
Abstract
Adolescent and young adult (AYA) cancer survivors often search online for information about cancer-related sexual and reproductive health concerns. A review of the websites of National Cancer Institute-designated cancer centers (n = 9) and comprehensive cancer centers (n = 58) was conducted to identify the presence of AYA-specific sexual and reproductive health programming and resources. No AYA-specific sexual health programs were found. Oncofertility programs were presented on 56% (n = 5) of cancer centers and 50% (n = 29) of comprehensive cancer center websites. As the population grows, it is imperative that cancer centers provide services to meet AYAs’ sexual and reproductive health needs and highlight these services on their websites.
Introduction
In 2024, there will be >84,000 new cancer diagnoses in the United States among adolescents and young adults (AYAs) aged 15–39. 1 Due to improved cancer screening and treatments, nearly 86% of AYAs will survive 5 or more years after their diagnosis. 1 A growing population of these survivors will face significant long-term effects of their cancer and cancer treatments. Sexual (e.g., difficulty building arousal, low sexual interest, body image concerns) and reproductive (e.g., infertility) health concerns are prevalent and especially burdensome long-term effects experienced by AYAs.2–4
AYAs are in a life stage characterized by exploring sexuality, developing romantic partnerships, and for some, pursuing biological parenthood. 5 The National Comprehensive Cancer Network (NCCN) Guidelines 6 emphasize the importance of screening for and intervening upon AYAs’ sexual and reproductive health concerns; yet, AYAs report sexual and reproductive health to be significant, though underaddressed health care needs.2,7 AYAs often face multiple barriers to receiving sexual health care, including (1) provider and patient discomfort with discussing AYAs’ sexual health concerns (e.g., providers may not ask about sexual health concerns, patients may not initiate conversations about sexual health concerns) 8 ; (2) providers’ general lack of knowledge about and infrastructure to support patients in addressing their sexual health concerns (e.g., clinical practice guidelines, trained multidisciplinary providers, referral networks) 2 ; (3) lack of time or other cancer-related concerns taking priority during clinic visits 9 ; and (4) inconsistent screening for and assessment of sexual health concerns for AYAs. 2 AYAs also face critical barriers to improved reproductive health care, including (1) lack of comprehensive information and guidance on fertility risks and fertility preservation options; (2) concerns about delaying cancer treatment; (3) uncertainty about the desire for parenthood; and (4) lack of financial support and insurance coverage for fertility care. 10 It is therefore critical that tailored information and support be readily available to address AYAs’ specific sexual and reproductive health needs.
AYA survivors are more likely than older survivors to search online through websites and social media for cancer-related information, and their searches commonly include sexual and reproductive health topics.11–13 For AYAs to access credible information and learn about available resources and supports, it is imperative that cancer centers provide up-to-date and easily navigable information on their websites. This study aimed to characterize the presence of AYA-specific sexual and reproductive health programs and resources at National Cancer Institute (NCI)-designated cancer centers and comprehensive cancer centers, as advertised on individual centers’ websites.
Materials and Methods
Design
The websites of all NCI-designated cancer (n = 9) and comprehensive cancer (n = 58) centers were reviewed between September 21 and October 5, 2023, to examine the presence of information about AYA-specific sexual and reproductive (i.e., oncofertility) health programs and resources. A single review of each website was conducted by three independent coders (L.A., U.N., and I.L.), all of whom were female. Coders were trained undergraduate researchers who were supervised by two PhD-level faculty members (C.D. and R.S.) and a PhD-level post-doctoral associate (J.S.). Coders completed initial training with the larger study team, where the standardized coding template developed for the study was reviewed and definitions for each component to be input into the template were clarified (i.e., see definitions below). During this initial meeting, the team jointly coded information from three websites to ensure similar understanding of codes and consistency in coding. The investigative team met weekly to discuss and review the coding process, resolving any discrepancies in use of the coding template or application of codes. One coder (L.A.) reviewed all websites again in February, April, and June 2024 to identify any new programs or resources that had been added to the websites in the time since the initial review.
