manifest as oligomenorrhea or amenorrhea in many circumstances. 4 Based on the American Society of Clinical Oncology recommendations, the risk of permanent amenorrhea in women treated with modern chemotherapy and radiotherapy for lymphoma are as follows: hematopoietic stem cell transplantation with cyclophosphamide or total body irradiation—high risk (>80%), BEACOPP—intermediate risk (20%–80%), ABVD—lower risk (<20%), and CHOP 4–6 cycles—lower risk (<20%). 5
Because of the potential risk of premature ovarian failure, recent research has shown that fertility after cancer treatment is a major concern for women with a recent cancer diagnosis and adequate information regarding FP should be a mainstay of all cancer care programs. 6 The common prevalence of NHL and HL in women of childbearing age is why discussion of FP is especially important in this group of patients.1,7
There are several FP strategies for women diagnosed with cancer, including controlled ovarian hyperstimulation (COH) with oocyte harvest for oocyte or embryo cryopreservation, ovarian tissue cryopreservation (OTC), and gonadotropin-releasing hormone (GnRH) analog treatment before chemotherapy. COH, which involves ovarian stimulation with injection medications, followed by an oocyte retrieval for oocyte or embryo cryopreservation, is an established FP method for postpubertal women who can delay the initiation of cancer treatment by ∼2 weeks. 8 In the past, ovarian stimulation was always started at the beginning of a menstrual cycle.
However, advancements in random start (RS) protocols for COH have allowed for quick initiation of COH cycles, which can shorten the delay of cancer treatment. Anti-müllerian hormone (AMH) levels are typically evaluated before initiating COH as a measure to estimate ovarian reserve; higher AMH levels indicating greater ovarian reserve. Peak estradiol levels (E2) are another measure of COH response during a stimulation cycle, with increased levels indicating a better response. Oocyte and embryo cryopreservation are both well-studied methods and choosing between the two may be based on a patient's personal preference. Because embryo cryopreservation requires a male partner or the use of donor sperm, it exposes women to potential ethical and legal implications in the instance of an unused embryo. 8
Oocyte cryopreservation, however, allows women the opportunity to make a decision regarding the fertilization of the oocyte in the future. OTC is indicated in prepubertal girls and women who cannot or do not wish to delay the initiation of cancer treatment. 8 Although data regarding the efficacy, safety, and outcomes of this method are limited, the American Society of Reproductive Medicine has deemed this technique nonexperimental and recommended its use in the prepubertal individuals discussed earlier. 9 GnRH treatment is considered a treatment for ovarian protection before chemotherapy in an attempt to reduce damage to ovarian reserve, but there is insufficient evidence regarding its effectiveness in terms of FP and, therefore, is considered experimental. 10 There is also the potential to combine strategies.
Investigators have studied FP COH outcomes in cancer patients versus healthy in vitro fertilization (IVF) patients, although it remains unclear how the cancer process itself may negatively affect FP outcomes. Quintero et al discussed the hypothesis that cancer patients may respond poorly to ovarian stimulation given that cancer is often a catabolic state that may cause an elevation of stress hormones. Their study, however, found no significant difference in the number of oocytes retrieved, number of fertilized oocytes, days of stimulation, or dose of gonadotropins between the cancer group and the healthy group. 11 Further studies by different investigators have also compared FP outcomes among patients with different cancer types.
Pavone et al found that, overall, patients with cancer had lower oocyte yields than age-matched infertile controls, suggesting that cancer itself may impact the ovary's ability to respond to gonadotropins. They also found that patients with hematologic malignancies had the longest stimulations, however, had overall similar oocytes retrieved. In addition, patients with breast or gynecologic cancers had a greater number of oocytes retrieved, suggesting the hormone sensitivity of tumors may play a role in ovarian stimulation outcomes. 12 Similarly, Alvarez and Ramanathan found that patients with gynecologic cancer had a reduced number of retrieved mature oocytes when compared with patients with breast or hematologic cancers.
