
Abstract
Introduction:
The COVID-19 pandemic caused widespread disruption to the provision of health care in the United Kingdom. It posed two risks to AYACs: disruption of care and long-term adverse consequences compounding late effects. This study sought to better understand the experiences of AYACs receiving care during the pandemic and identify areas where greater support is needed.
Methods:
In-depth semistructured interviews with AYACs (n = 6), 16–22 years at diagnosis. Interviews were transcribed verbatim and analyzed using the principles of Giorgi's phenomenological analysis.
Results:
Four major themes and an interconnected theme were identified. Changes to health care meant AYACs were isolated and loss of in-person follow-up caused anxiety (theme 1). AYACs had to adapt to life with COVID-19 restrictions (theme 2). Support during the pandemic came from a variety of sources (theme 3). AYACs reported poor mental health due to a fear of relapse and contracting COVID-19 (theme 4). An additional burden for AYACs was the loss of the third person (e.g., parent) in consultations (interconnected theme).
Conclusion:
This study has wider implications for delivery of AYAC care, despite being set during the COVID-19 pandemic. The mental health implications will impact long-term care of these patients, and health care professionals must be aware of these to meet AYACs' holistic care needs.
Background
During the COVID-19 pandemic, the United Kingdom (UK) entered 3 “lockdowns” from March 2020 to July 2021 (Fig. 1), with significant implications for cancer care. Hospital policies were adapted to meet the increasing demands on capacity for COVID-19 patients and new infection control measures implemented: appointments and treatments were postponed, strict visiting restrictions were imposed, 1 wards were restructured to minimize patient mixing and, telehealth (the provision of health care remotely using telecommunications technology) was introduced. Studies in the USA and Canada have demonstrated both physical and psychosocial consequences for adolescents and young adults with cancer (AYACs; 13–24 years of age) as a result of these modifications.2–5
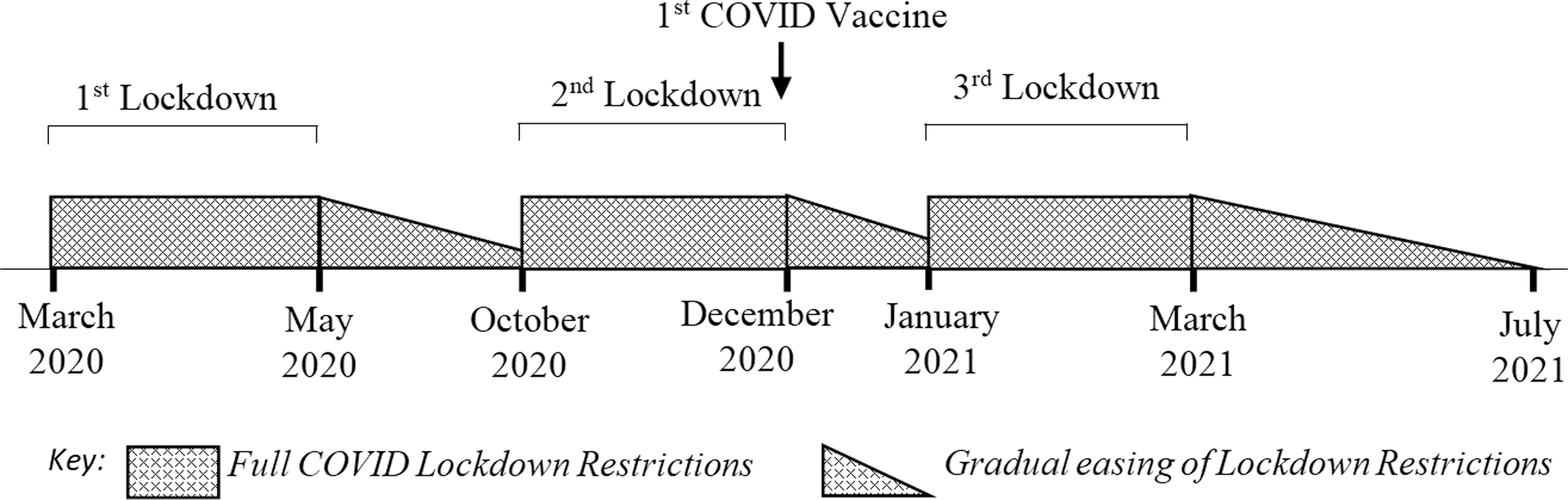
Timeline of the implementation and withdrawal of UK “lockdown” measures. Lockdowns encompassed several infection control measures, including stay-at-home orders, isolation of infected individuals and restrictions on social gatherings. These measures were implemented and eased in accordance with COVID-19 rates in the UK. UK, United Kingdom.
