
Abstract
Purpose:
Treatment sequelae compromising reproductive health are highly prevalent in childhood cancer survivors, and a main determinant of health and quality of life. Follicular reserve determines ovarian function life span; thus, its preservation is important in the care of female survivors. Anti-Müllerian hormone (AMH) is a biomarker to measure functional ovarian reserve. We aimed to evaluate the effect of leuprolide during gonadotoxic therapy on pubertal females' post-treatment functional ovarian reserve using AMH levels.
Methods:
We conducted a single-center retrospective study including all pubertal females who had undergone gonadotoxic treatments between January 2010 and April 2020, and had an AMH level after completion of therapy. We used multivariable linear regressions to compare AMH-level beta coefficients in patients stratified by gonadotoxic risk, adjusting for leuprolide use.
Results:
Fifty-two females meeting study eligibility were included, of which 35 received leuprolide. The use of leuprolide was associated with higher post-treatment AMH levels in the lower gonadotoxic risk group (beta 2.74, 95% CI 0.97–4.51; p = 0.004). This association was lost in the higher gonadotoxic risk groups.
Conclusions:
Leuprolide may have a protective effect on the functional ovarian reserve. However, this is limited by increasing treatment gonadotoxicity. Larger, prospective studies are needed to elucidate the potential benefits of gonadotropin-releasing hormone agonist on preservation of ovarian reserve among children receiving gonadotoxic therapies, as cancer survivors.
Background
An estimated one in 750
Ovarian reserve is established during fetal life and starts declining thereafter. As it depletes, hormonal deficiency and decreased reproductive function ensue. 3 Cancer and its treatment often have a gonadotoxic effect, hastening the reduction in the ovarian reserve and resulting in primary ovarian insufficiency.4,5 This risk is higher among those receiving ovarian exposure to ionizing radiation, chemotherapy with alkylating agents, and to a lesser extent heavy metal agents.5–9 Age at time of treatment, cumulative doses of alkylating agents, and radiation have a direct relationship with the magnitude of the gonadotoxic effect.4,9
Anti-Müllerian hormone (AMH) is a glycoprotein exclusively secreted by the gonads. In the ovaries, it is secreted by primordial and small, growing follicles. AMH is an excellent biomarker to indirectly measure the functional ovarian reserve because 10 of the following: (1) it is stable throughout and in between the menstrual cycles, 11 (2) it can be used in young girls with known reference values, 12 (3) its decline precedes changes in other markers of ovarian function,9,13 and (4) it also allows a quantitative assessment of ovarian injury after gonadotoxic treatment in childhood.14,15
Gonadotropin-releasing hormone (GnRH) agonists bind to GnRH receptors in the anterior pituitary and downregulate the pulsatile secretion of gonadotropins, resulting in a hypogonadal state. The use of these drugs during gonadotoxic therapies appears to protect ovarian function in adults undergoing treatment for breast cancer.16,17 The exact mechanism by which the GnRH agonist could exert this gonadoprotective effect is not well understood, but several hypotheses have been proposed including 18 the following: (1) an interruption of the accelerated follicular recruitment preventing the effect of antineoplastic agents on rapidly reproducing cells, 19 (2) hypoestrogenic decrease in the utero-ovarian perfusion limiting cumulative ovarian exposure to chemotherapy agents,20,21 (3) a direct action on GnRH receptors on the ovary,22,23 and (4) an upregulation of sphingosine-1-phosphate decreasing follicular apoptosis ovary,24,25 among others.
However, this effect in other diagnoses and populations remains controversial at best,18,26,27 particularly in the pediatric population, where studies are scarce and limited.28,29 Hence, we aimed to explore the effect of GnRH agonist treatment with leuprolide, during gonadotoxic therapy in pubertal females' post-treatment functional ovarian reserve, using AMH as a marker.
