
Abstract
Premature ovarian insufficiency (POI) is one of many potential long-term consequences of childhood cancer treatment in females. Causes of POI in this patient population can include chemotherapy, especially alkylating agents, and radiation therapy. Rarely, ovarian tumors lead to ovarian dysfunction. POI can manifest as delayed pubertal development, irregular menses or amenorrhea, and infertility. This diagnosis often negatively impacts emotional health due to the implications of impaired ovarian function after already enduring treatment for a primary malignancy. The emerging adult may be challenged by the impact on energy level, quality of life, and fertility potential. POI can also lead to low bone density and compromised skeletal strength. This review discusses the health consequences of POI in childhood cancer survivors (CCS). We also explore the role of fertility preservation for CCS, including ovarian tissue cryopreservation and other available options. Lastly, knowledge gaps are identified that will drive a future research agenda.
Introduction
Using current estimates, with the majority of morbidity and mortality data available from studies conducted in the United States and Europe, there are >500,000 childhood cancer survivors (CCS) who live in the United States.1–3 With improved treatment strategies, over 85% of children affected by cancer are currently cured. 4 However, these treatments often have long-term health consequences. Ongoing cohort studies of CCS reveal treatment-related morbidities and early mortality as these patients age and more data are needed that provide a broader international perspective.3,5–7 One late effect involves ovarian function. Clinical features associated with ovarian dysfunction include delayed or absent pubertal development, hypogonadal effects postpuberty such as premature ovarian insufficiency (POI), and infertility.8–12
POI is a significant source of treatment-related morbidity and concern for female CCS. The prevalence of POI among this group varies by report and is estimated at 8%–31%, while that among the general population is only 1%.13–16 The St. Jude's Hospital Lifetime Cohort reported the prevalence of POI to be 10.9% in their cohort of 921 women evaluated at a median of 24 years after cancer diagnosis. 9
The likelihood of developing ovarian dysfunction after childhood cancer is dependent on tumor location, the curative treatments employed, and age at treatment. While tumors occurring in the ovary, radiation to the pelvis, or exposure to certain chemotherapies can directly impact ovarian reserve and function, tumors of the central nervous system and their treatment can also disrupt the hypothalamic–pituitary–ovarian (HPO) axis. Tumors in the sellar/suprasellar region or cranial radiation can lead to central hypogonadism, which is associated with delayed or interrupted pubertal development due to low luteinizing hormone (LH) and follicle-stimulating hormone (FSH) concentrations. Furthermore, specifically for ovarian tumors, the amount of ovarian tissue removed (>1 ovary) may also impact ovarian reserve and function. However, this topic is beyond the scope of this review; hence, the reader is referred elsewhere. 17
Ovarian Development
The bipotential gonad develops from the adrenogonadal primordium at ∼28 days postconception. Subsequently, sex determination occurs primarily depending on the presence or absence of the SRY gene. In the absence of SRY, a complex, sequentially orchestrated developmental pathway unfolds, leading to ovarian differentiation. 18 For ovarian development, individual oocytes become enveloped by somatic cells to form follicles. Typically, these primordial follicles (PMFs) are located at the edge of the ovarian cortex in a region with limited vasculature. 11
At birth, ovaries contain ∼1–2 million PMFs with only about 400,000 remaining at pubertal onset. 19 Although most follicles remain arrested at the diplotene stage of meiosis I, a few PMFs are activated during childhood. Subsequently, with the onset of increased hypothalamic–pituitary activity at puberty, PMFs are activated until follicular depletion develops, which is signaled by elevated FSH during menopause. PMF activation is characterized by proliferation of surrounding granulosa cells and growth of the oocyte.
The initial phases of follicular maturation from the PMF until the preantral stage are gonadotropin independent. However, during the transition from the secondary follicle to the antral stage, FSH dependence develops. Anti-Müllerian hormone (AMH), a glycoprotein secreted by granulosa cells, interferes with follicular recruitment, acting as a “gatekeeper” for follicular maturation. With cyclic gonadotropin stimulation, small cohorts of antral follicles are sequentially recruited, ultimately leading to selection of a single dominant follicle for ovulation. 20
Puberty
Puberty is the process during which the prepubertal girl develops reproductive competence. In girls, increased gonadotropin-releasing hormone (GnRH) and gonadotropin secretion leads to increased ovarian estrogen secretion. Breast development is the initial physical pubertal sign with menarche signifying its completion. Systemic review with meta-analyses indicated that the median age for onset of breast development (Tanner Stage II) in the United States ranged from 8.8 to 10.3 years. 21 Usually, menarche occurs 2–2.5 years after the onset of breast development.
