
Abstract
Purpose:
This study aimed to explore the experiences of young adult cancer patients within the Tunisian context.
Methods:
A total of 104 patients between the ages of 20 and 40, undergoing treatment for various types and stages of cancer, participated in a questionnaire-based survey. The survey encompassed topics related to the socioeconomic and psychological impacts of cancer, coping mechanisms, relationships, sexuality, and future aspirations.
Results:
Of the participants, 78 were women (75%) and 26 were men (25%), with an average age of 33 years. Financial difficulties were reported by 60 patients (57.7%). The most common emotional responses to the diagnosis were sadness (54.8%), followed by denial (18.3%) and anger (5.8%). Thirteen patients (12.5%) choose not to receive information about the stage of their disease. In addition, 42 patients (40.4%) experienced a decrease in perceived physical attractiveness, while negative effects on sexuality were observed in 44.2% of cases. The primary concerns reported by patients were the fear of recurrence or progression (48%) and infertility (48%). Furthermore, 43 patients (41.3%) expressed a decrease in self-confidence, notably influenced by financial difficulties (OR: 2.77 [95% CI: 1.12–6.87]), physical alterations (OR: 0.18 [95% CI: 0.07–0.45]), and sexual issues (OR: 0.17 [95% CI: 0.06–0.48]). Notably, 78 patients (75%) continued to make future plans, particularly those under 30 years of age (OR: 0.2 [95% CI: 0.04–0.96]). Moreover, 47.1% of patients expressed an inclination toward immigration to developed countries, primarily due to perceived superior health care systems (61.5%).
Conclusions:
Young cancer patients face a range of social and psychological challenges, suggesting the necessity for a specialized care approach.
Introduction
Approximately 3
A recent American study reported that psychological challenges, including coping and depression, as well as interpersonal topics, including community support and nonfamily relationships, were the most prevalent psychosocial concerns for YAs. 2 A Moroccan study, with a population culturally close to Tunisians, showed that all patients worried about fertility and sexuality. 3
The main objective of the present study was to investigate the experiences, challenges, and perspectives of YA cancer patients in the Tunisian context. The study aimed to provide insights into various aspects of their lives, including the socioeconomic and psychological impacts of cancer, coping strategies, relationships, sexuality, and future plans. By gathering this information, the study seeks to highlight the specific needs and vulnerabilities of YA patients and potentially contribute to the development of a dedicated care pathway tailored to their unique circumstances.
Methods
We conducted a cross-sectional survey using an anonymous self-administered questionnaire delivered to patients aged 20–40 years who were receiving treatment for cancer, regardless of type and stage, in a medical oncology department in Tunis, Tunisia over a three-month period from February 1, 2022, to May 30, 2022. Study participants provided informed written consent to participate.
Inclusion criteria encompassed patients aged 20–40 years undergoing treatment for cancer, irrespective of gender, disease type, and stage, and whether they were under active treatment or in follow-up. Participants needed to be able to read/understand Arabic and/or French and without impaired cognitive function.
Questionnaire development
To our knowledge, there is no published valid tool suitable for our study's objectives. Based on a literature review, the authors developed a bilingual (Arabic, French) questionnaire consisting of six parts:
Demographic and socioeconomic features of patients (age, gender, primary site and stage of cancer, educational level, job and marital status, number of children). Patients were asked to report any financial difficulties, job loss, or difficulty finding employment. Relationships with partners, children, family, friends, colleagues, and caregivers. Patients were asked to report any changes in their relationships after the cancer diagnosis. Habit modifications (tobacco, alcohol, specific diet, alternative medicine), religious practices (prayer), and coping strategies (sports, art clubs). Psychological impact of cancer: “What was your reaction to the diagnosis announcement?” “Have there been changes in self-esteem, self-confidence, or body image, or physical modifications?” “Is there a need to consult a psychiatrist?” “Is there an impact on sexuality or fear of infertility?” Communications about cancer: “Do you seek information about your disease?” “Have you shared your experience with other patients in the day hospital or waiting room, in a support group, or via the internet (social media)?” Future plans (engagement, having children, career, investments) and immigration plans. Finally, patients were asked to respond to “What is your biggest fear?” and “What are your dreams?”
Data analysis
Descriptive statistics (frequencies, percentages) were calculated, and a chi-square test was conducted for comparisons. Multinomial logistic regression analysis was used to assess odds ratios. A two-tailed p-value <0.05 was considered statistically significant.