Methods
Subject, design, and population
This study was approved by the Baylor College of Medicine Institutional Review Board. The retrospective study consisted of a convenience sample of patients who had received care at Texas Children's Hospital (Houston, TX) and received any chemotherapeutic drug between January 2009 and April 2020. The study included all female patients, older than 10 years of age who were pubertal (based on documented physical examination findings or history of menarche), and who had an available AMH level in the medical record after completion of therapy.
Demographics, diagnosis, and treatment characteristics (chemotherapy cumulative doses, total ovarian radiation absorbed dose, hematopoietic stem cell transplant, and surgical history involving the ovaries) were extracted from the electronic medical record (EMR). Age at diagnosis for those with neoplasms was determined by oncology documentation, while for non-neoplastic diagnosis, it was established by the age at the time of treatment initiation. Subsequently, the cyclophosphamide equivalent doses (CEDs) were calculated for those who received any alkylating agent, using the methods described by Green et al. 30
We excluded those individuals who were prepubertal (based on absent menarche and thelarche as documented on history and physical examination), had a history of ovarian neoplasm, oophorectomy, ongoing or absence of gonadotoxic treatment (alkylating agents, platin-based drugs, or radiotherapy), or had incomplete records of cancer therapy. Patients were divided in two groups, according to administration of leuprolide during gonadotoxic treatment. Using The Oncofertility Consortium's Pediatric Initiative Network risk-stratification system developed by Meacham et al, 31 both groups were stratified by gonadotoxic risk category as follows: (1) minimally increased risk, (2) significantly increased risk, and (3) high level of increased risk.
AMH levels
Information on AMH levels, and time from completion of gonadotoxic treatment, was abstracted from the EMR. Samples were collected as part of routine clinical care, and were processed by LabCorp®, Quest Diagnostics™, ARUP Laboratories, or our institutional laboratory as per insurance requirements. Information about the assay used was obtained by direct inquiry with the processing laboratory. In those with multiple AMH levels available, the last AMH was used for analysis.
Leuprolide therapy
Leuprolide has been used in our institution, at the medical providers' discretion, to decrease thrombocytopenia-associated menorrhagia. Information regarding dose received, number of doses, and time of administration relative to gonadotoxic treatment was extracted from each patient's EMR. Patients received the first dose of leuprolide ≥14 days from initiation of gonadotoxic treatment, as done on previous studies evaluating the use of GnRH agonist for fertility preservation. 18 Those who received it inconsistently throughout the duration of the gonadotoxic therapy, or those who had previously received any gonadotoxic therapy before initiation of leuprolide were also excluded. Thus, if patients with disease recurrence were being retreated with gonadotoxic therapy, but leuprolide was only given during initial treatment, they were included up until initiation of treatment for recurrence, if an AMH level was available.
Statistical analyses
Patients were categorically grouped by use of leuprolide. Then demographic and clinical characteristics between groups were described and compared using either the chi-squared or Fisher's exact test for categorical variables and Student's t-test for continuous variables. AMH levels were interpreted using a validated model for normal reference values for age. 32 The AMH level for each subject was calculated by subtracting the age-specific modeled mean value from the value for the individual, then dividing that value by the standard deviation (SD) from the modeled population values. The formula was (X − Xmean)/SD. The value therefore represents the number of SD a given individual's AMH level lies above or below the expected mean AMH level for age.
Subsequently, using multivariable linear regression models, we examined the effect of the use of leuprolide on AMH level adjusting for type diagnosis; age at diagnosis; ethnicity; age at diagnosis, time from completion of treatment; AMH assay used; CED received; and ovarian exposure to radiation and particle used (photons or protons). A p-value of <0.05 was considered statistically significant. Thus, a change in the beta coefficient value indicates the effect of the predictor variables on the AMH level. All statistical analyses were conducted using Stata 16 (StataCorp LP, College Station, TX).