Adolescents and Young Adults with cancer have distinct psychosocial and informational needs compared with those of children or adults and often have age-appropriate care in specialist centers to improve outcomes.6–9 This age is a period of transition, which can be disrupted by a cancer diagnosis.10–12 The pandemic significantly interfered with AYAC specialist services, with life outside hospital unrecognizable, and reduced support available in hospital during this crucial developmental time.
With social isolation associated with poorer clinical and psychosocial outcomes, it is pertinent that the long-term effects of lockdowns for the general UK population include anxiety and depression 13 with studies showing that cancer patients of all ages experienced feelings of loneliness throughout the pandemic and the highest levels of such reported by AYACs.4,13–15 Not only are AYA cancer survival rates high (87%) but survivorship (>6 months post-treatment completion) can be long. 16 The potential for serious physical and psychological late effects after cancer treatment is known, however, the capacity of the pandemic to exacerbate feelings of isolation and the potential to compound late effects in survivorship is not known.2,5,17
This study sought to use a qualitative methodology to better understand the experiences of AYACs who received care during the pandemic and identify areas in which they may need greater ongoing support as a result of this.
Methodology
Recruitment and sampling
This study used purposive sampling to select eligible participants from the cohort of patients treated between March 2018 and June 2021 by the East of England Teenage and Young Adult Cancer (TYAC) Service, which treats cancer patients 13–24 years of age. 18 These dates enabled sampling of participants who received active treatment during the COVID-19 pandemic and also those who completed treatment at the start of the pandemic.
Not all of the 49 eligible participants (Fig. 2) were approached, such as those near end of life. Potential participants were invited through email and those who took part received a £20 voucher (≈23 USD), 19 to compensate for time and travel expenses. Attempts were made to recruit eligible participants who did not initially respond with a follow-up email or after clinic appointments.
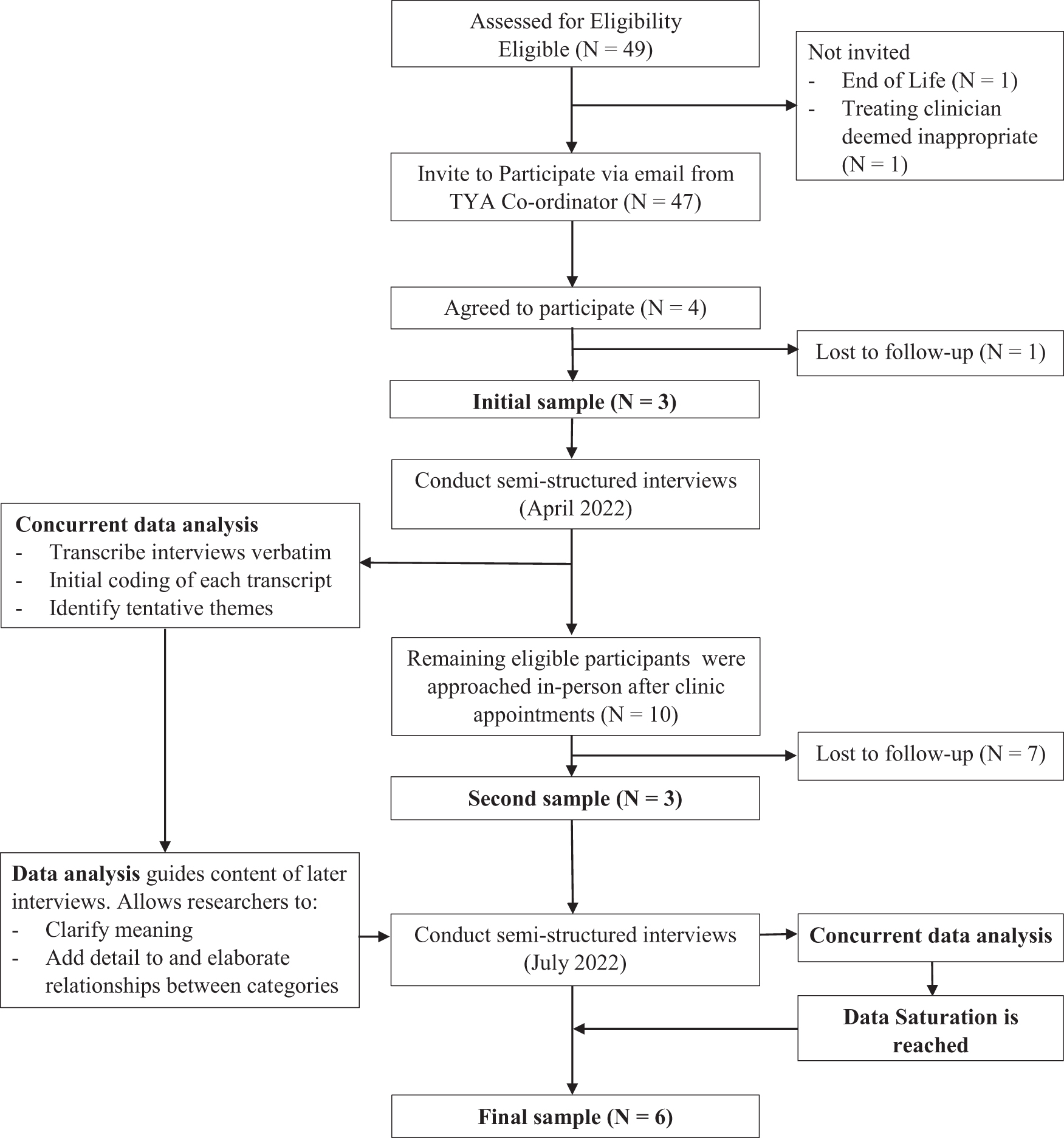
A flow diagram showing concurrent and interdependent participant recruitment, data collection, and data analysis. Data analysis informed semistructured interviews (data collection) and data analysis informed recruitment endpoint (data saturation). The initial invitation to take part in the study was sent out by the TYA coordinator in March 2022, and three participants were interviewed in this first stage. Recruitment for the second round of interviews took place by specialist nurses or doctors approaching eligible candidates at the end of clinic appointments. The second round of interviews took place in July 2022. TYA, teenage and young adult.
Six participants (four male, two female) took part. Age ranges at diagnosis and at interview were 16–22 and 19–25, respectively (Table 1). Participants included those on treatment during the pandemic (n = 4) and those who had completed treatment (n = 2) (Fig. 3). Further detail regarding the relative timings of treatments, the pandemic and interview are detailed in Table 2.
