
Abstract
Young adults (YAs), aged 18–39 years, with acute myeloid leukemia (AML) navigate life disruptions amid an unpredictable illness trajectory. We conducted a secondary analysis of patient-reported outcomes for hospitalized YAs with high-risk AML receiving intensive chemotherapy, collected during a multisite randomized clinical trial. Of the 160 patients, 14 (8.8%) were YAs. At week 2 of hospitalization, YAs demonstrated significant worse quality of life (β = −18.27; p = 0.036), higher anxiety (β = 2.72; p = 0.048), and higher post-traumatic stress disorder (PTSD; β = 10.34; p = 0.007) compared with older adults. Our analysis demonstrated a longitudinal presence of anxiety and PTSD, suggesting persistent unmet psychological needs for YAs with AML.
Introduction
Young adults (YAs),
Patients with acute myeloid leukemia (AML), in particular, face an abrupt onset of life-threatening illness, and must navigate several treatment intensity choices and often prolonged and/or frequent hospitalizations.6,7 While AML is typically diagnosed in older adults, with a median age at diagnosis of 68 years, 8 YAs have a higher chance of being cured, and as such are treated more aggressively. Intensive chemotherapy for many young, otherwise healthy AML patients consists of a combination of cytarabine and anthracycline, commonly referred to as the “7 + 3” regimen, with the hope of achieving a complete remission. For those with relapsed disease or more adverse risk AML subtypes, treatment goals often shift to achieving remission to allow for potentially curative allogenic hematopoietic stem cell transplantation. 9
Complete remission rates with “7 + 3” are ∼70%; however, patients are often simultaneously balancing a chance of cure with a risk of death, and can experience significant physical and psychological symptom burden that negatively impacts their quality of life (QOL).10–13 Furthermore, YAs with AML can have marked life disruptions with this unpredictable illness trajectory and prolonged induction hospitalization, further conflicting with normal development at this stage. 14
Few studies of solid tumor malignancies have compared psychological distress of YAs with older adults undergoing cancer treatment.15,16 However, since the treatment of AML is fundamentally different from solid tumors, we lack an understanding of the YA experience in AML induction compared with their older counterparts. This study, to our knowledge, is the first to explore prospective patient-reported outcomes (PROs), including QOL and physical and psychological symptom burden, among YAs with AML undergoing induction chemotherapy.
Materials and Methods
Participants and procedures
We conducted a secondary analysis of PROs for hospitalized YAs with high-risk AML receiving intensive chemotherapy, collected during a multisite, nonblinded randomized clinical trial of integrated palliative care (PC) intervention versus standard oncology care. 17 In the primary study, high-risk AML was defined as (1) patients aged ≥18 years with relapsed or primary refractory AML, (2) newly diagnosed patients ≥18 years with an antecedent hematologic disorder or therapy-related disease, and (3) older patients ≥60 years with a new diagnosis of AML. 17 Intensive chemotherapy was defined as a combination of cytarabine and anthracycline (“7 + 3” regimen) or a modification of this regimen on a clinical trial with additional drug(s) added, or other intensive chemotherapy regimens requiring a 3- to 6-week hospitalization. 17
One hundred sixty participants were enrolled from January 2017 to July 2019 at participating sites in the United States, including Massachusetts General Hospital, Duke University Hospital, University of Pennsylvania Health System, and The Ohio State University Comprehensive Cancer Center. Study approval was obtained from the institutional review boards at all participating sites and followed Consolidated Standards of Reporting Trials reporting guidelines. Participants completed study questionnaires at baseline and weeks 2, 4, 12, and 24 after enrollment. For the purposes of this study, we focused our secondary analysis on the earlier time points (baseline, week 2, and week 4) to specifically report on the induction hospitalization experience.