Results
The initial data set comprised 256 individuals. A total of 204 were excluded (Fig. 1) resulting in a final sample of 52 females, of which 35 had received leuprolide and 17 had not. Baseline characteristics are presented in Table 1. There were no differences in ethnicity, diagnoses, or gonadotoxicity of treatments received between the groups. The majority (76.9%) had an oncologic diagnosis, while seven (20%) in the leuprolide and five (29.4%) in the no-leuprolide had a hematologic or immune-derived condition such as sickle cell disease, myelodysplastic disorders, or systemic lupus erythematosus. Six individuals per group had undergone hematopoietic stem cell transplant, and four (66.7%) and five (83.3%) in the leuprolide and no-leuprolide group for non-neoplastic conditions.
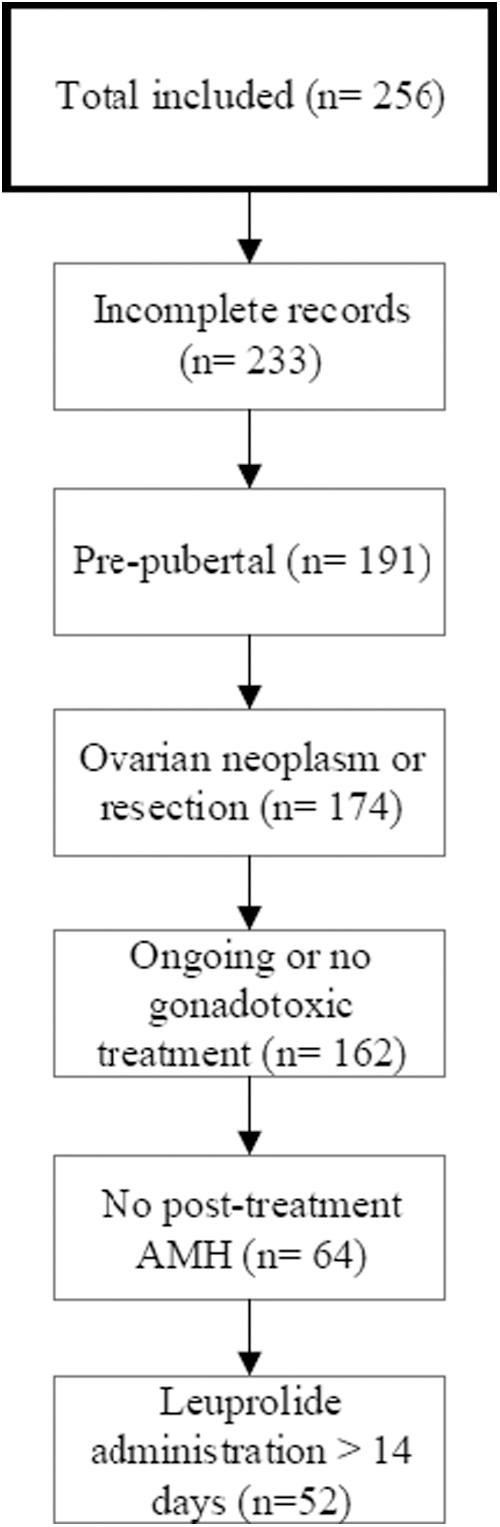
Sample selection for analysis.
Demographics, Disease, and Treatment Characteristics by Leuprolide Use
AMH, anti-Müllerian hormone.
A total of six patients received radiotherapy, two received total body irradiation with photon therapy, while the remaining four underwent craniospinal radiation with proton therapy. None of these had an ovarian absorbed dose ≥0.1 Gy. The radiation scatter map for one individual was unavailable, and thus was assumed to have had ovarian exposure to radiation ≥0.1 Gy. However, this did not alter the risk stratification since she was already classified as high level of increased risk based on a received CED >8 g/m2.
The AMH levels were plotted in the validated age-based nomogram by age at the time of collection, then grouped by leuprolide use, and by gonadotoxic risk from the treatment received (Fig. 2). There was an indirect relationship between gonadotoxic risk and functional ovarian reserve, with 5/23 (21.7%), 7/17 (41.2%), and 12/12 (100%) of individuals with an AMH level ≤ −2 SD in each risk group, respectively. Those receiving leuprolide had larger functional ovarian reserve (AMH levels > −2 SD), when compared with those who did not (23/35 (65.7%) vs. 5/17 (29.4%)).