Pubic hair development is often considered as a physical manifestation of puberty. However, development of apocrine odor, pubic and axillary hair, and acne represent adrenal pubertal maturation with increased secretion of androgenic steroids from the zona reticularis. Adrenal function is regulated by the hypothalamic–pituitary–adrenal axis, which is largely independent of ovarian function.
Premature Ovarian Insufficiency
POI, previously referred to as “premature ovarian failure” or “premature menopause,” is a clinical syndrome defined by the loss of ovarian activity in women <40 years.22–24 POI is characterized by amenorrhea for at least 4 consecutive months, and elevated FSH concentrations on at least two occasions, with measurements obtained at least 1-month apart.25–27 Symptoms may vary depending on the age of affected individual or severity of ovarian dysfunction. When POI occurs in adolescence, symptoms can include delayed or arrested pubertal development, amenorrhea, or signs of postpubertal hormonal deficits. 28 POI also directly and deleteriously impacts fertility. A consequence of impaired ovarian function is hypoestrogenism, which has long-term consequences on quality of life, psychosocial well-being, bone health, cardiovascular risk, vasomotor symptoms, sleep disturbances, and neurological function.3,29,30
Clinical presentation
As mentioned, adolescent girls with POI often present with pubertal delay, irregular menses, and/or symptoms reflecting estrogen and other hormonal deficiencies.22,24,28 Among adults, the clinical presentation broadens to include infertility. Importantly, the clinical presentation of POI varies. Some adolescents present with few symptoms, which heightens the diagnosis-associated surprise and shock. The waxing and waning of ovarian hormones may also result in fluctuating symptoms.
Elevated FSH concentrations, indicative of follicular depletion, and eventually a subnormal estradiol concentration, are required for the diagnosis of POI. Increased LH and low AMH concentrations may also be found. As noted, two elevated FSH concentrations (obtained >1 month apart) are requisite for the diagnosis and a common threshold for the elevation is 40 IU/L.22,31 However, the National Institute for Health and Care Excellence recommends 30 IU/L as an upper limit 32 and the European Society of Human Reproduction and Embryology, 25 IU/L. 33
Etiology and differential diagnosis
POI is a heterogeneous disorder characterized by depletion of ovarian follicles and subsequent hormonal dysregulation. For female CCS, iatrogenic factors are the most common cause of POI. Among CCS, POI has been associated with specific therapeutic exposures that are gonadotoxic and/or disrupt the HPO axis. Female survivors who have received hypothalamic, abdominal, or pelvic radiation involving the ovaries and/or gonadotoxic antineoplastic therapies are at the highest risk for POI (Table 1).9,34 Evidence-based recommendations regarding long-term follow-up care of CCS are available—the Children's Oncology Group “Long-term Follow-up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers.” 35
Indications for Hormone Replacement Therapy in Adolescent Girls
BMD, bone mineral density; CCS, childhood cancer survivor; COC, combined oral contraceptive; HRT, hormone replacement therapy.
Treatment-Related Risk Assessment
Chemotherapy
Chemotherapy can affect ovarian follicles and negatively impact ovarian vasculature and stroma (Fig. 1). 11 The direct and indirect consequences of these agents may depend on the stage of follicle maturation. Chemotherapeutic agents associated with gonadotoxicity are reviewed in this study (Table 2).

Mechanisms of ovarian injury due to chemotherapy, including effects of therapy on PMFs (borrowed with permission, Spears et al. 11 ). Depicted are the mechanisms of ovarian damage due to chemotherapy drugs. Chemotherapy may cause ovarian damage by inducing prenatal loss of oogonia, direct loss of PMFs, accelerated PMF activation, follicular atresia, stromal tissue damage, injury to the vasculature, or inflammation. PMFs, primordial follicles.
Gonadotoxic Chemotherapeutic Agents
BCNU, carmustine; CCNU, lomustine.
Alkylators
Alkylators are typically considered to be the most gonadotoxic chemotherapy class. These agents damage DNA by the addition of alkyl groups or DNA crosslinking, impairing transcription, protein synthesis, and further cell division.36,37 These actions can induce apoptosis of primary follicles. 38 Examples include bulsulfan, carmustine (BCNU), chlorambucil, cyclophosphamide, ifosfamide, lomustine (CCNU), mechlorethamine (nitrogen mustard), melphalan, procarbazine, and thiotepa. Each agent has variable gonadal toxicity (per cumulative milligram per meter squared administered). The cyclophosphamide equivalent dose (CED) is used to standardize cumulative alkylating agent exposures from the above agents for individualized risk assessment. 34 Dacarbazine and temozolomide are alkylating agents but are not included in the CED calculation.