Ethics committee approval
We obtained approval from the hospital local ethics institutional review board. We informed patients about the questionnaire and the study's aim and obtained their consent to participate.
Results
A total of 104 patients participated in the survey. Patient's characteristics are summarized in Table 1.
Patient Characteristics
Socioeconomic impact
Socioeconomic impact of cancer on YAs is summarized in Table 2.
Socioeconomic Impact
Relationships
Twenty-three patients (22.1%) reported negative partner reactions: separation (12.5%), indifference (6.7%), and pitiful attitude (2.9%). Among patients with children, 87.9% were able to care for them, and 22.1% disclosed the diagnosis to their children. Ninety-four patients (90.3%) received support from their families (parents and siblings); however, 10 (9.7%) patients reported an indifferent attitude. Fourteen patients (13.4%) were abandoned by their close friends.
Opinions on health care
Seventy-nine (75.9%) patients reported a helpful attitude from the medical and paramedical staff. In contrast, young adults made requests to improve health care, summarized in Figure 1.
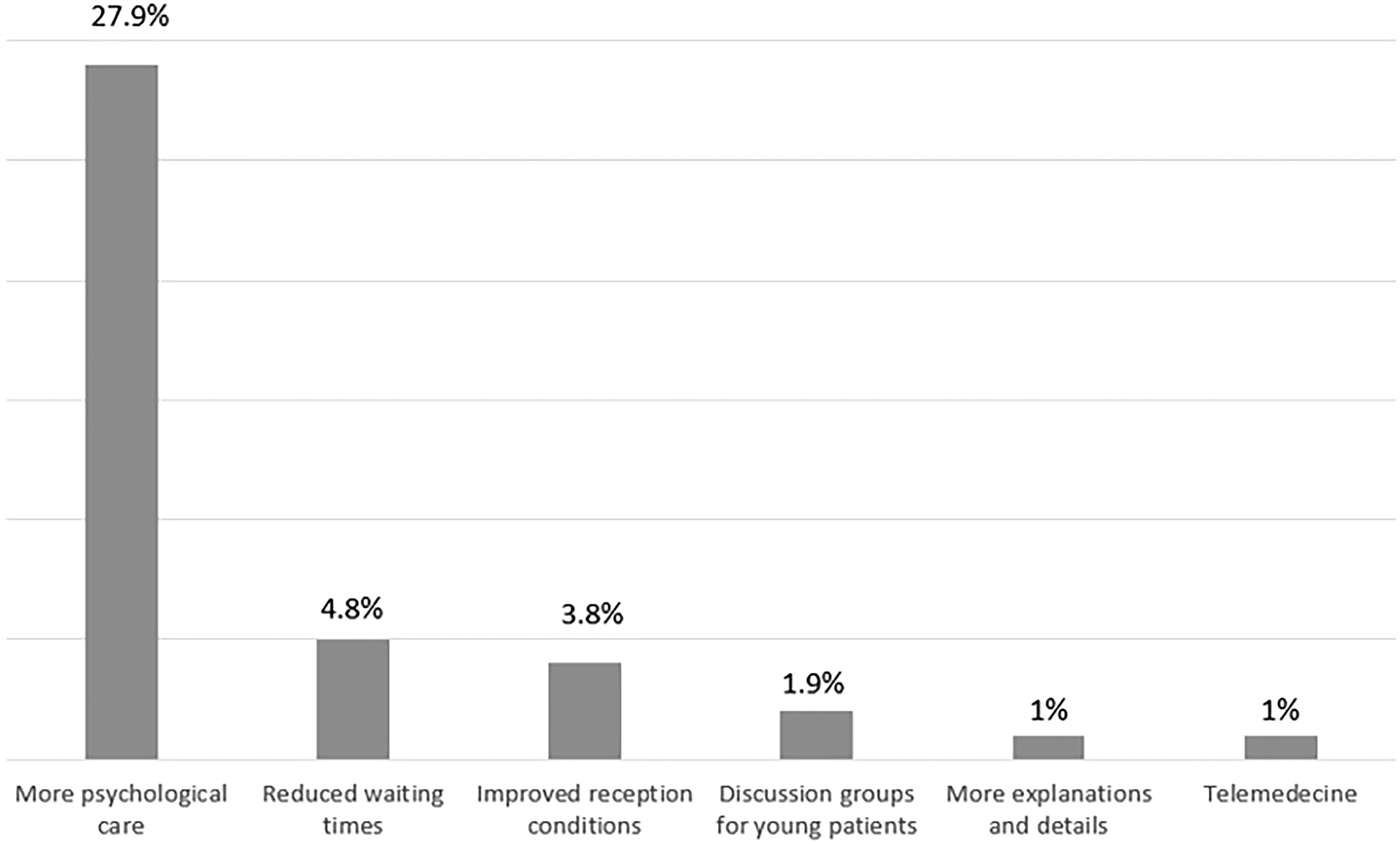
Requests for health care improvement.