Study measures
We used validated self-report measures to assess PROs, including QOL, symptom burden, and psychological distress during induction hospitalization. We used the 44-item Functional Assessment of Cancer Therapy-Leukemia (FACT-Leu), which includes five subscales to assess well-being categories of physical, social/family, emotional, functional, and leukemia-specific concerns (score range 0–176, higher score indicates better QOL). 18 We used the revised 10-item Edmonton Symptom Assessment Scale (r-ESAS) to assess general symptom burden (score range 0–100, higher score indicates greater symptom burden). 19
To capture psychological distress, we used the 14-item Hospital Anxiety and Depression Scale (HADS), which consists of 2 subscales assessing symptoms of anxiety and depression (score range 0–21, higher score indicates more distress), with a score of >7 indicating clinically significant symptoms. 20 We also assessed depression with the 9-item Patient Health Questionnaire (PHQ-9) that can be evaluated continuously, with higher scores indicating worse mood. 21 Finally, we used the 17-item civilian version of the Post-Traumatic Stress Disorder (PTSD) Checklist-Civilian (PCL-C) to evaluate post-traumatic stress symptoms (PTSS; score range 17–85, higher score indicates worse PTSS). 22
Statistical analysis
We used descriptive statistics to summarize participants' baseline characteristics and to compare PROs between YAs (<40 years) and older adults (≥40 years) using frequency and percentage for categorical variables, and median or mean and standard deviation (SD) for continuous variables (e.g., age and PRO scores). We used linear regression models controlling for PC intervention effect when examining the association between age (YAs vs. older adults) and PROs at week 2. Given the results of the primary study that demonstrated the PC intervention to have significant improvements in QOL and psychosocial distress (anxiety, depression, and PTSD), 17 it was important to adjust for this variable in our secondary analysis.
We used linear mixed-effects models controlling for randomization to the PC intervention to assess the association between age and PROs longitudinally throughout the hospitalization. For these analyses, we report the beta estimated coefficient (β). A positive β coefficient indicates a positive association between age <40 and the outcome of interest, whereas a negative β coefficient indicates a negative association between age <40 and the outcome of interest.
Results
Patient participants and baseline PROs
Of the 160 hospitalized patients with high-risk AML enrolled in this study, 14 (8.8%) were YAs <40 years with median age 30.9 (range 19.7–38.3) years. Demographic characteristics, as shown in Table 1, highlight that the majority of YAs had relapsed AML (n = 10, 71.4%), while newly diagnosed AML was more common in older adults. There was also a greater presence of racial and ethnic diversity among YAs.
Patient Characteristics and Baseline Patient-Reported Outcomes
AML, acute myeloid leukemia; ESAS, Edmonton Symptom Assessment Scale; FACT-Leu, Functional Assessment of Cancer Therapy-Leukemia; HADS, Hospital Anxiety and Depression Scale; PCL-C, PTSD Checklist-Civilian; PHQ-9, 9-item Patient Health Questionnaire; PRO, patient-reported outcome; PTSD, post-traumatic stress disorder; SD, standard deviation.
The baseline mean QOL score on the FACT-Leu for YAs was 110.5 (SD 34.2) compared with 117.5 (SD 23.4) for older adults, with additional mean baseline PRO scores demonstrated in Table 1. At baseline, 57.1% (8/14) of YAs reported clinically significant anxiety compared with 34.2% (50/146) of older adults. Furthermore, 50% (7/14) of YAs reported clinically significant PTSD symptoms compared with 24.7% (36/146) of older adults. Fewer YA patients, 21.4% (3/14), reported clinically significant depression at baseline compared with 27.4% (40/146) of older adults.
PROs at week 2
Evaluation of PROs at week 2 of hospitalization, adjusted for randomization to the PC intervention, highlighted a significant worse QOL (β = −18.27; 95% confidence interval [CI], −35.36 to −1.17; p = 0.036), higher anxiety (β = 2.72; 95% CI, 0.03 to 5.42; p = 0.048), and higher PTSD symptoms (β = 10.34; 95% CI, 2.86 to 17.83; p = 0.007) for YAs compared with older adults, as shown in Table 2. There were no significant differences in general symptom burden or depression.
Comparison of Patient-Reported Outcomes at Week 2
All analyses controlled for randomization to the palliative care intervention.
CI, confidence interval; QOL, quality of life.
Longitudinal PROs
Longitudinal analyses exploring the impact of age on PROs across the induction hospitalization demonstrated that YAs had persistently significant higher anxiety (β = 3.66; 95% CI 0.48 to 6.84; p = 0.024) and PTSD symptoms (β = 15.64; 95% CI 7.98 to 23.30; p < 0.001) compared with older adults (Fig. 1). There were no significant differences in QOL, depression, or general symptom burden longitudinally.