The risk of developing POI increases with increasing alkylator dose exposure. 39 Even with low exposure, POI can occur years to decades after receipt of chemotherapy.10,40 However, POI is more common among female CCS receiving ≥8000 mg/m2 of CED.9,34 Comparison of survivors exposed to alkylating chemotherapy before and after puberty suggest that the postpubertal ovary is more sensitive to alkylators, with toxic effects seen at lower cumulative dose exposure than prepubertal ovaries. 37
Heavy metals
Cisplatin and carboplatin contain platinum, which results in DNA crosslinking, leading to inhibition of DNA duplication and consequent cell death. Similar to alkylating agents, heavy metals have been shown to be gonadotoxic. 41 Gonadotoxicity has been most consistently demonstrated in male CCS; however, exposure to platinum chemotherapies is still regarded as potentially toxic for females and is considered a risk factor for POI in the context of fertility preservation and survivorship surveillance and counseling. 42
Radiation therapy
Radiation is a significant treatment-related risk factor for ovarian dysfunction.
Cranial radiation
As mentioned, disruption of the HPO axis by radiation exposure of the hypothalamic and pituitary regions can cause ovarian dysfunction by central hormonal dysregulation. Detailed reviews can be found elsewhere. 43
Ovarian tissue radiation
POI is strongly associated with ovarian radiation. 9 Ovaries sustain radiation exposure in broad fields such as pelvic, spinal (sacral or whole), or total body irradiation. The degree of risk for ovarian damage/dysfunction is related to radiation dose, radiation therapy type, whether ovarian shielding or oophoropexy was performed before radiotherapy, and age at treatment, recognizing that the oocyte is extremely sensitive to radiation. It is estimated that <2 Gy can destroy 50% of PMFs, and the ovary appears to become increasingly sensitive to damage from radiation with increasing age. 40 Additionally, radiation exposure to the gonads combined with higher cumulative doses of alkylator chemotherapy may further increase risk of POI. 9
Hematopoietic stem cell transplantation
Hematopoietic stem cell transplantation (HSCT) has been associated with POI incidence ranging from 44% to 100%, varying by clinical, treatment, and demographic variables.44,45 Conditioning regimens, which include high doses of alkylating chemotherapies, such as busulfan and cyclophosphamide46,47 and/or total body irradiation,44,45 have been associated with the most significant impact on ovarian function after treatment. Similarly, undergoing HSCT at an older age increases risk for the development of POI. 48 The association of POI with HSCT reflects a summation of treatment intensity, radiation exposure, and utility of transplantation in relapsed and refractory diseases where treatment before transplantation must be considered. A tool has been developed by the Oncofertility Consortium that considers treatment exposures (e.g., alkylating agents, platinum agents, HSCT, etc.) and provides relative risk categories for the development of reproductive compromise (Fig. 2). 49 This resource can be helpful for counseling patients.
