
Abstract
Purpose:
Reproductive health and sexual function are important to survivors of Adolescent and Young adult (AYA) cancers. We evaluated the prevalence of sexual dysfunction and factors associated with dysfunction using the Patient-Reported Outcomes Measurement Information System (PROMIS) sexual function (SexFS) measure in AYAs (15–39 years old at diagnosis) enrolled in a cancer survivorship cohort.
Materials and Methods:
Using a cross-sectional survey of a tertiary medical center-based cancer survivorship cohort, we determined the mean PROMIS SexFS v1.0 T-scores and prevalence of scores that were indicative of dysfunction (>1/2 standard deviation [SD] below reference population mean). Multivariable generalized linear regression was performed to identify factors associated with lower scores.
Results:
We identified 284 AYA cancer survivors, most of whom were women (70%). The mean age at survey was 36.0 years (SD = 7.9). Overall, 31% of females and 19% of men had clinically significantly lower scores than the general U.S. population in the domain of interest, and 13% of women and 6% of men had abnormal scores for satisfaction. Twenty-six percent of male AYAs reported erectile dysfunction. The rate of sexual inactivity in the last 30 days was 27%. Low levels of physical activity were associated with lower PROMIS scores for interest in sexual activity in both men and women, and for global satisfaction with sex life in women only.
Conclusions:
Our results suggest that low interest in sexual activity is common among survivors of AYA cancers. Low levels of physical activity may be associated with lower levels of interest in and satisfaction with sexual activity in this population.
Introduction
In the United States, more than 89,000 individuals are diagnosed with cancer during adolescence and young adulthood (AYA, ages 15–39) each year. 1 Because 5-year survival rates are high and increasing over time, issues surrounding survivorship are important to investigate.2–4 Reproductive health, including fertility and sexual function, is critically important to AYA survivors, particularly given that the adolescent and young adult period is a time of sexual development and maturation.5,6
Sexual health is defined by the WHO as “a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity.” 7 Sexual dysfunction is a component of overall sexual health, and encompasses multiple disorders characterized by a clinically significant disturbance in an individual's ability to respond sexually or to experience sexual pleasure. 8 Among individuals with cancer, this dysfunction is likely multifactorial, secondary to changes in body image, side effects of surgical treatment, gonadotoxicity of therapy, intentional gonadal suppression for maintenance therapy, or psychosocial stressors.9–11 Multiple analyses have found associations between sexual dysfunction after cancer and poor health-related quality of life. 5 Most data regarding sexual function after cancer treatment comes from women with breast cancer 11,12 and survivors of childhood cancer.6,10,13
Sexual dysfunction among survivors of AYA cancer has been previously reported.4,14–16 However, prior studies have used a variety of assessment tools, often with only a single item to assess sexual function. They have also lacked assessment of overall satisfaction with sexual function and evaluation of specific physiologic components that may contribute to dysfunction. The National Institutes of Health's Patient-Reported Outcomes Measurement Information System (PROMIS) tools are publicly available instruments designed to assess a variety of health domains. The PROMIS Sexual Function brief profile (PROMIS SexFS v1.0) is a validated scale that includes gender-specific domains and overall satisfaction assessment. 17 t has been validated in diverse populations including younger adults and adults with a variety of chronic diseases, making it a useful tool for patient-centered research.17–20 To our knowledge, there has not been a report of sexual function in AYA cancer survivors assessed with the PROMIS SexFS.
We aimed to use the PROMIS SexFS measures to describe the prevalence of sexual dysfunction in survivors of AYA cancers.
Materials and Methods
We conducted a cross-sectional analysis of data from a large tertiary medical center-based observational cohort. The University of North Carolina (UNC) Cancer Survivorship Cohort is a registry of cancer patients that integrates clinical and epidemiological data and biologic specimens. Participants were identified and recruited through UNC Healthcare outpatient oncology clinics between 2010 and 2016 with the following eligibility criteria: age ≥18 years at enrollment; North Carolina mailing address; and English or Spanish language proficiency. Those unable to provide informed consent or participate in questionnaires were excluded. In total, 5626 individuals with cancer were successfully enrolled in the cohort. For this analysis, eligibility was further restricted to participants who were diagnosed with cancer between ages 15 and 39 years and completed the baseline survey. The original study and this analysis were approved by the UNC Institutional Review Board.