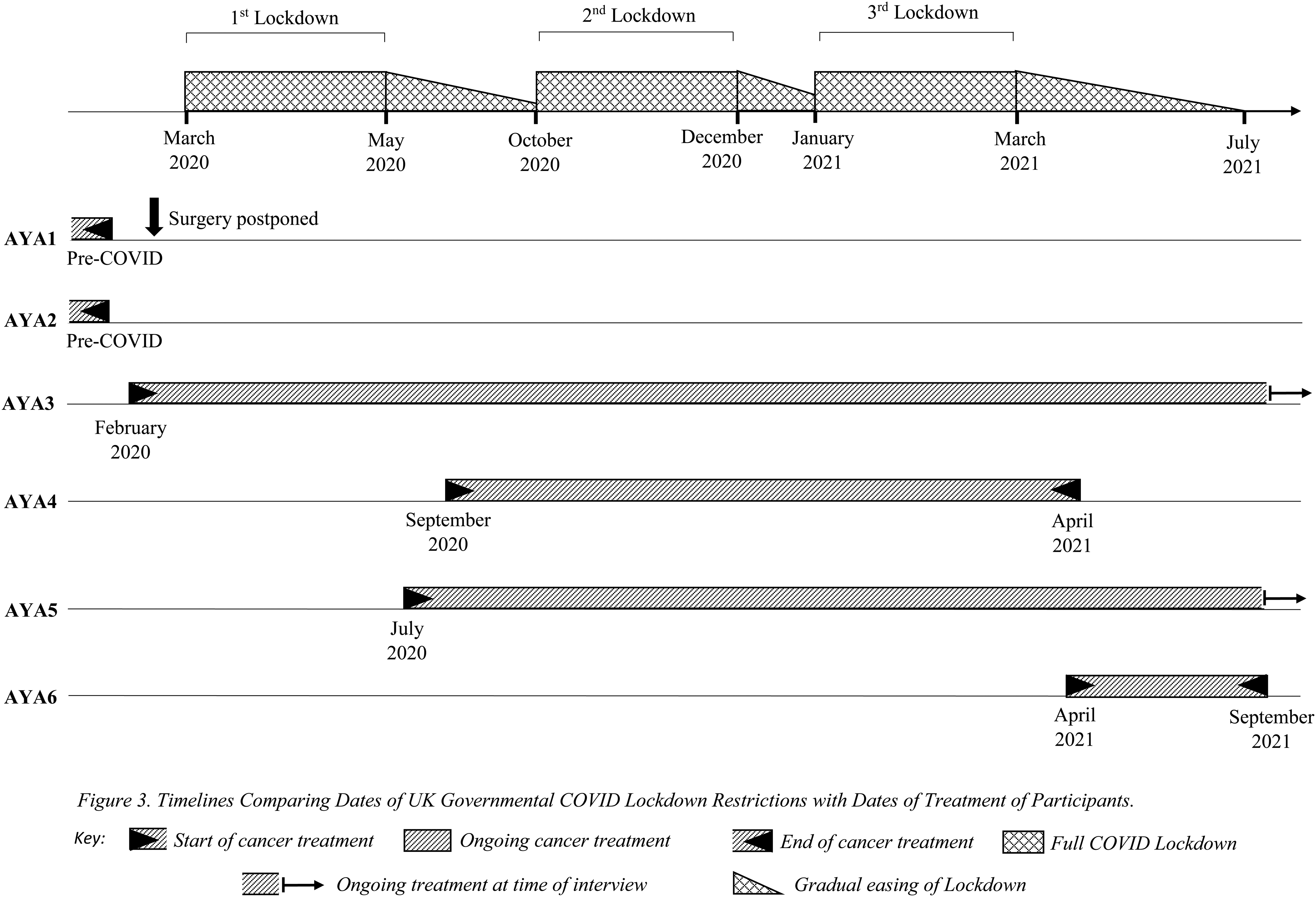
Timelines comparing dates of UK governmental COVID lockdown restrictions with dates of treatment of participants.
Participant Demographics Table
All patients that were interviewed had spent time on treatment in hospital. At the time of their interviews all participants were being managed as outpatients. This study investigated only the 16–24 age range as we received ethics approval to conduct our research in adults (ages >16) and the upper age limit of AYACs in the UK is 24.
AYA, adolescent and young adult; AYACs, adolescents and young adults with cancer.
The Relative Timings of Treatments, the Pandemic, and Interview
Data collection
Six in-depth, semistructured interviews were conducted by A.H. between April and September 2022, and were conducted at participants' convenience. Five interviews were conducted virtually (using video conferencing) to comply with UK Coronavirus guidelines at the time, and one interview was conducted in person.