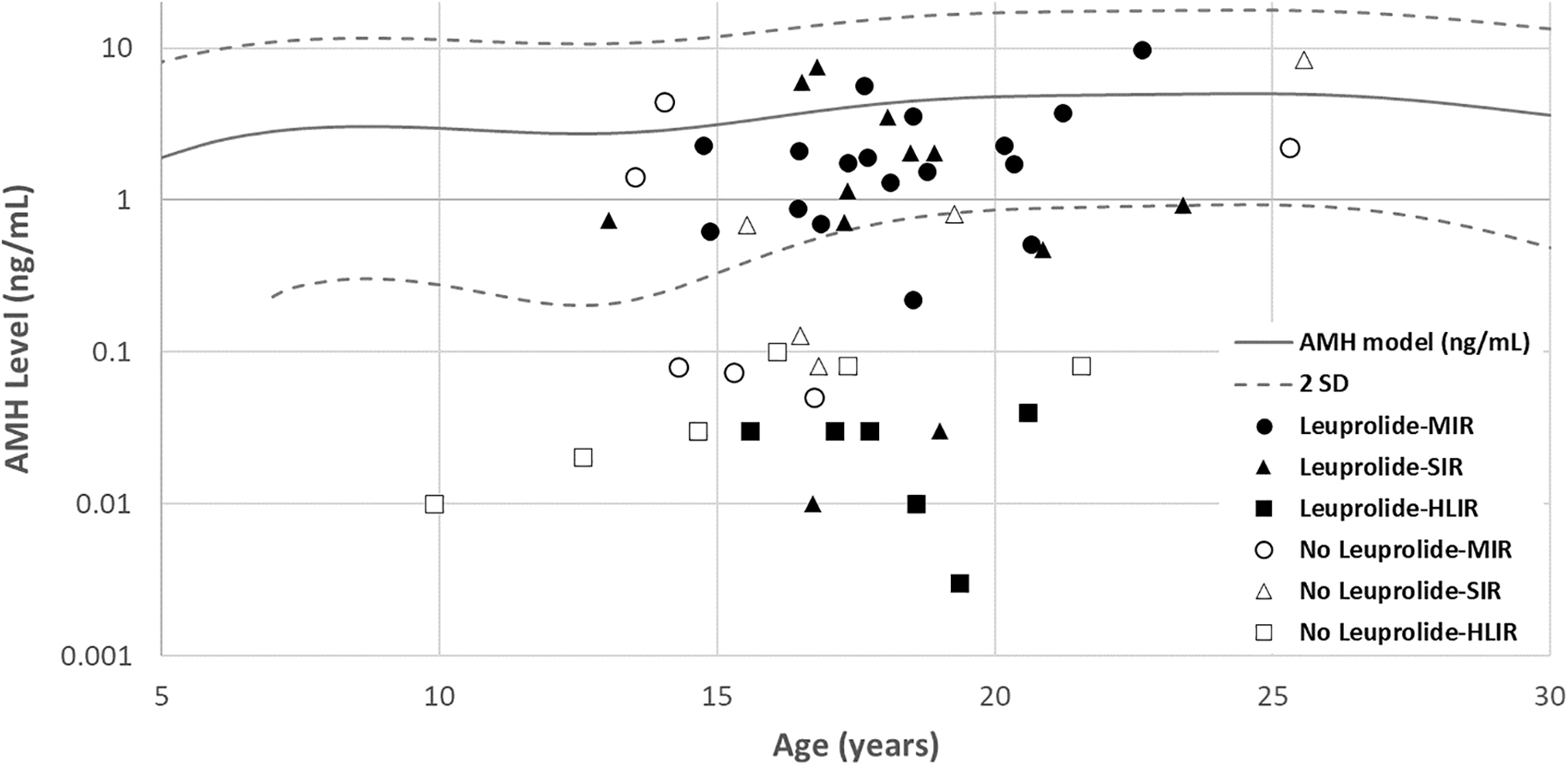
Anti-Müllerian hormone levels plotted in age-based nomogram by age at the time of collection. HLIR, high level of risk; MIR, minimally increased risk; SD, standard deviation; SIR, significantly increased risk.