Participants completed a baseline survey after enrollment that was administered by trained staff using computer-assisted telephone-based interviews. This survey included assessment of patient demographics, health history, reproductive history, health-related quality of life (PROMIS global health short form), 21 physical activity (World Health Organization Global Physical Activity Questionnaire [GPAQ]), 22 and sexual function (PROMIS sexual function and satisfaction [SexFS]). 17
The PROMIS v1.0 Sexual Function and Satisfaction Brief Profile is a 10-item scale for women and an 8-item scale for men that measures six subdomains of sexual function and satisfaction: interest in sexual activity, vaginal discomfort (women), lubrication (women), erectile function (men), orgasm, and global satisfaction with sex life. Additional information can be obtained at the PROMIS website (www.nihpromis.org). Symptom severity over the past 30 days is graded on a 5-point Likert-type scale.
Each domain of the PROMIS SexFS is scored using T-scores, which are standardized to the U.S. general population and have a mean of 50 and a standard deviation (SD) of 10. A clinically meaningful cutoff for this scale is defined as one-half SD (five points) below the population mean. In the case of vaginal discomfort only, increased discomfort leads to a higher T-score; therefore, a score of ≥55 is clinically significant. Sexual inactivity was determined by response of “no sexual activity” on the item “In the past 30 days, when you have had sexual activity, how satisfying has it been?”
Physical activity was assessed with the GPAQ. 22 Activity level was dichotomized as either meeting WHO physical activity recommendations (≥600 MET min/week) or not (<600 MET min/week).
The PROMIS questionnaire v1.0 Global is a 10-item scale that measures the quality-of-life domains including physical function, fatigue, pain, emotional distress, and social health. It generates T-scores for global physical health and global mental health that are standardized to the U.S. general population and have a mean of 50 and an SD of 10. Higher scores correspond to higher levels of health-related quality of life. 21
The clinical data abstracted from the medical record at time of enrollment were combined with the Health Registry/Cancer Survivorship Cohort demographics. Patient age at diagnosis and survey, marital status, cancer stage, grade, and initial course of treatment were obtained and used for the analysis.
Statistical analysis
T-scores calculated among AYA survivors within each domain of the PROMIS Sex FS were compared with standardized population means. To evaluate associations between patient characteristics and PROMIS SexFS scores among AYA survivors, we used generalized linear regression to estimate adjusted means and 95% confidence intervals. Multivariable models adjusted a priori for age at time of survey and time from diagnosis to survey. Demographic factors included marital status, age at diagnosis, and age at baseline. Medical characteristics included self-reported physical activity using the GPAQ tool and self-rated physical function and mental health (PROMIS physical and mental). Disease characteristics included cancer type, stage, time since diagnosis, and treatment modalities. Data were analyzed with SAS 9.4 (Cary, NC, USA).
Results
There were 295 individuals diagnosed with cancer between the ages of 15 and 39 enrolled in the Cancer Survivorship Cohort who completed the baseline survey. Eleven were excluded for missing dates of diagnosis or survey or completing the survey before cancer diagnosis, leaving n = 284 as the final study population. Of note, there were only three participants in the final sample who were diagnosed as adolescents (age 15–19). The majority of participants were women (70%), 30–39 years old at time of cancer diagnosis (72%) and married or living with a partner (65%).