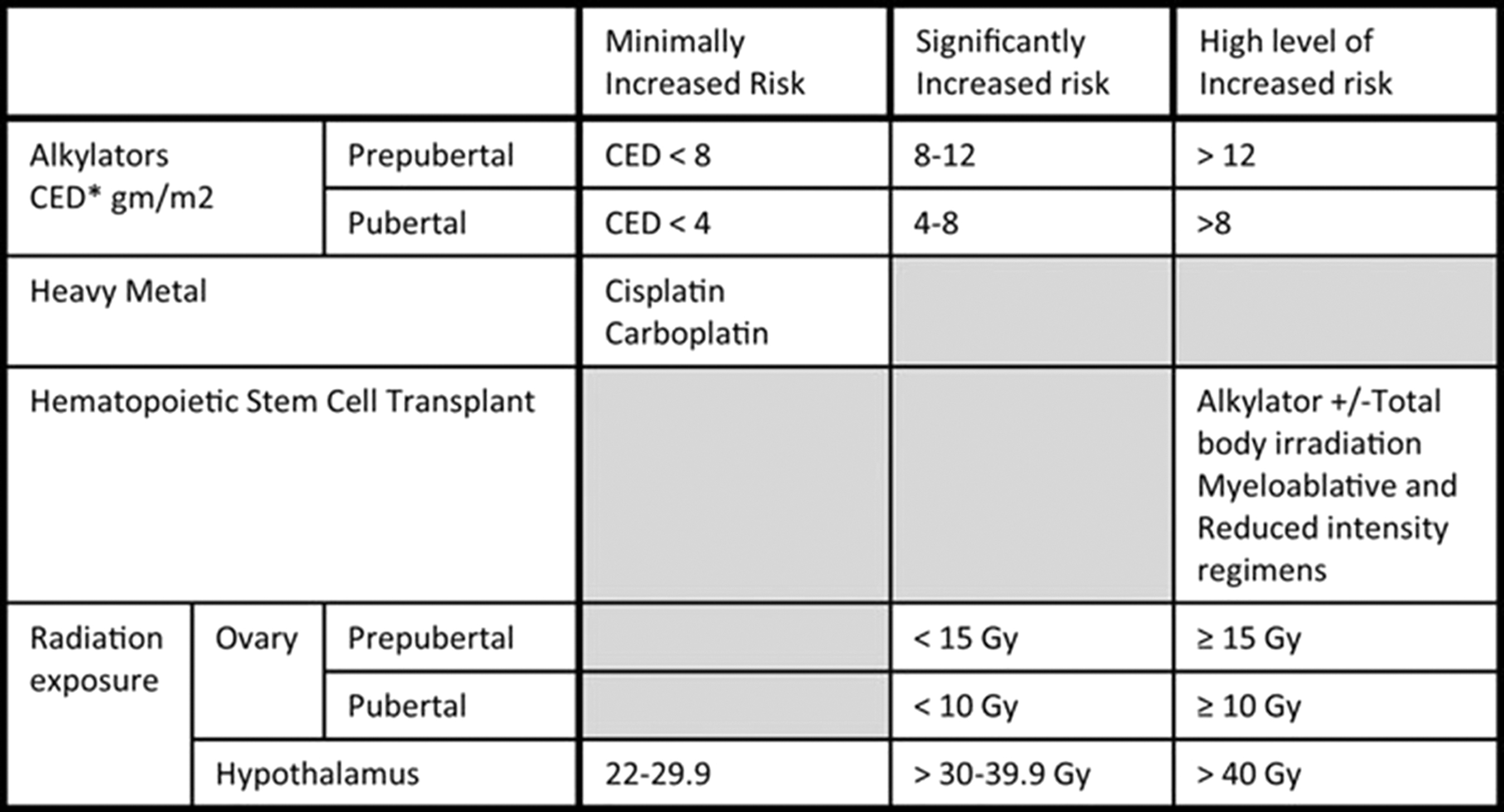
Level of risk for gonadal failure/infertility in females above that for the general population with respect to treatment-related factors (borrowed with permission). 45
Ovarian tumors
Ovarian tumors are rare in children and often affect ovarian function. Granulosa cell tumors may secrete estrogen. Sertoli–Leydig cell tumors may be associated with DICER1 genetic variants; individuals with DICER1 variants have increased risks to develop neoplastic changes and hamartomatous lesions in diverse organs at young ages. 50 Ovarian germ cell tumors are associated with gonadal dysgenesis and the presence of Y chromosomal material; karyotypes with fluorescent in situ hybridization (FISH) for the Y chromosome should be performed. 51
Other considerations in the evaluation
Although this review focuses on POI in CCS, exclusion of other causes should be considered. Other etiologies include chromosomal, genetic, metabolic, and toxic factors. Considering genetic versus nongenetic causes can provide a useful framework (Table 1). Chromosomal etiologies of POI include X chromosome monosomy and its mosaic variants associated with hypergonadotropic hypogonadism and streak gonads. 19 The list of genes associated with POI continues to expand. Another example of a genetic cause is galactosemia.