The interview schedule, including “prompts,” (Table 3) was developed using themes highlighted by similar studies and the researchers' clinical experiences working with AYACs during the pandemic.4,5,20 Interviews were recorded, transcribed verbatim, and subsequently deidentified. Interview mean duration was 1 hour 39 minutes (range: 56 minutes–2 hours 42 minutes).
Interview Guide Sample
Data analysis
This qualitative study was guided by the principles of Giorgi's phenomenological analysis as follows21,22:
Interview transcripts were reviewed in their entirety to obtain a general sense of content Transcripts were then coded for “meaning units” with a focus on the phenomena being researched Meaning units were reviewed and grouped for their ability to explain the behavior underlying the phenomena Final results were presented as themes, kept as descriptive as possible to communicate the meaning and significance of experiences. Illustrative quotations were sought for in the transcripts.
Data analysis occurred concurrently with data collection in an iterative process.23–25 Preliminary analysis from steps 1 and 2 allowed modification of interview guides, while the incorporation of meaning units from later transcripts allowed analysis to be refined. When interviews yielded no new meaning units, data saturation was reached and data collection was stopped.
During analysis, authors noted that some meaning units pertained to all four nascent themes although these meaning units did not fully underly or explain the phenomena of these other themes. Although not part of Giorgi's methodology, a decision was made to include an interconnected theme that represented a unique phenomenon within the data but also had explanatory relevance to the other themes.
Validity of analysis was enhanced by researcher triangulation, with all researchers (an AYAC Lead Consultant, specialist AYAC nurse, junior doctor, and medical student) involved in all aspects of data analysis. The researchers engaged in reflexivity, acknowledging their professional and scientific roles, attitudes, and biases.
Ethics
This study was approved in February 2022 by the South Central—Berkshire Research Ethics Committee (21/SC/0409).
Results
Analysis of AYAC interviews identified four themes and an interconnected theme, summarized in Table 4. Verbatim quotes exemplifying each theme are shown in Table 5 with in-text references.
Descriptions of Themes
Themes and Exemplifying Quotes
ADHD, attention deficit hyperactivity disorder.
Theme 1: Changed health care encounters during COVID-19
Hospital visiting restrictions created a heightened sense of loneliness and isolation
Strict hospital visiting restrictions exacerbated feelings of isolation. As restrictions eased to allow visitors during daytime hours, overnight stays remained prohibited. The large geographical area served by the tertiary center meant long travel distances for supporters which, for some, remained a barrier to daily visits. AYACs had fewer distractions compared with those treated pre-pandemic and described the loss of structure to their days as “boring”[1.a.i,1.a.ii.1.a.iv]. Some AYACs sought out new hobbies such as online gaming. Participants with neurodivergent backgrounds particularly struggled with the lack of stimulation[1.a.iii].
Some AYACs acknowledged visiting restrictions were more upsetting for those who wished to visit[1.a.v]. Others felt protected from the outside world during a vulnerable time when they did not want to be seen[1.a.vi].
Telehealth became commonplace in care delivery
“Telehealth” was increasingly used during the pandemic. Follow-up for participants who had completed treatment when the pandemic began was switched to phone or video calls, whereas those still receiving treatment continued with in-person appointments. Telehealth was challenged by technological issues, such as poor signal[1.b.v].
Telehealth deprived AYACs concerned about relapse of the reassurance of a physical examination[1.b.ii,1.b.iv]. Most AYACs were understanding of the need for telehealth and did not want to add further burdens on the stretched system. However, the convenience of reduced travel requirements with telephone appointments was important to the participants[1.b.vi].