The mean age at survey was 36.0 years (SD = 7.9) and a majority (52%) were <1 year from time of cancer diagnosis. Mean age at diagnosis was 32.6 years (SD = 5.2) and the most common diagnoses were breast (42%), gynecologic (cervical, vaginal, ovarian, endometrial; 27%), and testicular (36%). The majority of participants had localized disease at diagnosis (48%) and had surgery as a part of their treatment (77%). Approximately half received any chemotherapy (47%) and a smaller portion received any radiation therapy (37%) (Table 1). More than half had T-scores <50 for PROMIS mental (51%) and physical (58%) overall health and met physical activity recommendations (53%).
Descriptive Characteristics of 284 Adolescent and Young Adult Cancer Survivors in the University of North Carolina Cancer Survivorship Cohort
Defined as cervical, endometrial, ovarian, vaginal.
Physical activity level determined by GPAQ scale.
GPAQ, Global Physical Activity Questionnaire; PROMIS, Patient-Reported Outcomes Measurement Information System.
Overall, 27% reported no sexual activity in the past 30 days and therefore generated PROMIS SexFS scores only in the domain of interest. Individuals who were sexually active were more likely to be married or living with a partner than those who were not sexually active (76% vs. 45%, p < 0.001). Compared with those who were not sexually active, those who were had a higher frequency of PROMIS mental (54% vs. 35%, p = 0.003) and physical T-scores (48% vs. 26%, p = 0.001) above the population mean and were more likely to report moderate or high levels of physical activity (61% vs. 45%, p = 0.008).
The distribution of responses to the sexual function questions by sex are included in Supplementary Table S1. Overall, a higher proportion of female survivors (20%) reported no interest in sexual activity compared with male survivors (13%). Among women, 17% of respondents reported intercourse was very uncomfortable or uncomfortable and 16% reported having to stop intercourse because of discomfort. Among men, 25% reported difficulty getting an erection and 22% reported difficulty keeping an erection.