POI can be due to isolated autoimmune oophoritis. However, most women with autoimmune POI have other autoimmune disorders such as Hashimoto's thyroiditis or adrenal insufficiency. 52 In some instances, POI occurs in conjunction with a genetic autoimmune polyglandular disorder (APS), such as APS-1, which is associated with variants in the AIRE gene.53,54
Diagnostic Testing
As mentioned, documentation of two elevated serum FSH and simultaneously measured low estradiol concentrations obtained at least 1 month apart are necessary to diagnose POI. Among cancer survivors, the most likely etiology is treatment of the malignancy or the malignancy itself, especially among girls with ovarian cancer. Nevertheless, additional studies should be considered in specific circumstances. Girls with XY gonadal dysgenesis may present with germ cell tumors such as dysgerminoma. In this situation, chromosomal analysis with FISH to assess for mosaicism and detect Y chromosome elements is essential. Fragile X gene analysis to assess for the premutation status and autoantibody studies to assess for autoimmunity may be helpful for some patients.22,24
Anti-Müllerian Hormone
AMH is produced by granulosa cells of preantral and small antral follicles. The major role of AMH in the ovary is to maintain the follicular reserve by impeding the transition of PMFs to primary follicles. Among healthy girls, serum AMH concentrations during adolescence showed a positive correlation with values obtained in infancy and childhood. 55 Thus, under normal circumstances, AMH concentrations provide an estimate of ovarian follicular reserve. 56
Following gonadotoxic therapeutic interventions, AMH concentrations may decline. The initial fall and inconsistent recovery of AMH appears to vary by treatment regimen. Between cancer diagnosis and the end of treatment, AMH concentrations fell more rapidly in those treated with alkylating agents.57,58 In a pediatric cohort of 22 girls with a range of oncologic diagnoses, AMH concentrations declined progressively after each course of chemotherapy and were eventually undetectable in half of patients. 59 In another series, lower AMH concentrations were associated with higher doses of gonadotoxic therapies and bilateral ovarian irradiation. 60 A systematic review reported that among pediatric patients, AMH concentrations were reduced in 14/20 studies compared with either pretreatment or control values. 29 Low/moderate gonadotoxicity regimens showed recovery with AMH approaching pretreatment concentrations. High-risk regimens (i.e., high doses of alkylating agents or with pelvic radiotherapy) showed persistently low AMH concentrations with little to no recovery. Some cancer survivors have low AMH concentrations despite normal FSH concentrations suggesting partial ovarian insufficiency. 61
In CCS, potential reasons to measure AMH is to identify ovarian damage, identify patients who may need to be followed more closely, and allow consideration of post-treatment oocyte harvest in those not yet diagnosed with POI. Thus, AMH concentrations may be used to assess ovarian reserve and risk for POI in these patients. However, normative reference ranges (compared with age-appropriate peers) for AMH remain poorly defined 62 and may vary by the assay used. In addition, clarity is needed regarding the capability of post-treatment AMH concentrations to predict risk for future development of POI.63,64
Preservation Strategies
Considerations before cancer treatment
Children diagnosed with cancer and their families should be informed of the impact of planned cancer treatment on fertility. For female cancer patients undergoing treatment with alkylating agents,9,65 ovarian radiation,9,65,66 HSCT,65,66–69 cranial radiation,70,71 unilateral oophorectomy,65,72 hematological malignancy treatment, 73 or a combination thereof, counseling on pretreatment fertility preservation options and alternative family planning should be provided. 69 Data from the Childhood Cancer Survivor Study (CCSS) suggest that female cancer survivors who did not undergo radiotherapy have similar rates of pregnancy and live birth to their siblings, except when exposed to busulfan, high-dose CCNU, or high cumulative doses of other alkylating agents. 4 The impact of radiation is dependent on the planned radiation field, dose of fractionated radiotherapy, and age of recipient, with complications rising with increasing doses and older ages at the time of treatment. Receipt of pelvic radiotherapy is associated with the most significant risk of future infertility74,75 and increased risk of pregnancy complications.76–78
A discussion of oocyte, embryo, or ovarian tissue cryopreservation (OTC; as appropriate) should accompany treatment plans that include high doses of alkylating agents, ovarian radiation, or HSCT. Postpubertal females at high risk of cancer recurrence should undergo counseling on oocyte or embryo cryopreservation, as well. Female fertility preservation techniques require time to plan and execute, which may not always be feasible. When cancer treatment is urgent, the implications of treatment delays must be considered in determining whether pretreatment fertility preservation is possible.