They noted although that 10 patients in their group underwent hysterectomy with ovary conservation before FP, which may have affected ovarian response to stimulation. 13 Although it remains largely unclear why the findings differ among these studies, we believe that many different factors play a role in affecting FP outcomes in cancer patients. To look more specifically at these potential factors, we analyzed if the cancer stage at the time of FP affects COH outcomes in patients with lymphoma. We hypothesized that higher cancer stage negatively affects COH outcomes for FP patients who have not been exposed to chemotherapy or radiation. To investigate this, we performed a retrospective cohort study of female patients with lymphoma to determine if their stage of cancer affects the oocyte stimulation capacity for FP.
Materials and Methods
This is an Institutional Review Board-approved study. Subjects were identified from an FP patient log of women with a cancer diagnosis who contacted the FP patient navigator (PN) at Northwestern Memorial Hospital between January 2006 and December 2017. Only patients with lymphoma who chose to initiate a cycle for either oocyte or embryo cryopreservation were included. Since this article focuses on lymphoma, patients were excluded if they were diagnosed with any other type of malignancy. Other exclusion criteria for our study included age >45 years at the time of FP PN contact and chemotherapy within 5 years of beginning ovarian stimulation. Of note, there were no patients with a history of chemotherapy in our study.
For each patient, specific lymphoma diagnosis, cancer stage, other past cancer diagnoses, treatment history, dates of initial contact with FP PN, and dates of COH cycle initiation were collected. AMH levels and COH outcome data, including antral follicle count on ultrasound, total number of stimulation days, day of antagonist start, peak E2, oocyte yield at the time of egg retrieval, and the number of mature oocytes or zygotes cryopreserved, were also collected for analysis. These data were collected from medical records.
Controlled ovarian hyperstimulation
Our COH protocol has been documented in previous studies. 14 In brief, COH was started using recombinant follicle-stimulating hormone with or without urinary menotropins with dosage determined by age and ovarian reserve measurements. Over time, our practice has evolved to include more RS protocols, which allow patients to begin stimulation immediately if they wish to do so. Gonadotropins were initiated at any point in the menstrual cycle for RS, and on the 3rd day of menses for menstrual-cycle specific (CS). Medication response was monitored with regular ultrasounds and E2 measurements and subsequent medication dosage was adjusted accordingly.
For a CS protocol, once the leading follicle grew to at least 12 mm in diameter or E2 reached 300 pg/mL, the patient began a daily injection of GnRH antagonist to prevent premature ovulation. For an RS protocol, the GnRH antagonist was started once the lead follicle grew to at least 12 mm. Per our institutional IVF protocol for all patients, when at least two follicles measured 16 mm in diameter, final follicular maturation was triggered by an injection of human chorionic gonadotropin, GnRH agonist, or a combination of both depending on peak E2. Oocyte retrieval was then performed 36 hours later. Cryopreservation of oocytes was performed at our clinic using slow cooling until 2008, when vitrification became the standard protocol. 15 All zygotes were cryopreserved using slow freeze.
Statistical analysis
The data were analyzed using chi-squared and analysis of variance tests followed by post hoc Tukey test. A limited regression analysis was also done to adjust for potential confounding variables. p-Values <0.05 was considered statistically significant. All statistics were done using SPSS software. The institutional review board approved this study.
Results
FP patient cohort
A total of 89 lymphoma patients initially contacted the FP PN for an FP consult and were included in the analysis. Their demographic data are summarized in Table 1. Of the 89 patients included 45 (50.5%) proceeded with ovarian stimulation for FP before initiating cancer treatment (Table 2). The median age at the time of contact with the PN was 28.3 years (range 18.0–43.7 years) for the entire cohort and 27.7 years (range 20.8–38.3 years) for patients that initiated a stimulation cycle (Table 1). Body mass index (BMI) was included as one of the variables investigated given the fact that it can influence ovarian response to stimulation. The average BMI was 24.93 (15.50–43.52) for the entire cohort and 25.23 (17.71–43.27) for patients who initiated a stimulation cycle. In terms of lymphoma staging, there were 12 patients (13.5%) with stage 1, 43 patients (48.3%) with stage 2, 13 patients (14.6%) with stage 3, 13 patients (14.6%) with stage 4, and 8 patients (9.0%) where staging information was not available.