Figure 1 provides the proportion with PROMIS SexFS scores that were 5 points (1/2 SD) or more from the standardized population mean T-score of 50, indicating clinically significant worse function compared with the general population. In all domains except for vaginal discomfort this would be scores ≤45. Scores ≥55 in the domain of vaginal discomfort would be clinically significantly worse than the population mean. Overall, 27% and 11% of respondents had interest and satisfaction scores, respectively, that were clinically significantly lower than the population mean.
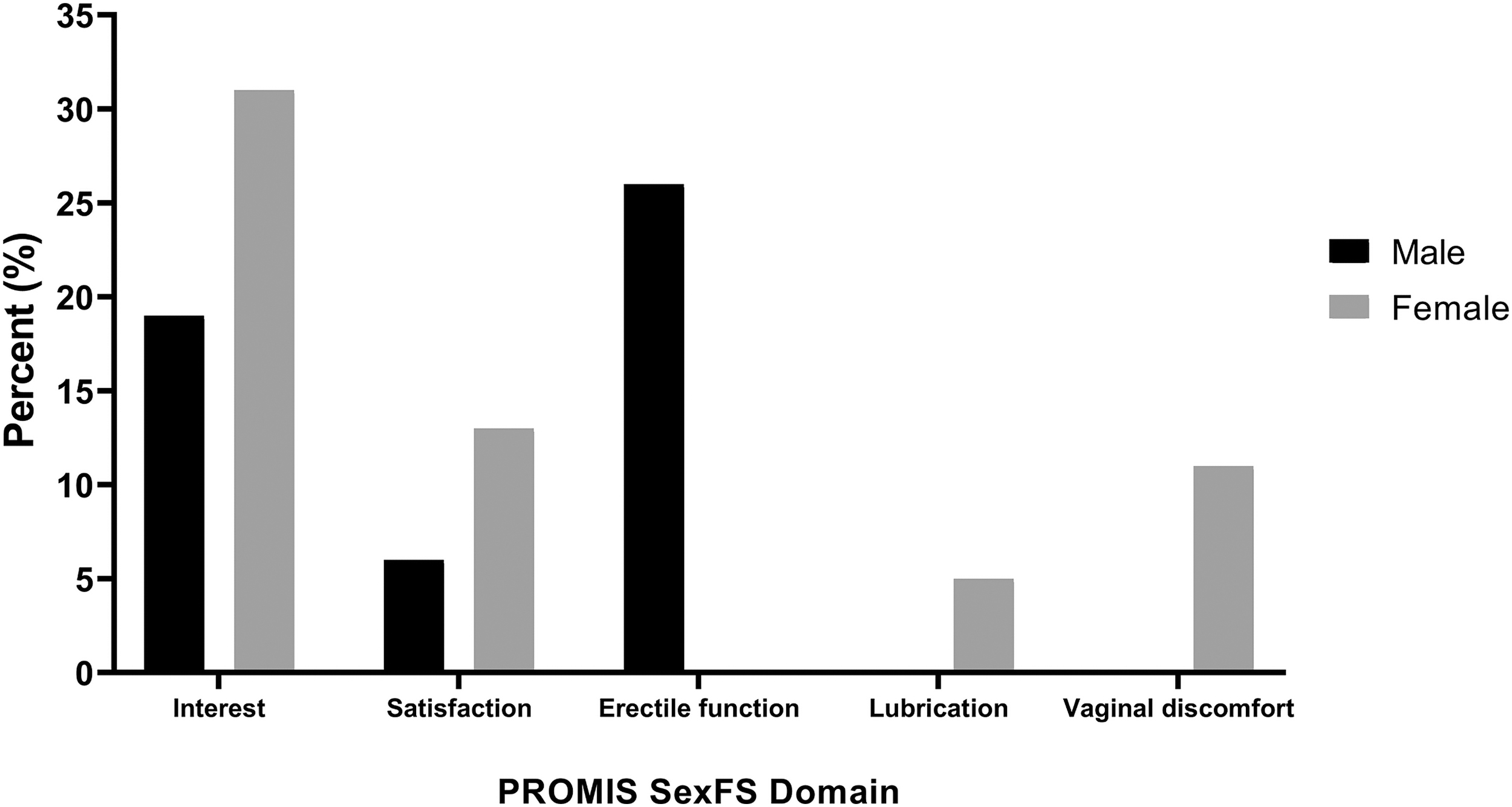
Proportion of male and female adolescent and young adult survivors in UNC Cancer Survivorship Cohort with T-scores at least one-half of a standard deviation below (or above for vaginal discomfort only) the standard U.S. population mean (indicating worse sexual function) in five domains of sexual function. UNC, University of North Carolina.
Among men, 27% reported erectile dysfunction that was clinically significantly worse than population mean. Among women 5% and 11% reported clinically significant issues with lubrication and vaginal discomfort, respectively. Mean PROMIS SexFS T-scores are given in Supplementary Table S2. Among male AYA survivors, the mean score for satisfaction was 58.8, clinically significantly higher satisfaction than the general U.S. population. Female AYAs had mean scores indicating clinically significantly less vaginal discomfort, improved lubrication, and greater satisfaction than the general U.S. female population. Scores in the domains of interest and erectile function were within 5 points of the U.S. population mean of 50, similar to the general U.S. adult population.
Table 2 provides multivariable-adjusted Sex FS scores among women in our AYA survivor cohort according to sample characteristics. Women with gynecologic or breast cancer had lower mean T scores for lubrication, indicating worse lubrication, than women with other cancers (p < 0.01). For vaginal discomfort, women with gynecologic cancer had significantly higher scores (p < 0.01), indicating greater discomfort, than women with other cancers.
Adjusted Mean Patient-Reported Outcomes Measurement Information System Sexual Function T-Scores for Female Adolescent and Young Adult survivors in the University of North Carolina Cancer Survivorship Cohort
Adjusted for age at survey and time from diagnosis to survey.
Defined as cervical, endometrial, ovarian, vaginal.