Habit modification and coping strategies
YAs presented habit modification after diagnosis and coping strategies to face cancer, summarized in Table 3.
Habit Modification and Coping Strategies
Psychological impact
Sadness (54.9%) was the most frequent reaction to the disease announcement, followed by denial (22.1%), acceptance (16.3%), and anger (6.7%). Sixty-one patients (58.7%) asked “Why me, God?” Forty-two patients (40.4%) felt less physically attractive. Physical changes were primarily caused by alopecia, weight loss, mastectomy, and skin hyperpigmentation, accounting for 23%, 8.6%, 6.7%, and 4.8%, respectively. Negative impact on sexuality was noted in 44.2% of cases. Forty-three patients (41.3%) reported reduced self-confidence, which was significantly impacted by financial difficulties (OR: 2.77 [95% CI: 1.12–6.87]), physical changes (OR: 0.18 [95% CI: 0.07–0.45]), and negative impact on sexuality (OR: 0.17 [95% CI: 0.06–0.48]). Ideas of treatment discontinuation were reported by 32.7%. Twelve patients (11.5%) consulted a psychiatrist. We explored the relationship between psychological impact and time between diagnosis and the survey and found that reduced self confidence was more observed when interval time was <2 years (OR: O.34 [95% CI: 0.11–0.99]).
Communication
Eight patients (7.7%) refused to be informed about their disease stage by their doctors. However, 82 (78.8%) attempted to learn more about prognosis and treatment. Sixty-nine patients (66.3%) used the internet for more information, and 3 patients (2.8%) received assistance from patient associations and books. Thirteen patients (12.5%) shared their experiences in private social media groups. However, 34 patients (32.7%) declined to exchange experiences with other patients, mostly due to a desire to forget their disease (10.5%) and negative and stressful vibes (4.8%). Among YAs, 63 patients (60.6%) preferred not to share the same waiting room or day hospital with elderly patients due to pitiful comments.
Future plans
Seventy-eight patients (75%) continued to make future plans, primarily those under 30 (OR: 0.2 [95% CI: 0.04–0.96]). Immigration intentions to developed countries were reported by 47.1% of patients, mostly due to better health care systems (61.5%). The most commonly reported fears and dreams of patients are summarized in Table 4.
Fears and Dreams of Patients
Discussion
The present study investigated the psychological impact of cancer and the most patient concerns. It found that about 40% of YAs expressed a decrease in self-confidence, notably influenced by financial difficulties, physical alterations, and sexuality. Infertility in addition to fear of progression were the primary patient concerns.
YA cancer patients and diagnosis delay was commonly observed in our study. The median time to diagnosis was 3 months, and the diagnosis was made after 6 months from symptom onset in 17% of cases. These results could be attributed to an uncommon perception of illness among young people. Miedema et al. reported that 75% of YAs experienced some delay in the diagnosis process, often due to either patients' or physicians' inaction. Physicians sometimes perceived patients as too young to have cancer, while patients attributed initial symptoms to their lifestyle choices. 4 More efforts should be made in Tunisia (through radios, TV, social media, etc.) to raise awareness among the YA population about healthy lifestyles and the symptoms of the most common cancers in Tunisia.
YAs often face fragile economic situations, as they are either still studying, seeking employment, or have recently started their professional careers. Corrigan et al. reported in a study (N = 311, 9.6% of YAs, 18–39 years old) that 50% of YAs experienced severe overall financial toxicity, compared to 40.7% of other working-age adults (40–64 years old) and 9.6% of older adults (≥65 years old) (p < 0.001). 5 Similar to the literature, in our study, more than half of YAs reported financial difficulties, consequently depending on their families. Financial difficulties, in addition to complicating economic cancer care management, also negatively impacted the self-confidence of YAs in our study. Similarly, a study of 142 YA survivors showed that worse financial toxicity was associated with lower insurance satisfaction, higher levels of depressive and anxiety symptoms, and greater worry. 6 Economic and psychological interventions should be considered by medical staff and health and social authorities in Tunisia to assist this vulnerable population in facing cancer.