The specialist environment of the Teenage Cancer Trust Unit was at best disrupted and at worst, lost
The Teenage Cancer Trust Unit at Cambridge University Hospitals (CUH) Trust is a dedicated ward with eight beds and a day unit. The unit has different zones for socializing and quiet individual activities. Initially the social room was closed and visitors were not permitted to stay overnight in line with hospital policy. During Winter 2021, the unit was redeployed to manage COVID-19 pressures and AYACs were relocated to adult wards.
Reduced peer support was a compounding source of isolation[1.b.ii]: AYACs were discouraged from interacting to reduce the risk of infection transmission. Some participants preferred beds in mixed bays, rather than individual side rooms as it guaranteed opportunity for socializing[1.c.i]. Others believed that any friendships made were circumstantial and had no desire to meet new people during treatment, nor found comfort in this[1.b.v]. These participants described fewer feelings of isolation. As restrictions on the AYAC ward relaxed, participants enjoyed spending time in other ward areas such as the “social room,” which provided stimulation and variety to their days.
Some participants were treated on a non-specialist ward during the pandemic. One AYAC described “horrifying noise” during an admission to an adult ward[1.b.iii,1.b.iv]. Those participants able to compare experiences on specialist and non-specialist wards reported taking comfort from meeting other AYACs with shared experiences and feeling less isolated on the specialist AYAC ward. Staff on the specialist ward were a key support for AYACs during inpatient stays as they had good rapport and had built trusting relationships.
Theme 2: Living with COVID-19 restrictions
Differing attitudes to “shielding” restrictions
Many AYACs reported confusion over seemingly ever-changing lockdown rules[2.a.iii], with complex guidelines increasing the information burden associated with their diagnoses. In March 2020, those deemed clinically extremely vulnerable to COVID-19 infection were advised by the government to “shield” and undertake additional isolation measures.26,27 Those “shielding” could not leave their homes for leisure or work. At home they were advised to maintain a 3 m distance from others and to minimize time spent with others in communal spaces.
Advice to “shield” received different reactions[2.a.i]. There was confusion regarding individual risk for AYACs who had entered survivorship[2.a.ii] many of whom questioned whether “shielding” was necessary. Some participants found it “scary” to be told that they were vulnerable[2.a.vi]. For others, “shielding” measures resembled the infection control precautions they had been advised to undertake during treatment[2.a.iv] and felt they had lost the opportunity to move on from their diagnosis and treatment. Many participants described only being able to mentally process their experiences once both lockdown restrictions and their treatments were over[2.a.viii].
“Shielding” also exacerbated feelings of difference from healthy peers[2.a.vii]. They found it hard to see others getting on with their lives, which made them feel even further behind. Some AYACs were frustrated with their reliance on others to complete errands such as shopping and bank appointments, having previously been used to independence.
Changes across all aspects of daily life
All participants reported changes to their daily lives and described the first 3 months of UK lockdown measures as the hardest adjustment with the strictest rules and most sudden changes.
Disruption to employment was multifactorial: nonessential sectors closed, AYACs were required to shield, or treatment schedules made employment impracticable[2.b.ii]. The unpredictability of employment created significant financial stress.
Educational institutions were slow to adapt to COVID-19 restrictions, further delaying the educational goals of some participants who had already lost time during treatment[2.b.iii]. The virtual delivery of content allowed AYACs to resume their education without infection concerns, but some participants found this “anti-social” and struggled to connect with classmates[2.b.iv].
Theme 3: Feeling supported during the pandemic
Personal relationships and home life
All participants lived with family or partners when not receiving in-patient cancer treatment and their support was greatly appreciated. Shared experiences of lockdown restrictions both strengthened and strained relationships[3.a.i]. Those living in family homes struggled for privacy, whereas those living with partners missed important family events[3.a.ii]. Participants' clinical vulnerability had consequences for others at home: for example, the education of siblings was disrupted, or partners were furloughed to reduce the risk of infection. Lockdown restrictions posed challenges for AYACs trying to meet new partners or maintain relationships with those they did not live with.