Initial regression models showed a lack of statistically significant difference between the AMH level groups after adjusting for leuprolide use, age at diagnosis, and time from completion (p > 0.05). Similar results were seen after incorporating cumulative CED (mg/m2) and ovarian exposure to radiation to the model (p > 0.05). Further adjusting for ethnicity, diagnosis, or AMH assay used also failed to show a significant effect, and thus, these were excluded from subsequent analyses. The type of particle used for radiotherapy (photons or protons) was excluded from the models due to insufficient sample size.
When patients were stratified by gonadotoxic risk group, the use of leuprolide was associated with a statistically significant higher post-treatment AMH level in the minimally increased risk group, after adjusting for age at diagnosis and time from completion (beta 2.74, 95% CI 0.97–4.51; p = 0.004), whereas this effect lost significance in the significantly increased risk (beta 0.31, 95% CI −2.85 to 3.48; p = 0.84) and high level of increased risk (beta −0.34, 95% CI −0.1 to 0.08; p = 0.15) groups.
Discussion
In this study, we observed that the use of leuprolide in pubertal females during gonadotoxic treatment was associated with a higher post-treatment AMH level overall. The majority of the patients receiving leuprolide had normal (>−2 SD) functional ovarian reserves, contrary to those who did not. The use of leuprolide during treatment minimally increased risk for gonadotoxicity, resulted in higher AMH levels after controlling for age at diagnosis, and time from completion of treatment. However, this effect of leuprolide appears curtailed by increasing treatment gonadotoxicity, as those in the significantly increased risk and high level of increased risk groups did show the same effect. This higher post-treatment AMH among those subjects receiving leuprolide, compared with those who did not, indicates a reduced ovarian injury from gonadotoxic therapies, suggesting that leuprolide use may exert a protective effect on functional ovarian reserve in pubertal girls undergoing gonadotoxic treatment, approximating their levels to those of healthy, age-matched peers.
Similar results were reported by Pereyra Pacheco et al in a small pediatric group. 29 However, they studied the effect of GnRH agonist on ovarian function, not reserve, by using menstrual history and pregnancy as outcomes. Instead, by using AMH as an outcome, we were able to examine an objective, quantifiable effect on the ovarian reserve that long precedes changes on menstrual periods.9,13–15
The exact mechanism by which the GnRH agonist could exert this gonadoprotective effect is not well understood, but several hypotheses have been proposed including 18 the following: (1) an interruption of the accelerated follicular recruitment preventing the effect of antineoplastic agents on rapidly reproducing cells, 19 (2) hypoestrogenic decrease in the utero-ovarian perfusion limiting cumulative ovarian exposure to chemotherapy agents,20,21 (3) a direct action on GnRH receptors on the ovary,22,23 and (4) an upregulation of sphingosine-1-phosphate decreasing follicular apoptosis ovary,24,25 among others.
In children undergoing cancer therapy, AMH levels decline during treatment, with a recovery period of 20 months until stabilization at its post-treatment levels. 33 When measured 2 years after completion of therapy, the AMH is an excellent predictor of ongoing menses the following 3 years. 34 Thereafter, the rate of AMH decline among female CCS is similar to age-matched healthy controls. 35 Thus, post-treatment AMH levels closer to the age-matched mean may predict an ovarian function life span similar to healthy counterparts.
While a larger functional ovarian reserve would potentially translate to better reproductive health outcomes, this does not necessarily equate to improved fertility, considering that actual childbearing entails many other intricate factors. Nonetheless, AMH levels have shown to be a good outcome predictor after assisted reproductive techniques, thus potentially improving the chances of future fertility. 36 As such, for those female CCS who do exhibit higher post-treatment AMH levels following concurrent use of leuprolide, this could translate to a potential improvement in fertility outcomes.