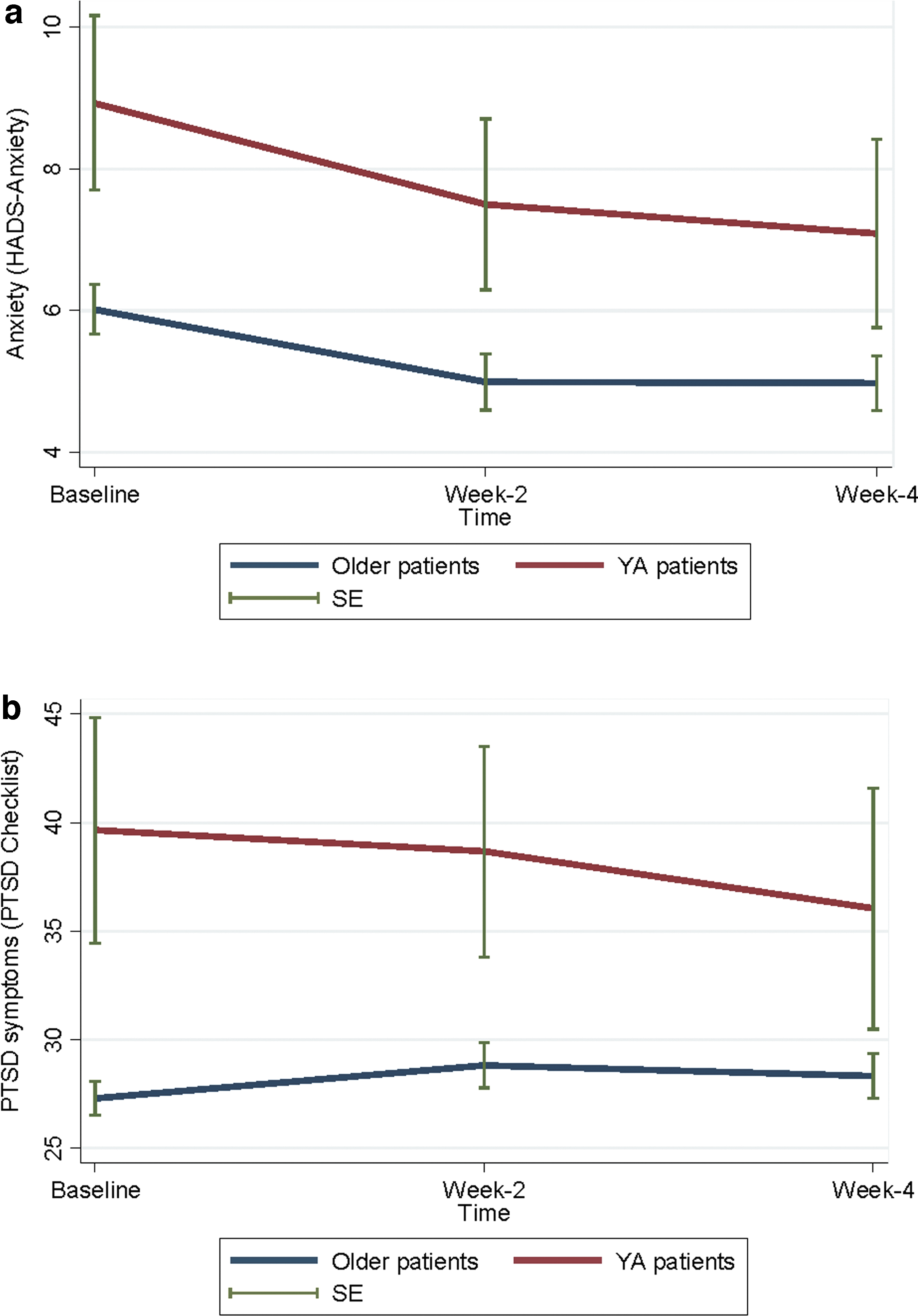
Longitudinal analysis of patient-reported outcomes by scale.
Discussion
In summary, YAs with AML undergoing induction chemotherapy have significantly higher anxiety and PTSD symptoms compared with older adults both at baseline and longitudinally throughout hospitalization. This is a novel finding in an area where little is known about the psychological distress of YAs with AML during the induction hospitalization experience.
It is well recognized that YAs with AML have better overall disease outcomes compared with older adults 23 ; yet, the lengthy hospitalization for induction chemotherapy is met with higher rates of anxiety and PTSD symptoms. These results demonstrate that there is already a significant symptom gap at baseline that is only slightly attenuated by this prolonged hospitalization, risking further isolation and possible derailment of the YA's normal developmental trajectory and goals.