Demographic Information and Lymphoma Staging for Patients Who Contacted Fertility Preservation Patient Navigator
BMI, body mass index; FP, fertility preservation; PN, patient navigator.
Demographic Information and Lymphoma Staging for Patients Who Initiated Stimulation Cycle
Decision to pursue FP
Of the 44 cancer patients (49.4%) who did not undergo FP, the primary reason cited in the medical record was insufficient time to complete an ovarian stimulation cycle before initiation of cancer treatment (17 patients, 38.6%). Of the remaining patients, 7 (15.9%) were prescribed cancer treatment that was not gonadotoxic or posed no threat to fertility, 6 (13.6%) were not interested in future childbearing, 5 (11.4%) did not follow up with the PN, 2 (4.5%) were not interested in FP, and 1 (2.3%) underwent Lupron Depot for FP. There was no reason documented for declining FP in 6 patients (13.6%). Interestingly, no patients cited disease burden or performance status as a factor in choosing to forgo FP.
Ovarian stimulation
Of the 45 patients who elected FP, there were 44 patients analyzed with complete stimulation information; one of the 45 patients who elected FP started ovarian stimulation but had their cycle canceled before egg retrieval due to poor response. The prestimulation mean AMH level for patients who underwent a stimulation cycle was 2.62 (range 0.18–9.56). Median peak E2 was 1772.0 pg/mL (range 171.8–7443.0 pg/mL). The median total number of oocytes retrieved was 16.77 (range 3–56). The median number of mature oocytes retrieved was 11.00 (range 0–46). The median number of oocytes frozen after completing FP was 8.00 (range 0–56) (Table 3).
Ovarian Stimulation
Median values reported.
AMH, anti-müllerian hormone; COH, controlled ovarian hyperstimulation; E2, estradiol levels.
COH outcomes: assessing the impact of cancer stage
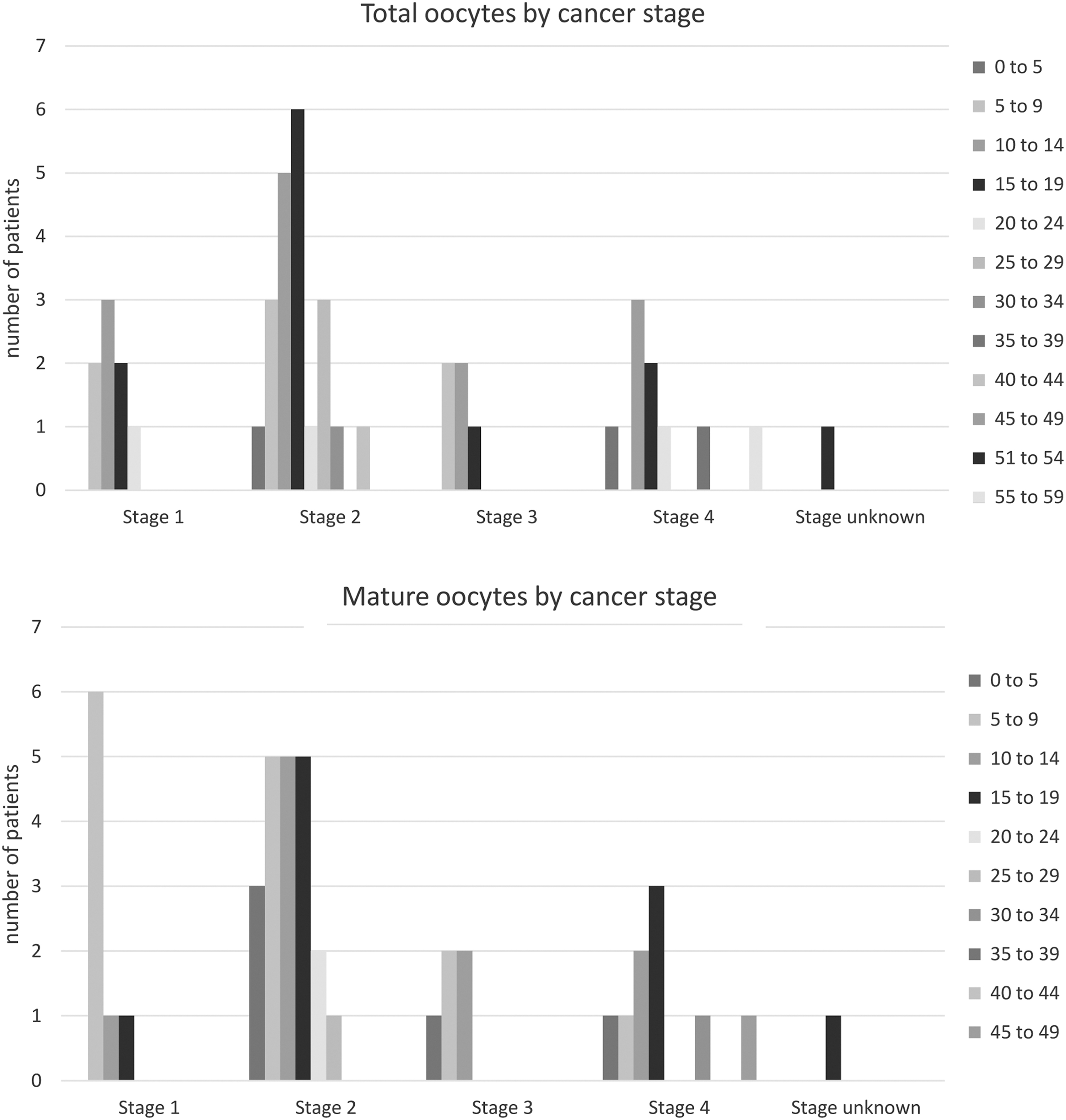