In our study, the most important sources of social support were families and friends, followed by partners. One-fifth of our patients reported a negative attitude from their partners, which could potentially alter their cancer experience. In a Norwegian study, the patients' major sources of private social network support were their partners and close family members. Few friends provided support during cancer treatment, and most lacked peer support. 7 Sources of support can vary between cultures and countries, but parents and siblings seem to be a common source of support universally. Cancer care strategies in Tunisia should support and accompany patients' families to indirectly improve YAs' experiences.
Cancer brings about enduring changes in the way young adults (YAs) live their lives and how they adapt to these changes. Patients predominantly opt to continue planning for the future, adopt a healthier diet, engage in physical exercise, strengthen their spiritual connections through prayer and Quranic readings, and, to a lesser extent, pursue hobbies. In a Palestinian study, different coping strategies were used. Religion and acceptance of the cancer diagnosis were the most frequently used, followed by seeking emotional support, active coping, and making plans. The least utilized strategies were behavioral disengagement, self-blame, and substance use. 8 This underscores the importance of providing sensitization and antismoking consultations, especially for the third of smokers who increased their consumption after their cancer diagnosis. Similar to our population, a Swedish study also identified physical exercise as a crucial coping mechanism. 9 In addition, a Canadian study found that engaging in physical activity contributed to an improved body image among young adult patients. 10
Coping strategies vary from country to country and from one culture to another. However, maintaining a positive attitude appears to be a universal approach adopted by YAs in facing cancer. In more conservative societies, religion often serves as a coping strategy. Providing psychological and social support is crucial in enabling YAs to develop positive and personalized coping mechanisms.
Physicians should encourage more and more YAs to engage in physical exercise. Authorities should facilitate access to coaches, spaces, and equipment for YAs. In a Dutch study, YAs exhibited very positive coping strategies, including minimizing the impact of cancer, taking control, maintaining a positive outlook, embracing the present moment, and being consciously present. 11 In a Japanese study, effective coping strategies included gaining knowledge about cancer, adopting a positive life attitude, believing in one's own resources, faith in a higher power, and drawing from earlier life experiences. 12
Three-quarters of our patients, particularly those under 30 years old, continue to plan for the future. Having plans can be instrumental in helping YAs face their cancer. This approach was also identified by Australian patients to cope. 13
The role of internet and social media in communication
Our patients found the internet to be a valuable tool for accessing information about their disease, including treatments and potential side effects, as well as for sharing experiences with fellow patients. This aligns with findings reported by Seale et al., who noted that patients use the internet to support one another. YAs emphasized that online communities allowed them to connect with other young adult cancer survivors worldwide, considering them as “brothers and sisters” and “friends for life.” They referred to this collective as their “cancer community.” This sense of belonging provided meaning to their lives. 14 However, relying on social media for peer support can be emotionally charged, particularly when encountering demoralizing content. It may also raise privacy concerns, particularly in the context of navigating stigma associated with cancer. 15
In our study, a third of patients were hesitant to share their experiences with others, primarily due to a desire to move past their illness and concerns about encountering negative and stressful content. YAs reported that online community Web sites enabled them to meet other young adult cancer survivors around the world considering them as “brother and sisters”’ and “friends for life.” They used the term « cancer community » to identify their peers. YAs needed to develop a sense of belonging to a group or community which gave their lives meaning. Using social media, especially in today's digital age, can assist YAs in accepting and navigating their cancer experience.