Sexual and reproductive health programs and resources were identified using three methods: (1) navigating cancer centers’ websites (e.g., clicking on a menu item titled “Patients,” then clicking on a hyperlink titled “Support Services”), (2) using the search bar embedded within a cancer center’s website, and (3) using a general search engine (i.e., Google Search). Search terms for center-specific website search engines included “AYA,” “adolescent and young adult,” “sexual health,” “AYA sexual health,” and “oncofertility.” These search terms were also used for the general search engine, with the addition of the cancer center name. In addition to searching each cancer center, the websites of any affiliated children’s hospitals were reviewed using similar search criteria. Information gathered was then input into the coding template, specifying the presence of programs and resources related to sexual and reproductive health that were advertised on each study website (see “Analytic Strategy” section for additional details).
Analytic strategy
The team developed project-specific definitions and search procedures (see Fig. 1), which were included in the coding template. A “program” was identified when in-house clinical services were advertised collectively with the purpose of achieving a specific goal (e.g., to address sexual health) and described specifically with the word “program” on the webpage. “Resources” were defined as: (1) support services, (2) internal educational resources, and (3) external educational resources. “Support services” were defined as clinic services, consultations, psychotherapy, physical therapy, and retail services specific to addressing sexual and/or reproductive health concerns. “Internal educational resources” were defined as online educational information developed by the center and pertaining to sexual and/or reproductive health, including written information on web pages, videos, infographics, brochures, and patient manuals. “External educational resources” were defined as links to sexual and/or reproductive health information developed by other organizations (e.g., Elephants and Tea). Consolidated Criteria for Reporting Qualitative Research were followed as applicable. 14
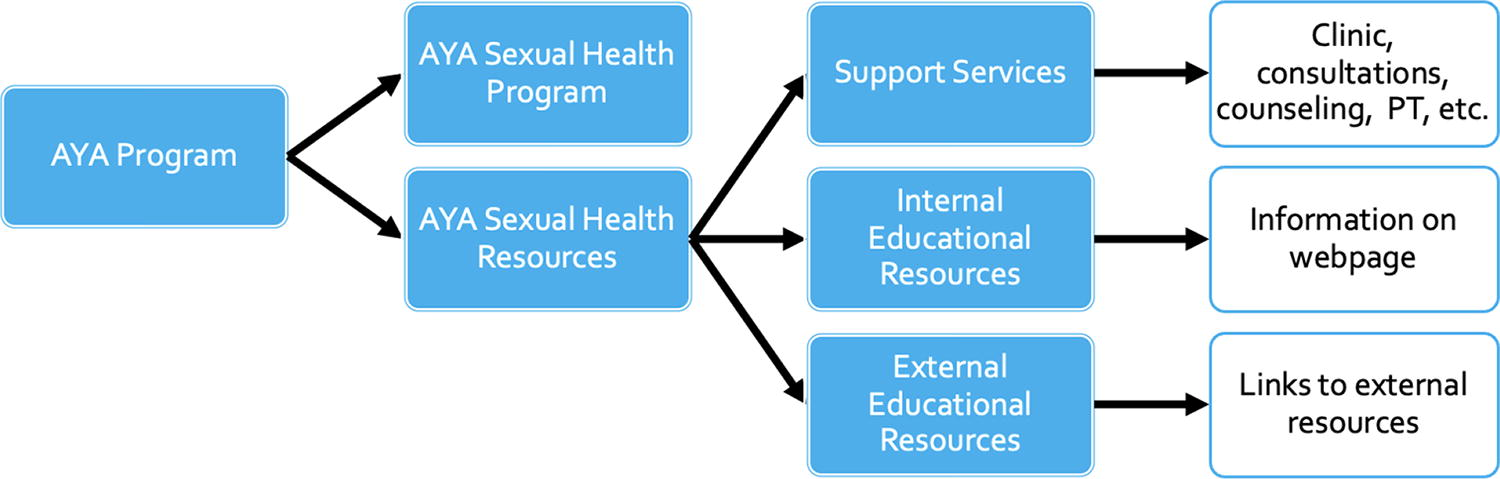
Search criteria used to identify AYA sexual health programs and resources. AYA, adolescent and young adult.