For this study, we explored how a particular stage of lymphoma impacted COH characteristics. These data are summarized in Table 4. We found no significant difference in AMH level based on the cancer stage. We found no difference in the number of retrieved, mature or vitrified oocytes. There was also no difference between cancer stages of any of the other COH characteristics (Table 5). The total number and mature oocytes by cancer stage are represented in Table 4 and Figure 1. After conducting a regression analysis of age and cancer stage, there was no difference in AMH levels.
Analysis of variance stats.
Ovarian Stimulation Measures: Cancer Stage
There were no statistically significant differences noted.
Analysis of Variance Analysis of Age, Body Mass Index, and Anti-Müllerian Hormone by Cancer Stage
p < 0.05; post hoc Tukey's test showed that there are BMI differences between stage 1 and 3, stage 2 and 3, and between stages 3.
COH outcomes: assessing the impact of type of lymphoma (HL vs. NHL)
For this study, we explored how the type of lymphoma, HL versus NHL, impacted COH characteristics. These data are summarized in Table 6. We found no significant difference in AMH level based on the cancer stage. We found no significant differences in the number of retrieved, mature or vitrified oocytes. There was also no difference between the cancer type, HL versus NHL, of any of the other COH characteristics.
Ovarian Stimulation Measures: Hodgkin's Versus Non-Hodgkin's Lymphoma
No significant differences noted.
Discussion
This is one of the only studies evaluating FP outcomes in patients with different stages of lymphoma. We found no significant difference in the number of retrieved, mature or vitrified oocytes between different cancer stages. There was also no difference in AMH levels in the different cancer stage groups. This suggests that even with advanced lymphoma, ovarian stimulation for freezing oocytes or embryos could still be a viable option. There were also no differences in stimulation parameters and COH outcomes when examining HL versus NHL.