Rarely, ovarian infiltration with tumor has been described in girls with lymphoma or leukemia.79,80 Importantly, the potential to reintroduce malignant cells from cryopreserved ovarian tissue needs to be considered. Available data regarding the risk for reintroduction of malignancy through reimplantation of cryopreserved ovarian tissues is limited emphasizing the need for prospective long-term follow-up of such patients.81,82
In addition to pretreatment oocyte or ovarian tissue harvest, oophoropexy and use of GnRH analogs for ovarian suppression have been used during therapy, although the efficacy of these interventions is controversial.76,83,84
Fertility preservation
The loss of fertility in patients with POI can be devastating for adolescents and their families. Thus, consideration of options for fertility preservation is crucial. Oocyte cryopreservation is an established method of fertility preservation,85,86 but requires a postpubertal ovary and an indication of adequate ovarian reserve (usually encompassing FSH, AMH, and antral follicle count). OTC is used increasingly world-wide, attempting to minimize adverse effects of gonadotoxic cancer therapies and fertility loss associated with iatrogenic POI.85,87 In 2019, the American Society of Reproductive Medicine Committee Opinion on fertility preservation in patients undergoing gonadotoxic therapies stated: “OTC should be considered an established medical procedure and is no longer considered experimental.” 87 However, significant knowledge gaps remain regarding use of OTC in prepubertal children and adolescents, given the sparse available data in this patient population. 88 Oocyte cryopreservation has been successful among girls as young as 12 years of age at risk for POI. 89
The procedure requires laparoscopy to remove tissue and later surgery to replace it, which is not without risk. Surgical expertise and appropriate storage are also required. Therefore, centers with clinical and laboratory expertise are needed.90–92 Standardized infertility risk assessment guidelines provide an opportunity for greater consistency in clinical care and baseline for the launch of future studies to refine risk stratification. 93
Oocyte vitrification
Removal of ovarian tissue and in vitro activation of follicles from a fresh and frozen ovarian cortex are emerging as possible fertility treatments for POI. 94 Even in limited income settings, parents of children with cancer value a multifaceted approach to shared decision making. 95 Although fertility preservation is not yet fully integrated into the comprehensive cancer care of pediatric and adolescent patients, advances continue to take place.96,97
Considerations During Cancer Treatment
GnRH analogs
Based on their role to suppress HPO axis function, GnRH agonists have been utilized to avoid ovarian damage from chemotherapy or radiation. 27 The benefits of this approach in CCS remains to be determined and is therefore controversial, especially regarding fertility outcomes.11,98 Currently, a Cochrane review recommended use of adjuvant GnRH agonist therapy in premenopausal women. 99 However, their use in many circumstances has been replaced by OTC. 100
Potential protectants
There are now multiple agents designed to protect the ovary against cisplatin and other chemotherapy-mediated damage. While not yet tested in pediatrics, these agents prevent the direct loss of PMFs, acceleration of PMF activation, or follicular atresia.83,101,102 Proposed treatments are hypothesized to protect against ovarian damage by reducing ovarian drug delivery and altering pathways that mediate damage other than damage to stromal tissue. 11 Examples include: everolimus, tamoxifen, melatonin, and antioxidants, among many others. However, no published findings are available, and the potential roles of these protectants are still in research phases. Gonadal shielding, oophoropexy, and ovarian transplantation are being explored to minimize exposure of the ovaries to treatment-related damage; further study is needed due to conflicting efficacy data.83,101,102
After Completion of Therapy
Monitoring for POI
After completion of therapy, engagement with survivorship services to address treatment-related health concerns is recommended. Pediatric endocrine consultation may be appropriate to provide ongoing assessment of pubertal development, reproductive history, and provision of fertility counseling. Early detection of POI allows for discussion of post-treatment fertility preservation options and/or timely initiation of hormonal replacement. Regular surveillance for ovarian late effects should be followed using guidance from the Children's Oncology Group. 35 These guidelines may present opportunity to expedite referrals to a pediatric endocrinologist in a timely fashion.
Hormone replacement therapy
Hormone replacement therapy (HRT) offers multiple benefits for adolescents and young women with POI, including: development of secondary sex characteristics or pubertal completion; establishment of menarche or resumption of a regular menstrual cycle; alleviation of vasomotor symptoms (e.g., hot flashes and night sweats); resolution of symptoms affecting quality of life (e.g., mood, cognitive slowing, energy levels, etc.); support for normal sexual function with vaginal lubrication; and creation of an optimal hormonal milieu for implantation and ultimate pregnancy. While sparse clinical trial data are available, proper dosing of HRT should reduce the future risk of osteoporosis and cardiovascular disease. 103
Irrespective of etiology, the goals of HRT are to provide and/or restore a physiological estrogenic hormonal environment to ensure optimal health outcomes, maximizing benefits and minimizing side effects/risks. 24 Ideally, hormone replacement would include preparations identical to 17β-estradiol. Nonoral delivery routes avoid first-pass hepatic metabolism and minimize the prothrombotic effects of oral estrogen. A transdermal 17β-estradiol delivery system also facilitates monitoring stability of estradiol concentrations compared with oral delivery due to more stable pharmacokinetics.