Anxiety and depressive symptoms are often screened as part of routine cancer care, and are highly prevalent in YAs with serious illness. The high rate of PTSD symptoms in this small sample mimics rates in other studies, 24 highlighting the importance of incorporating PTSD symptoms into routine screening, especially for YA patients. Re-experiencing, avoidance, and arousal are often identified in PTSD, and given that most YAs in this study had relapsed AML, this may contribute to the high rates of psychological distress given the re-experiencing of disease and prior treatments. In addition, studies have shown that patients with relapsed AML identify greater distress, higher symptom burden, and worse QOL compared with patients with de novo AML or those in remission. 25
In addition, YAs reported significantly worse QOL compared with their older counterparts at week 2, which is often the most symptomatic phase of the intensive chemotherapy hospitalization when cell counts are at nadir. 13 This further emphasizes the impact of symptom intensification on perceived QOL and the potential role for PC in addressing and alleviating symptom burden. Early integration of specialist PC into standard oncology care can improve PROs such as QOL, symptom burden, health care utilization, goal-concordant care, and even survival in solid tumors and hematologic malignancies.26–32 Growing evidence now demonstrates this benefit too in patients with AML undergoing induction chemotherapy. 17 Yet, many challenges still exist for PC integration into YA cancer care.33–35
Although the small sample size is a notable limitation, results suggest opportunities for future hypothesis-generating research. In addition, our finding that the majority of YAs had relapsed AML was directly influenced by our inclusion criteria. Newly diagnosed YA AML patients are often considered to have more favorable risk disease that is highly curable with intensive chemotherapy alone, and given our high-risk AML inclusion criteria this largely meant relapsed disease for YAs.
Our participant demographics present a limitation of generalizability, given the lack of diversity in representation of race and ethnicity (e.g., only 3.1% of participants identified as Hispanic). There are continued disparities of mental health prioritization, access, and adherence influenced by many factors, including race and ethnicity. Future studies should explore specific barriers, facilitators, and the design of interventions to better promote mental health equity. Furthermore, other demographic characteristics (e.g., relationship status and education) may influence PROs, and thus could be adjusted for in a future study.
Future studies should also include evaluating psychological distress in YA patients with AML undergoing induction chemotherapy in different settings (e.g., pediatric vs. adult hospital). As this patient population can overlap between pediatric and adult health care systems, depending on the treating location, YAs may have variable access to PC and other important supportive services throughout induction. For example, pediatric PC often incorporates unique disciplines that serve as excellent psychosocial support, including psychologists and child life specialists that are less available in the adult health care setting, and may impact anxiety and PTSD symptoms.
Finally and more broadly, in the published literature and clinical trials, there is significant heterogeneity of PRO measures and timing of administration. 36 Future studies should attempt to minimize this heterogeneity to allow for comparison of PRO scores even between studies to further aid in interpretation of outcomes.
Conclusions
For YAs with AML undergoing induction chemotherapy, anxiety and PTSD symptoms are highly prevalent both at baseline and longitudinally throughout the induction hospitalization. This demonstrates a continued unmet need for the significant psychological distress and intensified hospitalization experience for YAs compared with older adults. Given that distress during induction hospitalization can be predictive of post-treatment outcomes, it is imperative to tailor integrated supportive care and psychosocial interventions for YAs with AML during induction chemotherapy.
Footnotes
Acknowledgments
The authors thank all the patients, clinicians, and sites (Massachusetts General Hospital, Duke University Hospital, University of Pennsylvania, and The Ohio State University Comprehensive Cancer Center) who participated in the primary study from which data were collected for this secondary analysis. Special thanks to Ellin Gafford, MD, a pioneer palliative leader, for facilitating collaboration and inclusion of Ohio State in the primary study.
Authors' Contributions
B.J.L. contributed to conceptualization, investigation, visualization, writing—original draft, writing—review and editing. A.E.-J. contributed to conceptualization, methodology, investigation, formal analysis, writing—review and editing. S.E. contributed to conceptualization, writing—review and editing. A.R.W., D.R., J.G., S.S.K., T.W.L., and S.M.L. carried out investigation. S.B.-B. and M.L. performed writing—review and editing. B.B. contributed to conceptualization, investigation, supervision, and writing—review and editing. All authors performed review and approval of the final article.
Disclaimer
Partial results were included in a poster presentation at the American Society of Hematology (ASH) annual virtual meeting in December 2020.
Author Disclosure Statement
T.W.L.: Grant/Research/Clinical Trial Support: AstraZeneca, BMS, Jazz Pharmaceuticals. Consultant/Advisory Boards: AbbVie, Acceleron, Agios/Servier, Astellas, AstraZeneca, BlueNote Therapeutics, BMS/Celgene, Flatiron, Genentech, GSK, Jazz Pharmaceuticals, Novartis, Pfizer. Speaker's Bureau: AbbVie, Agios/Servier, BMS/Celgene. B.B.: Research support from Karyopharm Therapeutics, Cell Therapeutics, Inc., and Sumitomo Pharma Oncology. Honoraria for advisory boards from Karyopharm, Cell Therapeutics, Astellas, Kite, Novartis, Pfizer. All other authors have no conflicts of interest to disclose.
Funding Information
This secondary analysis was performed without funding. For funding information that supported the primary study, see the referenced article by El-Jawahri et al. 17