Among women, receipt of chemotherapy was associated with significantly lower mean T-score in the domain of lubrication (55.65 vs. 59.17, p < 0.01). There was no difference in scores for other treatment types. Moderate to high levels of physical activity were associated with significantly higher PROMIS-SexFS scores for interest, satisfaction, and lubrication. Female AYAs with PROMIS global physical and mental health scores ≥50 had significantly higher scores in the interest and satisfaction domains as well, but not in the lubrication or vaginal discomfort domains. (Table 2)
Adjusted scores among male AYA survivors are given in Table 3. Those who were married had significantly higher scores in the domain of interest compared with those who were single, divorced, widowed, or separated. Receipt of radiation therapy was associated with a significantly lower score in the domain of erectile dysfunction (45.8 vs. 46.9, p = 0.02). Guideline-recommended physical activity was associated with statistically significantly higher mean scores for interest in sexual activity compared with not meeting guidelines (56.2 vs. 50.5, p = 0.008). Higher PROMIS physical health t-scores were also associated with higher interest scores, but there was not a significant difference in scores in any domain by PROMIS mental health score.
Adjusted Mean Patient-Reported Outcomes Measurement Information System Sexual Function and Satisfaction T-Scores for Male Adolescent and Young adult Survivors in the University of North Carolina Cancer Survivorship Cohort
Adjusted for age at survey, and time from diagnosis to survey.
Discussion
To our knowledge this is among the first reports of the PROMIS SexFS in a population of survivors of AYA cancers. Our study has several important findings. We found that mean scores among survivors of AYA cancers were similar to or better than U.S. general population means in most domains of sexual function. Interest in sexual activity was the domain of the PROMIS SexFS with the highest prevalence of dysfunction among survivors of AYA cancer, with 27% of survivors in our study having scores for interest that were clinically significantly lower than the general population mean. We also found that patient factors associated with lower scores in the PROMIS SexFS domains among survivors of AYA cancers included lower levels of physical activity and lower patient-reported mental and physical health.
Overall, our results suggest that sexual function among survivors of AYA cancer may be comparable with or better than the general population in most domains. Compared with the T-scores for age groups 18–29 and 30–44 years in a PROMIS SexFS validation study, 20 the scores in our population are similar to the scores they obtained for interest, and higher than the validation population in the domains of satisfaction and lubrication. In the domain of erectile function, our cohort mean score of 46.5 was significantly lower than the 18–29 and 30- to 44-year-old validation group means of 55.4 and 54.5, respectively. This suggests that sexual function among sexually active survivors of AYA cancer may be similar to a noncancer population in the domains of interest, satisfaction, vaginal discomfort, lubrication, and worse for erectile function.
The prevalence of sexual inactivity in the past 30 days among women in our cohort was 29%, similar to rates of 26%–32% reported in noncancer cohorts of this age,18,19 and to the 28% rate of inactivity reported by older female cancer survivors (mean age 52 years). 23 The prevalence of sexual inactivity reported by women in our population was 21%, which is somewhat higher than reports of 15% in the general U.S. male population.18,19 The reason for sexual inactivity would be important to assess in future studies as some individuals may choose to avoid sexual activity because of pain or other dysfunction, and we are unable to account for that in this study.
In a 2008 national sample of U.S. women, the rate of self-reported low desire among those aged 18–44 was 22%. 24 The rate of “no interest” or “a little bit of interest” in sex in our female AYA population was substantially higher (45%). Lower desire in female survivors of AYA cancer may be related to factors that are unmeasured in this study such as body image, interpersonal relationship dynamics, partner health factors and interest, and medical comorbidities.4,25–27 The prevalence of reduced interest among men in our cohort was 26%. Previous reports in the general population have also identified lower interest in sex among women compared with men. In a national sample of men and women aged 18–39, Laumann et al identified that lack of desire was reported by ∼32% of women and 14% of men.28,29 The primary factors associated with low desire were emotional problems or stress, and reduced sexual frequency. The higher prevalence of reduced interest among both men and women in our study compared with theirs may reflect greater emotional problems or stress in cancer survivors compared with the general population.