In clinical practice, much variability exists for the management of POI among health centers and even between countries. Data from high-quality clinical trials to guide clinicians on beneficial doses for optimal health and quality-of-life outcomes are limited. Debate continues regarding the most appropriate doses and method of administration for both estrogen and progesterone for peak bone mass, endometrial protection, and other outcomes. There is also more to be learned about patient preferences, which will influence compliance. A patient-based, integrated hormonal approach has been proposed that incorporates data from an international database for patients with POI. 104 This approach could also be developed to focus on adolescents who are female CCS.
For an adolescent with POI who is in mid- to late puberty (Tanner III–V breast development), a typical regimen would consist of 17β-estradiol provided as a 75–100 μg patch, initially starting with a low dose (i.e., 25–50 μg daily). Oral estradiol (2–4 mg/day) is an alternative regimen, which is thought to be safe for a nonobese adolescent. These doses are thought to achieve steady estradiol levels of 200–400 pmol/L. Estrogen dosing is relatively high (compared with that prescribed for women during natural menopause), as a higher dose is needed for symptom relief, as well as bone and cardiovascular benefits (from limited clinical trial data).105–108
Progesterone replacement in an adolescent is typically achieved with 100–200 mg of micronized progesterone orally (or vaginally) for 12 days of the month, allowing for regular withdrawal bleeding. Micronized progesterone is preferred over medroxyprogesterone acetate or other preparations. With micronized progesterone, metabolic benefits of estrogen can be maintained, and thrombotic side effects minimized when combined with transdermal estrogen. 109 Of note, data have been obtained primarily in women undergoing a natural menopause, and more information is needed to confirm findings in adolescents and younger women with POI. Medroxyprogesterone acetate is also a more androgenic androgen and associated more frequently with side effects, as well as mastalgia and premenstrual symptomatology. One study of women suggested that the benefits of estrogen are not significantly attenuated by androgenic progestogens when higher doses of estrogen are used in POI. 110 More research is needed in adolescents.
For the adolescent requiring contraception, if there are problems with sporadic vaginal bleeding, a levonorgestrel intrauterine system (IUS) releasing 20 μg/day can be used in combination with transdermal or oral estrogen. 23
The combined oral contraceptive (COC) pill containing ethinyl estradiol has been used for both pubertal induction and hormone replacement in adolescents with POI. The COC is easily accessible, inexpensive, familiar to both patients and clinicians, and provides contraception, if needed. However, as has been discussed in the context of care for adolescents with Turner syndrome, use of the COC has been driven by practicalities rather than science. 111 Ethinyl estradiol is a potent estrogen with a long hepatic half-life that can increase the risk of thrombosis and hypertension. There are also data suggesting that ethinyl estradiol does not result in optimal breast and uterine development and should be avoided when possible, for pubertal induction. 32 Longitudinal studies reveal that metabolic and bone outcomes make this preparation less beneficial for women with POI.107,112,113 The cyclic regimens (e.g., 21/7 or 24/4 days) may also diminish the benefits of primary prevention outcomes. There are general concerns that the estrogen doses provided in a typical COC are not high enough for adolescents and young women with POI.
The contraceptive ring, however, is another option for continuous provision of estrogen/progestin that merits further study in adolescents.
In closing, it is important to know that HRT typically does not provide contraception. Ovarian function can wax and wane in adolescents and women with POI, and there is an ∼5% chance of a pregnancy. 45 Therefore, contraception should be prescribed if pregnancy is not desired. As reviewed, estrogen (transdermal or oral) with a levonorgestrel IUS or a COC is generally well received by adolescents. It has been suggested that after 2 years of a POI diagnosis, the risk of pregnancy is low, and a patient can be transitioned from a COC to HRT regimen. 24 Lastly, more research is needed to inform counseling to patients on the association of HRT with malignancy (e.g., breast cancer) in those survivors who received chest radiotherapy and/or anthracycline exposure, who appear to already be at increased risk.