Reproductive health is a common concern for both female CCS and their families, and a main determinant of quality of life after cancer therapy.37,38 Hence, oncofertility counseling is recommended for all patients before initiation of treatment, with referral for fertility preservation when interested.39–41 Unfortunately, due to a myriad of factors and barriers, fertility preservation remains underutilized, particularly in the pediatric population.42–45 Some of the most prominent barriers are the financial toxicity of these techniques, along with the invasiveness of oocyte or embryo harvesting for cryopreservation.
Conversely, GnRH agonists such as leuprolide are safe, minimally invasive, and inexpensive compared with other available interventions. Currently, none of the existing fertility preservation techniques enables the prolongation of the ovarian endocrine function, except perhaps ovarian tissue autotransplantation, which is costly, invasive, and still being optimized.46,47 The GnRH agonist therapy may be especially useful in extending the life span of ovarian endocrine function, thus mitigating the detrimental effects of premature menopause including but not limited to low bone mineral density, poor linear growth (in those with open growth plates), global neurocognitive decline or dementia, parkinsonism, anxiety, depression, and cardiovascular disease.48–52 Furthermore, this prolongation of ovarian life span may open a window for fertility preservation after completion of treatment, enabling adolescents, especially those who were started on treatment at an early age, to reach a more mature stage in their life in which oocyte harvesting becomes more feasible from a psychosocial standpoint.
Finally, GnRH agonists have the added benefit of decreasing the need for blood products in postmenarchal females with thrombocytopenia and menorrhagia, reducing potential complications and costs related to transfusion of blood products.53,54 Nonetheless, it is important to emphasize that to date, the accrued evidence to support the use of these drugs for fertility preservation is scarce, particularly in those receiving significantly intense gonadotoxic treatments. 40 Thus, leuprolide and other GnRH agonists should not be used in place of other proven fertility treatment techniques, but perhaps as an adjunct therapy.
This study had limitations inherent to the retrospective design such as the lack of randomization, the heterogeneity in the dosing and timing of leuprolide administration, short time of AMH collection in regard to completion of treatment, and the difficulty interpreting different AMH assays. However, multivariable modeling failed to identify any significant differences arising from these factors supporting the validity of our results. Similarly, body mass index has been reported to have a modest negative effect on AMH levels. 55 However, conflicting results have been reported on this, and limited to adult population.56,57 Our study included patients with nononcologic diseases undergoing gonadotoxic therapies. Although multivariable analyses failed to show a significant effect of controlling by diagnosis, generalization of these results exclusively to the field of oncofertility should be pursued with caution.
Finally, the study may have been underpowered, failing to detect the effect of leuprolide, if any, in the moderately and high levels of increased risk groups.
To the best of our knowledge, this is the first study evaluating the role of GnRH agonist in the functional ovarian reserve in an exclusively pediatric-age cohort. Furthermore, given the paucity in post-treatment ovarian reserve outcomes, routinely using AMH as a marker specific to this group, this is the largest study to date to examine this. Using a validated age-adjusted model allowed us to minimize the normal age-related variations on AMH levels, unmasking any external effects. Future work needs to be conducted to replicate and refine the results reported here.
Conclusion
In this retrospective study, we found that the use of leuprolide during gonadotoxic treatment was associated with a higher post-treatment AMH level in females receiving gonadotoxic therapies that were at minimal risk for gonadotoxicity, suggesting that leuprolide may have a protective effect on the functional ovarian reserve of those who received these therapies. However, such effect seems to be limited by increasing treatment toxicity. Larger, prospective studies are needed to elucidate the real extent of the benefits of GnRH agonist in the field of pediatric oncofertility. Until then, the use of these medications should not replace proven fertility preservation techniques.
Footnotes
Authors' Contribution
All the listed authors certify that they have participated sufficiently to meet the criteria for authorship, and take public responsibility for the content of this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.