For both male and female AYAs, physical activity levels that met WHO guideline recommendations and higher scores on the PROMIS physical function measure were associated with significantly higher sexual interest scores. Physical activity was also associated with higher sexual satisfaction scores for women only. This is consistent with associations of physical quality of life and sexual function found in prior studies. 30 Our cross-sectional data cannot assess the temporality of these associations; however, interventions to promote physical activity for AYA cancer survivors have a wide range of potential benefits, and may enhance sexual function. 31
Cancer-related sexual dysfunction is thought to develop as a result of impaired physiologic function involved in the sexual response including hormone feedback, autonomic nervous system signaling to increase genital blood flow, vasculature in the pelvis and sensory nerves. 5 This may be secondary to chemotherapy resulting in ovarian failure and lack of estrogen, or to damage inflicted to brain centers by radiation therapy. In our study, chemotherapy was the only treatment type associated with significantly lower sexual function scores and it was limited to the domain of lubrication in women. Radiation therapy for men was associated with statistically significantly worse scores for erectile dysfunction; however, this was a difference of only 1.11 in the mean T score, which may not be clinically meaningful.
Several limitations of the analysis should be considered. Cross-sectional data does not allow for determination of causal or temporal relationships. Only individuals who are sexually active generate scores in the PROMIS SexFS domains of satisfaction, erectile dysfunction, and vaginal discomfort; therefore, individuals who are not sexually active owing to pain or other dysfunction are not captured by this measure, potentially resulting in an underestimate of the prevalence of sexual dysfunction. The domain of sexual interest was completed by all individuals regardless of recent sexual activity. Of note, the SexFS brief profile v2.0 now includes a question regarding reason for not engaging in sexual activity in the past 30 days, but this was introduced after our survey. In addition, all the individuals completed the survey after diagnosis and at different times during or after treatment, and there was no assessment of sexual function before diagnosis with which to compare.
The PROMIS SexFS v1.0 did not include assessment of other types of sexual activity include masturbation or oral sex, which could provide further insight into sexual function of cancer survivors. All participants received care at a single institution and therefore may not be representative of the general AYA survivor population. In addition, our cohort included only three individuals diagnosed with cancer younger than the age of 19 years. Another limitation of the study is that the development of the PROMIS Sex FS measure was performed among older cancer survivors with a mean age of 58.5, 17 and validation studies included few young adults. Therefore the mean T-scores are normalized to a population older than the AYA survivors in our study. This may account for improved scores in some domains in our cohort compared with overall population means. Comparisons within our cohort are unaffected by this.
Conclusions
In our sample, sexual function of AYA survivors as assessed by the PROMIS SexFS was similar to the general U.S. population in the domains of interest, satisfaction, vaginal lubrication, and vaginal discomfort, but worse for erectile function. Overall, 27% of AYA cancer survivors reported significantly lower interest in sexual activity than the U.S. population mean. Higher levels of physical activity were associated with higher scores for satisfaction from and interest in sexual activity. These results may provide a promising avenue for future prospective research to identify potential interventions to improve outcomes. With increasing attention to the unique survivorship needs of AYA cancer patients, we encourage sexual function to be included in the collection of longitudinal outcomes.
Footnotes
Acknowledgments
The authors thank the UNC Health Registry/Cancer Survivorship Cohort (HR/CSC) participants for their important contributions. The HR/CSC is funded in part by the UNC Lineberger Comprehensive Cancer Center's University Cancer Research Fund. This project was reviewed and approved by the Human Research Protections Program (IRB No.: 09-0605) at the University of North Carolina at Chapel Hill.
Authors' Contributions
All authors contributed to the study conception, design, and interpretation. Material preparation, data collection, and analysis were performed by V.W.Z., C.A., J.B., and H.N. The first draft of the article was written by V.W.F. and all authors commented on previous versions of the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The HR/CSC is funded in part by the UNC Lineberger Comprehensive Cancer Center's University Cancer Research Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.