Friendships were a vital source of support during both the pandemic and treatment. When participants felt understood by friends, this reinforced the relationship. Continued socializing retained a sense of normality and most felt comfortable to socialize in-line with lockdown guidance, especially following vaccination roll-outs. However, friendships were divided when attitudes of healthy peers about COVID differed from the AYAC: some found friends unsympathetic or unable to appreciate their vulnerability[3.a.iii].
Staying connected
With lockdown restrictions, online methods of communication predominated and all participants reported greater difficulty maintaining relationships compared with in-person interactions[3.b.i]. AYACs accustomed to socializing in-person, struggled to adapt to a “FaceTime relationship”[3.b.ii]. AYACs who already had an established network of online friends reported less burden on relationships as “nothing changed.”
Social media provided a vital way to connect with friends, but AYACs could see lockdown rules flaunted, which exacerbated feelings of difference from healthy peers. One participant formed an online support group using social media to connect AYACs with shared diagnoses over long distances.
Specialist AYAC services
Despite significant adaptations in the operation of specialist AYAC services, all participants appreciated their ongoing support from these services. For example, the counseling service implemented a telephone service, which provided continuity of care for participants with practitioners they had previously met in person [3.c.i].
A Youth Support Coordinator was restricted to organizing one-to-one meetings over the phone or outdoors rather than organizing group activities. Participants were grateful as this helped pass the time and reduced loneliness[3.c.ii]. As COVID-19 eased, small events such as pizza evenings were organized in the ward's “social room.” Time spent in this less clinical environment helped participants “forget that [they] are a patient.”
Theme 4: Poor mental health
Pre-existing mental health diagnoses, especially anxiety, were exacerbated during the pandemic and some participants received mental health diagnoses. AYAs reported two major anxieties: fear of relapse and of COVID-19 infection[4.i,4.iv]. Some reported increased introversion and reduced confidence because of their health anxieties.
Participants who entered survivorship pre-pandemic were expecting to return to normality and found the imposition of COVID-19 restrictions on their daily life and future plans frustrating and disappointing[4.iii]. The loss of usual coping strategies, such as outdoor exercise, gave AYACs “more time to think” and “sit and worry about things”[4.ii]. Many used online gaming as a form of escapism[4.v]. Participants found returning to old hobbies when restrictions lifted difficult after long periods of time spent in treatment or lockdown[4.vi].
Interconnected theme: loss of the triad
Hospital policy not only reduced ward visitation but also prohibited the attendance of parents, partners, and other family members during clinic appointments. As a result of these changed health care encounters (theme 1), participants described having a significant information burden, often needing to break news of diagnoses or treatment progress to multiple family members[ii]. Without family members, AYACs felt less supported (theme 3) as they no longer had a second person to listen to and understand the consultation[i]. Central to AYA clinical care,28,29 the communication triad was lost (clinician–patient–family member/supporter relationship). 30 Neurodivergent participants reported difficulties adequately understanding and engaging with consultations and one participant asked for email summaries of all important discussions[iii]. Many participants acknowledged the difficulties that loved ones faced living with these COVID restrictions (theme 2) as their families were unable to meet their treating team and ask questions. These additional burdens acted as stressors at a time when participants' mental health (theme 4) was already fragile.
Discussion
This study contributes to the existing body of knowledge about the experiences of AYACs during the COVID-19 pandemic: the pandemic was an additional layer of complexity. Our qualitative methodology revealed four themes and an interconnected theme: changed health care encounters during the COVID-19 pandemic, living with COVID-19 restrictions, feeling supported during the pandemic, and poor mental health. Our interconnected theme “Loss of the triad” was a common element spanning across all four themes.
Existing literature has reported the detrimental effects of visiting restrictions on experiences in hospital and our study further explored the impact of being alone as an AYAC in hospital during treatment.15,31 The necessity of COVID-19 restrictions has provided a unique opportunity to study the significance of a third party in health care encounters and the impact of losing this third party due to visiting restrictions. Without an extra person to listen to consultations, more responsibility was placed on the AYAC to understand the information and relay the information back to loved ones. This was an added burden that was compounded by needing to keep up to date with the ever-changing restrictions. This information was learnt in the COVID-19 pandemic but has wider implications for practice: there are many reasons why a third person may be absent in AYAC consultations.