The coders first identified whether an AYA program was advertised and then reviewed the AYA program webpage for the marketing of AYA-specific sexual and reproductive health programs and resources. The team also documented if general (not AYA-specific) sexual or reproductive health programs or resources were marketed to patients on cancer centers’ websites. For example, non-AYA-specific sexual health programs were documented if they advertised sexual health-related support services and/or survivorship care to patients and survivors of cancer but did not specify that the program was designed for certain age groups. Descriptive statistics were used to characterize the frequency of available programs and resources.
Results
One-third (n = 3) of cancer centers’ and approximately 52% (n = 30) of comprehensive cancer centers reported on their websites to have a center-affiliated AYA program (see Table 1 and Fig. 2). None of the centers with AYA programs reported having sexual health programs specifically targeting AYAs. The websites of one (11.1%) cancer center and nine (15.6%) comprehensive cancer centers provided AYA-specific sexual health resources, with 40% (n = 4) classified as information about support services (e.g., questions to ask your providers about sexual health; information about and hyperlinks to available counseling services at the institution), 40% (n = 4) classified as internal educational resources (e.g., information about safety, including sexually transmitted infections, compromised immunity, pregnancy risk), and 20% (n = 2) classified as external educational resources (e.g., links to information from the American Cancer Society about sexual health concerns for cancer survivors). All (n = 10) of the AYA sexual health resources were identified via a general search engine, 70% (n = 7) were identified via center-specific website searches, and 50% (n = 5) were identified via navigation of the center’s website.
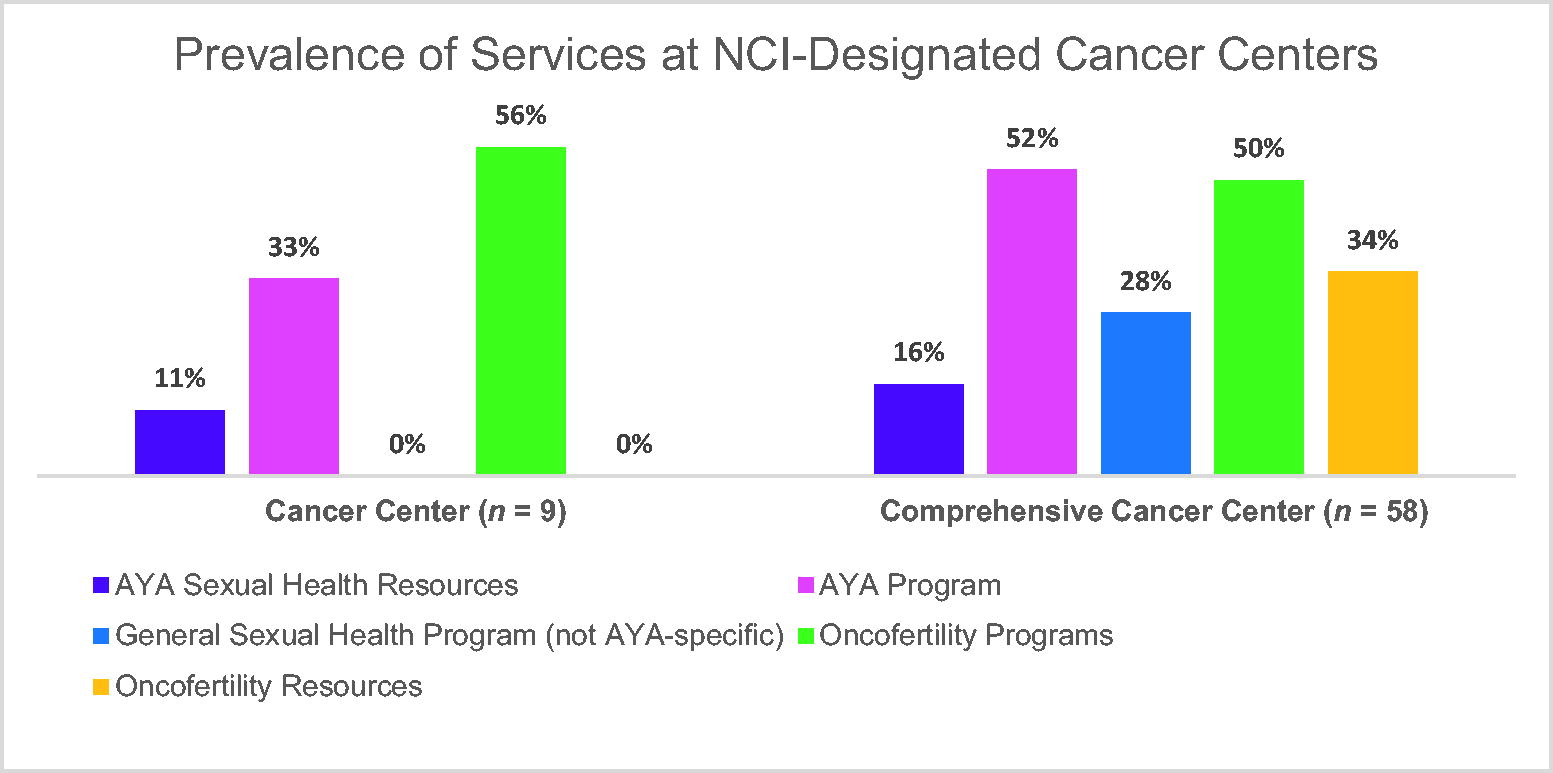
Prevalence of sexual and reproductive health services at NCI-designated cancer centers. NCI, National Cancer Institute.
Geographic Location of Sexual and Reproductive Health Services at NCI-Designated Cancer Centers