Nonetheless, it comes with a double-edged sword, as it can also disseminate negative sentiments and misinformation. There is a need to develop personalized social media platforms and apps, with oversight from both medical and social science professionals. Nevertheless, using social media for peer support can be an emotional charge, especially when others post demoralizing or vexing content, and can enhance privacy concerns, especially when navigating cancer-related stigma. In our study third of patients refused to exchange experiences with other patients because mostly of desire to forget their disease and stressful vibes. 16
Psychological care and impact
While demands for logistical improvements (such as reducing waiting times and enhancing reception conditions) did not surpass 5%, one-third of our YAs expressed a need for more psychological care, underscoring their vulnerable situation. In an American study, YAs reported feeling at times that health care providers treated them with minimal regard for their rights, spoke in a patronizing manner, and overlooked their requests. 17
Emotional responses to cancer diagnosis
YAs facing a recent cancer diagnosis predominantly experienced sadness, denial, and anger toward a higher power, followed by eventual acceptance. Similar emotional responses were expressed by Iranian patients study. 18
Body image concerns
Slightly less than half of our patients reported experiencing body image concerns, which significantly affected their self-esteem and confidence. The SURVAYA Study (N = 3735) reported negative body image in 14.5% of YAs, a figure lower than our data. 19 Body image appears to play a significant role in the identity of individuals at a young age. In our study, factors like alopecia, weight loss, mastectomy, and skin hyperpigmentation were particularly influential in altering body image. Kim et al. also noted the challenging experiences of patients in dealing with remaining sparse hair and selecting clothing to address asymmetrical breasts. 15
Adapted and personalized psychological support
Specialized and tailored psychological consultations, including considerations for the number, frequency, and tools, should be incorporated into the care plan for YAs. These consultations are crucial at the time of diagnosis, throughout the treatment process, and following remission. They play a vital role in aiding individuals in coming to terms with their transformed self-perception. In addition, patients should be guided, as necessary, to specialists in reconstructive surgery, personalized nutritional guidance, and esthetic recommendations for hair and skin care, recognizing the significant importance of self-image for YA patients.
Sexuality and self-confidence
A negative impact on sexuality was reported by slightly less than half of our patients, which also correlated with a decrease in self-confidence. 20 Similarly, an American study found that over half of the patients experienced challenges with sexual functioning. Jäkel et al. reported that, in a study involving 139 YAs, participants expressed less satisfaction with their sexual health compared to their family life and partnerships. 21 This could potentially be attributed to a lack of open communication surrounding sexuality within the professional, patient, and societal realms. Dutch patients articulated specific needs related to sexual health, including practical and emotional support (e.g., coping with physical side effects), informational requirements (e.g., more detailed explanations), and communication needs (e.g., providers should initiate conversations, validate concerns, and be empathetic and open). 22
Health care providers should proactively inform patients about the potential sexual side effects of treatments and maintain regular discussions about sexual health during the course of cancer care, extending even after remission. Consulting with a sexologist should be an available option when necessary. It is imperative that sexuality is no longer considered a taboo subject within the Tunisian and Arabic-Islamic contexts.
Common fears among YA patients
The most prevalent fears among YA patients encompassed concerns of recurrence or progression, infertility, separation from their children, and a loss of autonomy. Our data closely paralleled findings from Iranian studies. 16 Furthermore, YAs expressed apprehensions regarding the financial implications, including the expenses associated with cancer care and childcare. Half of our patients indicated a desire to immigrate to developed countries, primarily due to the perceived advantages of a superior health care system.
Preserving fertility and providing reassurance
Fertility preservation should be routinely recommended and diligently implemented for YAs. Health care providers should consistently offer reassurance to patients. In addition, authorities should proactively identify financial hardships and furnish economic support.
Addressing the unique needs of young adult cancer patients
YA cancer patients form a particularly vulnerable demographic due to their distinct beliefs, needs, and expectations. Our study sheds light on the experiences of YA cancer patients within the specific Tunisian context, an economically diverse, North African, Arabic-speaking country with a predominantly Muslim population.
Study limitations and conclusions
It is important to acknowledge the limitations of our study. It was conducted at a single center and predominantly included patients from the northern and western regions of Tunisia, potentially limiting its generalizability to YAs from other parts of the country who may have distinct experiences with cancer. In addition, the majority of our patients were female and diagnosed with breast cancer, potentially introducing a selection bias. In one hand it is representative of the YA cancer population, in which breast cancer is predominant; on the other hand it did not allow a precise comparison between man and women considering the low number of men in the present study.
In conclusion, YA cancer patients confront a range of social and psychological challenges, from financial difficulties to communication barriers and negative partner dynamics. These individuals require a dedicated care pathway that encompasses psychological support, economic aid, and social guidance.
Footnotes
Authors' Contributions
Y.B.: Conceptualization, Formal analysis, Investigation, Writing—original draft, Methodology. H.R.: Data curation, Formal analysis, Investigation, Writing—original draft. M.S.: Data curation, Investigation. A.A.H.: Validation, Visualization. S.F.: Validation, Visualization. N.D.: Visualization, Validation, Software. N.M.: Writing—review and editing, Supervision. H.B.: Supervision, validation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.