There have been a few other studies that have evaluated the effects of cancer stage and grade on FP outcomes. Volodarsky-Perel et al investigated 10 different cancer types and the effects of stage and grade on FP outcomes with mature and vitrified oocytes retrieved as the primary outcomes. They divided patients into low-stage (I and II) and high-stage (III and IV) groups and low-grade (G1 and G2) and high-grade (G3–G4) malignancies. They found a similar number of mature and vitrified oocytes retrieved between the low- and high-stage groups, which supports our findings. They did find fewer vitrified embryos in the high-grade group, however. 16 Volodarsky-Perel et al did another study specifically looking at cancer stage and grade in breast cancer patients.
This followed the same method as the previous article of dividing patients into low and high stage and grade groups. They found no difference in oocyte retrieval between low- and high-stage groups but did find that high-grade breast cancer negatively affected oocyte numbers. 17 Another study from Cioffi et al specifically evaluated the effect of stage and grade in patients with breast cancer. This study divided the patient into low-stage (I) and high-stage (II and III) and low-grade (G1–2) and high-grade (G3) groups. They found that high-stage and high-grade disease was not associated with worse oocyte retrieval outcomes. 18 Overall, these studies were consistent with our findings that the cancer stage does not have a significant effect on FP outcomes.
There are reports that cancer itself does negatively affect FP outcomes. Domingo et al conducted a retrospective cohort study that compared FP outcomes in cancer patients before treatment and a control group. Primary outcomes included days of stimulation, total dose of gonadotropins, estrogen levels, and number of oocytes retrieved and vitrified. The study found that patients with cancer had a weaker response to ovarian stimulation than the control group. 19 This suggests that cancer itself does affect FP outcomes, which does not directly refute our results.
However, this was the basis of our hypothesis that increased cancer stage would negatively affect FP outcomes. In addition, our group similarly found that different types of cancer impacted FP outcomes. The article included patients with breast, gynecologic, lymphoma/leukemia, and other cancers and compared them with IVF controls and found that IVF controls had higher peak E2, number of oocytes obtained, and fertilization rates when compared with the cancer patients. Moreover, patients with breast and gynecologic cancer were found to have a greater number of oocytes retrieved than other cancer types. 12
The strengths of this article include the novelty of the study question. FP in the form of oocyte and embryo cryopreservation has been done for quite some time. Although there have been numerous studies looking at cancers and FP outcomes, the effects of cancer staging itself have been understudied. Because lymphoma is common in women of childbearing age, this information could help guide more personalized discussions with patients about FP around the time of diagnosis. Weaknesses include the overall small number of patients and the retrospective nature of the study. Given that our study population spanned an 11-year period, the evolution of lymphoma treatment and FP methods posed a challenge. For example, there were numerous patients included in this study who were set to undergo BEACOPP chemotherapy treatment, which is noted to be more gonadotoxic but not as commonly used anymore.
This may affect the generalizability of FP decision-making to patients who are presently being diagnosed with lymphoma. Advancements in FP methods may also have led to better FP outcomes in patients who underwent ovarian stimulation more recently. In addition, there were patients whose data, such as AMH levels, were not accessible due to the outdated electronic medical record or that some of the early patients in our study were seen before the routine use of AMH as a marker of ovarian reserve. In addition, since not all of the patients received their cancer care at our institution, it was not clear in all cases where the lymphoma was present, and if the pelvis or abdomen was involved.
In the future, we will continue to investigate the effect of cancer stage on ovarian stimulation outcomes in larger patient cohorts and other types of cancer that are common in reproductive-age women. The results of this study and others like it have implications for driving patient care. We have shown that even in higher stages of cancer, many patients respond to ovarian stimulation techniques and have a good chance of a successful stimulation cycle. With improving cancer treatments, we should be discussing FP with all reproductive-age patients.
Footnotes
Authors' Contributions
All authors contributed to the conceptualization and design of the article. The methods and data analysis were conducted by S.S. and A.K.L., respectively. The article was drafted by V.K. and M.E.P. All authors contributed equally to the review and editing of the final article.
Ethics Approval
Institutional Review Board (IRB) approval was obtained.
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
No funding was received for conducting this study.