State-level information was not included for states with NCI-designated cancer and comprehensive cancer centers that reported zero availability of the specified program/resource on center websites.
AYA, adolescent and young adult; NCI, National Cancer Institute.
The websites of ∼28% (n = 16) of comprehensive cancer centers advertised having sexual health programs for oncology patients more broadly; none of the cancer centers advertised sexual health programs. For example, several comprehensive cancer centers advertised gender-specific sexual health programs, but these programs did not specifically target AYAs (e.g., The Ohio State University Women’s Integrated Sexual Health Program; the Smilow Sexuality, Intimacy, and Menopause Program at the Yale Cancer Center; the Sexual Health in Women Impacted by Cancer Program offered by the Oregon Health & Science University Knight Cancer Institute and the Oregon Health & Science Institute Center for Women’s Health; Memorial Sloan Kettering Cancer Center’s Sexual Health Program for Males and Sexual Health Program for Females; Fox Chase Cancer Center’s Men’s Sexual Health Program and Erectile Dysfunction Clinic and Women’s Menopausal and Sexual Health Program).
Oncofertility programs were advertised on the websites of ∼56% (n = 5) of cancer centers and 50% (n = 29) of comprehensive cancer centers. Reproductive health and oncofertility resources (e.g., links to general fertility service information) were present on the websites of 34% (n = 20) of comprehensive cancer centers.
Table 1 provides an overview of the geographic locations of available sexual and reproductive health services. Although 36 states have NCI-designated cancer and comprehensive cancer centers, only 19 (52.7%) states have centers with advertised AYA programs. Centers in 13 (36.1%) states advertised non-AYA-specific sexual health programs, and centers in 23 (63.9%) and 15 (41.7%) states had centers that advertised oncofertility programs and resources, respectively. Even fewer states had centers that advertised AYA-specific sexual health resources (13.9%). Some states had a larger number of these programs and resources (e.g., California, New York, North Carolina), while many states had very few to no advertised sexual and reproductive health programs and resources for cancer survivors, let alone for AYAs specifically.