Bone health surveillance
A low bone mass for age and skeletal deficits are of high concern among young women with POI.114,115 Both adolescents and adult women with POI have a lower bone mineral density (BMD) and are at increased risk for osteoporosis compared with those experiencing menopause at an appropriate age (odds ratio 2.54; 95% confidence interval 1.63–3.96).116–118 Estrogen deficiency as is seen in POI is associated with increased bone resorption, which can impede bone accrual. 119 The estrogen deficiency associated with POI could compound the impact of glucocorticoids and other medications on diminished osteoblast function and bone formation.120–122 Survivors of HSCT may experience an even higher risk of bone health compromise, as HSCT has been associated with low BMD and the development of POI from glucocorticoids and other therapies. The St. Jude Lifetime Cohort also found POI to be an independent predictor of low BMD. 9 In adolescents who are CCS, a primary concern is the compromise of peak bone mass, which in turn heightens the risk of developing osteoporosis. Thus, surveillance for early-onset osteoporosis is needed in adolescent and young women with POI.114,115
Surveillance and management of bone health in the adolescent or young woman with POI generally include: Dual-energy X-ray absorptiometry (DXA) screening at diagnosis, with follow-up scans every 1–2 years if the initial BMD is low for age; 25-hydroxyvitamin D measurement at least annually; prompt initiation of HRT as estrogen monotherapy initially; and then advancement to combination estrogen/progesterone replacement. For DXA screening, the lumbar spine and whole body (ideally total body less head) would be assessed for the adolescent ≤ age 15 years; for those ≥16 years, hip and spine would be the recommended sites. 123 A low bone mass for age would be defined as a BMD Z-score ≤less than or equal to −2.0 in an adolescent, as this threshold has been associated with an increased fracture risk in pediatrics. 124
Appropriate lifestyle counseling would include meeting daily calcium recommendations (1300 mg elemental daily) and vitamin D (600–1000 IU daily), with consumption through dietary means promoted, whenever possible. However, vitamin D is often most easily provided as an oral supplement given the limited sources within foods (e.g., sardines, mackerel, etc.). Moderate weight-bearing physical activity should be encouraged, as appropriate.23,125
The above general approach, combined with HRT, should lower the risk of osteoporosis, although evidence from clinical trials is currently lacking.
Post-treatment screening
Hypoestrogenism associated with POI can have an impact on bone health surveillance and cardiometabolic health. At diagnosis, a baseline assessment of insulin resistance (e.g., hemoglobin A1c and fasting lipid panel) is warranted. After therapy's completion, annual assessments should be considered, although the frequency should be ultimately determined by results of initial testing and the adolescent's family history and risk profile. 24
Screening for the psychosocial and psychosexual sequelae of POI should also be carried out. 126 Following a diagnosis of POI, high levels of depression and reported stress have been noted, as well as lower self-esteem and life satisfaction.127,128 In a CCS, the risk may be even higher, given the disappointment about this diagnosis following an initial relief after treatment of the primary malignancy. The use of validated screening tools for depression and anxiety can be helpful in addition to information obtained from a clinical interview.
Risks for future offspring
Primordial oocytes may suffer damage during chemotherapy and radiation, leading to potential transmissibility of germline damage to future offspring. However, a large population-based Finnish study found no increase in cancer risk apart from inherited cancer syndromes. 129 Despite differing methodologies and limited numbers of subjects, available data fail to show an increased risk for genetic disorders in the offspring of cancer survivors. 66
Conclusions
POI is a common and life-altering complication of treatment for female CCS. POI not only impacts fertility but has the potential to adversely affect overall physical, mental, and sexual health in an already vulnerable patient. The risk of POI appears to increase with age and can vary depending on disease, treatment, and demographic variables. An active area of research is the identification of fertility preservation measures, including the efficacy of these agents and techniques, and the safety and efficacy of the optimal estrogen replacement regimens for BMD and other aspects of health. Compelling data exist, showing a low bone mass and compromised emotional well-being to be common among adolescents with POI linked in part to hypoestrogenism.
Therefore, data from future estrogen treatment trials will advance the field. Currently, there are sparse longitudinal data that document the risk of fractures at any age or osteoporosis during the adult years among CCS. A future research agenda will also need to include the exploration of agents that protect the ovaries from chemotherapy-induced damage. Loss of fertility can be a devastating consequence of cancer-related therapy, and options for fertility preservation will continue to be an active and important area of research.
Footnotes
Authors' Contributions
K.L.F.: conceptualization, methodology, and writing—original draft. D.J.L.: writing—review and editing, and visualization. S.F.W.: writing—review and editing, and visualization. C.M.G.: conceptualization, methodology, writing—original draft, visualization, and supervision.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
The authors have received no funding for this article.