Risk perception in the AYA population differs between each individual AYA. 32 This study showed variability in individual AYAs' perception of clinical vulnerability to COVID-19. Health care professionals (HCPs) should not assume that AYACs share the same opinion regarding health behaviors simply because they share one demographic. Instead, individual discussion of risk perception can inform assessments of health needs to better provide individualized care, complimenting recommendations in wider medical practice. 33
The effect of AYACs' experiences on their mental health was profound. The mental health effects of a cancer diagnosis in the AYA age group have been long understood,11,12 and the pandemic exacerbated this.2,4,5,16 All participants reported a decline in their mental health due to their experiences during the pandemic. This could be due to increased reports of loneliness and isolation from peers,5,34 or “shielding” requirements and increasing difficulty connecting with existing support networks. Those who entered survivorship shortly before or during the pandemic faced delayed recoveries and an inability to process their experiences, which should be considered during long-term follow-up.
Implications for clinical practice
The psychosocial consequences during AYAC survivorship are widely documented.12,35,36 This study shows that the disruption caused by the pandemic compounded these consequences and were detrimental to AYACs' mental health as they transitioned from active treatment into the survivorship phase. HCPs must advocate for effective psychosocial assessments to ensure individual needs can be identified and supported. Should care be disrupted again in the future, this study has identified the merit in protecting specialized services to enable them to offer their support and maintain contact with young people.
To further support AYACs during health care interactions, HCPs should assess their ability to understand and retain information, particularly in cases where a supporting third party is not present. HCPs may consider other forms of information sharing to supplement traditional verbal methods as well as remaining cognizant of both the benefits and limitations of telecommunications. HCPs may also try to empower AYACs to share and communicate important and difficult information with their families, meeting a critical aim of AYAC care: to support the AYAC to take responsibility for their care.
Strengths and limitations
Despite the small sample size recruited from a single UK center, individual interview duration enabled detailed and in-depth exploration of experiences. Our sample represented both males and females, across a range of AYAC cancer diagnoses and treatment protocols. Furthermore, participants were treated at different times during the pandemic and across the cancer trajectory, which ensures the results are representative of a broad range of experiences. However, the sample for this study did not encompass the younger ages of the AYAC group and therefore this skew toward the middle and older AYACs should be considered when interpreting our results. The study was conducted in the UK health care system, which we recognize may not be similar to other health care systems, which will impact generalizability of our findings.
The use of purposive sampling risked introducing self-selection bias, although it remains unclear if those positively or negatively affected by the pandemic were more likely to volunteer. Our results show concordance with previous studies, which would suggest that bias is limited.
The choice of qualitative techniques and thematic analysis allowed for in-depth analysis of our data. To avoid experiential bias, all researchers were involved in analysis.
Conclusion
The COVID-19 pandemic had widespread effects on health care across the UK. This study has shown that the pandemic affected the experiences of diagnosis, treatment, and long-term follow-up of AYACs. Existing vulnerabilities of the AYAC group were amplified during the pandemic. Longer term effects are critical to understand and study, since complex, compounding effects are not yet understood. HCPs who work with AYAC treated during the pandemic should seek to understand the additional needs of these young people.
Footnotes
Acknowledgments
The authors are grateful to the TYAC service at CUH for assistance with recruitment and, most importantly, thank the patients who participated.
Authors' Contributions
A.H., D.C., H.H., and C.M.: Conceptualization, methodology, validation, formal analysis, and writing—review and editing; A.H.: investigation, data curation, writing—original draft, and project administration; C.M.: writing—figures, and visualization; A.H. and H.H.: funding acquisition; and D.C. and H.H.: supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors would like to acknowledge the University of Cambridge Student Selected Component fund for financially supporting this project.