Discussion
Despite recognition of the prevalent, persistent, and impactful sexual health concerns experienced by AYA cancer survivors and a growing consensus on the importance of addressing sexual health concerns among AYAs, 6 a review of the websites of NCI-designated cancer centers and comprehensive cancer centers revealed zero AYA-specific sexual health programs. Just under one-third of NCI-designated comprehensive cancer centers’ websites advertised sexual health programs for cancer survivors, more broadly. NCI-designated cancer centers and comprehensive cancer centers meet rigorous standards for providing state-of-the-art cancer care, and most are affiliated with academic medical centers. Yet, the inclusion of sexual health information and center-specific services for cancer survivors, let alone AYA-specific services, on center websites was rare.
It is possible that cancer centers may not advertise all available resources and programs within their institution on their websites. However, AYAs are “digital natives,” 15 having been brought up with the internet as a regular part of their lives; consequently, the internet serves as a primary source when seeking health information.16–18 When searching for information about or solutions to cancer-related sexual health concerns, AYAs may naturally look to the internet, including the website of their treating cancer center, for information. If sexual health information is not readily available, patients may instead look to other web-based resources (e.g., YouTube) and social media (e.g., Tik Tok, Instagram) that may or may not provide accurate or credible information. 19 Even in the absence of a sexual health program, cancer centers should aim to have easily navigable websites with links to accurate, up-to-date, external resources to ensure AYAs receive critical, evidence-based sexual health information.
Despite the general lack of sexual health programs and resources, information about oncofertility-related programs and resources was more often included on centers’ websites. As many as 44%–86% of AYAs experience reproductive concerns secondary to cancer and cancer treatments. 4 Given the significant reproductive health impacts faced by many young cancer patients and the time-sensitive nature of fertility preservation, it is encouraging that available oncofertility programs and resources are prominently displayed on centers’ websites. There are several possible reasons why oncofertility programs and resources were more commonly included on centers’ websites when compared with sexual health. If sexual health programs and resources are advertised, providers must be prepared to discuss patients’ concerns. Oncology providers rarely receive formal sexual health training.20,21 A recent survey completed by 114 hematology/oncology fellowship program directors found only 49% of programs to provide formal instruction in sexual health, while 75% offered formal instruction in fertility-related issues. 21 Sex is also commonly viewed as taboo in the United States, 22 which may further impact providers’ comfort with sexual health discussions. 23 Due to variations in cultural, societal, and religious norms, sexual and reproductive health discussions are often reserved for married, heterosexual couples, with providers having less comfort discussing these topics with younger, unpartnered, or sexual- and gender-minority-identifying individuals.24,25 Providers may feel even less comfortable discussing sexual health topics with AYAs due to the presence of parents or other family members during clinic visits. 23
The discipline of oncofertility is now approaching its second decade. 26 As the use of assisted reproductive technologies has become more common, oncofertility resources have also become more common. Providers are generally comfortable discussing fertility-related topics with AYAs,27,28 which may be due to increased training as well as available medical solutions (e.g., sperm or oocyte cryopreservation, in vitro fertilization) to assist AYAs with family building. If sexual health is discussed, providers must be prepared to refer AYAs to appropriate clinical services to address their concerns. Evidence-based approaches to addressing sexual health concerns, particularly among female patients, are more limited. Due to the relative infancy of the field of onco-sexual health, there are also a limited number of medical and behavioral health providers with expertise in addressing the sexual health needs of cancer survivors, let alone the sexual health needs of AYA survivors, and these limited services may be offered by a variety of different provider types (e.g., physical therapists, psychologists, physicians). There is a need to increase the onco-sexual health workforce to advance the availability of sexual health programs and resources and ultimately facilitate comprehensive sexual health care for AYAs.
Limitations
There are several limitations of this study that warrant attention. Cancer center websites are periodically updated; thus, this study presents only a snapshot of available programs and resources as listed on centers’ websites at the time of review. While we have taken steps to review centers’ websites on multiple occasions, it is possible that sites may have changed by the time of publication. Further, it is possible that the cancer centers’ websites may not list all programs and resources available to patients. Given AYA’s penchant toward seeking cancer-related health information on the internet, inclusion of all available programs and resources on centers’ websites is imperative.
Additionally, we did not examine the websites of cancer centers or clinics that do not have NCI-designated status. NCI-designated cancer centers and comprehensive cancer centers receive their designations due to the presence of state-of-the-art services. Given the limited available sexual health resources on the websites of NCI-designated cancer and comprehensive cancer centers, it is likely that community cancer centers are even less resourced. Additional research is necessary to understand the availability of sexual health programs and resources for AYA patients who are treated in the community. If this work confirms our hypothesis that community cancer centers lack AYA-specific sexual health programs and resources, system-level interventions will be necessary to improve access to care.
Clinical and Research Implications
Sexual and reproductive health is incredibly important to AYAs, yet our review of cancer center websites revealed that, consistent with prior research, the sexual health needs of AYAs may be underaddressed. NCCN AYA guidelines recommend that sexual health be addressed with AYAs as an “essential” part of their health care, providing education, routinely asking about the impact of cancer and cancer treatments on sexual health, and providing referrals to specialists when possible. 6 Yet, research suggests that oncology providers rarely discuss sexual health topics with AYAs.8,9,29 The onus often falls on the patient to initiate conversations with their providers about their sexual health concerns. Including sexual health resources and programming for AYAs on cancer centers’ websites are the first steps in normalizing sexual health changes and reassuring patients that concerns can be addressed within the context of their cancer care. If clinical expertise in medical and behavioral management of sexual health concerns is not available at the cancer center, including links to reputable resources and knowledgeable community providers can help to ensure patients receive credible information and access to services to address their concerns.
Additional work is necessary to explore whether NCI-designated cancer centers and comprehensive cancer centers offer sexual health services—AYA-specific or otherwise. Bober and colleagues 30 recently surveyed NCI- and NCCN-affiliated cancer centers to learn about the availability of sexual health aids in the centers’ retail stores and patient boutiques. Using the “mystery shopper” method, centers were queried via telephone to learn whether sexual health aids were available. Use of the “mystery shopper” method could take the present work a step further to anonymously query NCI-designated cancer centers and comprehensive cancer centers to learn more about sexual and reproductive health services, programs, and resources that may be present at the institution but not listed on the centers’ websites. This strategy would help to characterize the true availability of sexual and reproductive health programs and resources.
Based on our review, it appears that there are geographic disparities in the availability of sexual and reproductive health programs and resources for AYAs and cancer survivors, more broadly. Future qualitative research would assist with understanding barriers to developing and implementing AYA-specific sexual health programs and resources. It is likely that barriers are multifaceted. Gaining a better understanding of these barriers can help facilitate access to and optimally promote and advertise services.
Conclusions
As the number of AYA survivors grows, it will be important for cancer centers to provide comprehensive care and services to meet AYAs’ unique sexual and reproductive health needs. AYAs are “digital natives,” often searching for information and support around sexual and reproductive health on the internet. It is imperative that cancer centers prominently display available sexual health and oncofertility programs and resources on their websites in a way that is easily navigable for patients.
Footnotes
Authors’ Contributions
The article has been approved by all the authors. Conceptualization: C.S.D., R.A.S., J.M.S., L.A., I.L., and U.N. Methodology: C.S.D., J.M.S., and R.A.S. Formal analysis: L.A., I.L., and U.N. Funding Acquisition: C.S.D., R.A.S., and S.S.A. Investigation: C.S.D., J.M.S., L.A., I.L., and U.N. Writing—original draft: C.S.D., A.L., and J.M.S. Writing—reviewing and editing: R.A.S., I.L., U.N., C.C., and S.S.A.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This study was funded by the Duke Bass Connections Program awarded to C.S.D., R.A.S., and S.S.A. C.S.D. was supported by a career development award from the National Institutes of Health (