
Abstract
Objectives:
Breastfeeding is highly important for a child's health, and the widespread use of herbal medicines as galactagogues has been reported. The present study was conducted to evaluate the use of traditional, complementary, and integrative medicine (TCIM) and its determinants among breastfeeding mothers in Shiraz, Iran.
Design:
Cross-sectional study.
Setting/Location:
Neonatal clinics affiliated to Shiraz University of Medical Sciences.
Subjects:
Mothers elder than 18 years old.
Interventions:
Nothing.
Outcome Measures:
Prevalence and of the use of TCIM products and its associated factors.
Methods:
In this cross-sectional study, mothers older than 18 years who referred to neonatal clinics affiliated to Shiraz University of Medical Sciences were enrolled. Using a structured interview, the authors explored the prevalence and of the use of TCIM products and its associated factors.
Results:
Of 625 mothers who were approached, 483 agreed to participate (response rate: 77.3%). The average age was 27.3 ± 5.9 years. The prevalence of using TCIM products during current breastfeeding was 97.1%. There were 168 working mothers (44.9%); 163 mothers (34.1%) complaining of postpartum breastfeeding problems, and 327 mothers (68%) had no history of breastfeeding. Recommendations of medical staff or relatives were the most frequent reasons for the consumption of TCIM products (64.9%). Only 27% of mothers disclosed the use of TCIM products to their doctor or health care provider, although 62% of mothers were asked about the use of such products. Notably, 438 mothers (95.8%) considered TCIM to increase their milk. Based on multivariable logistic regression, literacy and past use of TCIM galactagogues were independently associated with TCIM products use.
Conclusions:
The use of TCIM galactagogues is highly common among breastfeeding mothers in south of Iran, showing a diverse range of determinants. It is necessary to evaluate the safety and efficacy of common herbal galactagogues, and evidence-based studies must be designed to achieve standardized complementary medicine approaches in this regard.
Introduction
Breast milk is the ideal food for infants, providing various benefits to both the mother and child. 1,2 The World Health Organization (WHO) vehemently supports breastfeeding, recommending its continuation for a minimum of 24 months as it is an important right of the mother and infant and improves their health. 3 Breast milk contains a variety of vitamins, minerals, proteins, and unsaturated fatty acids and is rich in antimicrobial, anti-inflammatory, and immunomodulatory compounds. 4,5 Hence, it reduces the infant's risk of acquiring certain gastrointestinal, respiratory, and infectious diseases. It also has beneficial effects on the cardiac, neurological, endocrine, and immune function of the infant. 6,7 For the mother, breastfeeding is associated with a reduced risk of breast, endometrial, and ovarian cancer, as well as decreased bleeding and accelerated return of the uterus to its original condition. 8
Various factors affect the duration of a mother's breastfeeding, including their education level, economic status, family support, and family stability. Other influential factors are breastfeeding skills and maternal knowledge in this regard. 9 Despite its importance, breastfeeding is discontinued for a variety of reasons, including fatigue, problems with breastfeeding techniques, and not having enough milk. 9 Early onset of complementary foods following weaning the child from breastfeeding can cause complications such as malnutrition, obesity, and allergies, while increasing the risk of gastrointestinal, respiratory, and infectious diseases in the newborn. 1,10 However, not having enough milk can decrease the mother's confidence and give rise to mental health problems. 11
The use of traditional, complementary, and integrative medicine (TCIM) has been expanding in the past decade globally. 12 According to reports of the WHO, a considerable number of herbal compounds and dietary supplements are used by people in both developed and developing countries. 13 If applied properly, TCIM can help meet the needs of breastfeeding mothers and can guide them toward successful breastfeeding. 14
In TCIM, there are several ways to increase the mother's milk, including acupuncture, massage, kangaroo mother care, relaxation, and herbal medicine. 15 The use of herbal products represents one of the prime aspects of TCIM, with the promotion of lactation being one of the key applications of such products. 16,17 Galactagogues are foods, herbs, or medications that support the initiation, continuation, or reinforcement of breastfeeding. 18 Notably, mothers often choose to use herbal supplements because they believe that they are safer, more reliable, and cheaper than chemical drugs. 18,19 Many foods and medicines have lactation-inducing properties, with the choice of fruits, foods, and herbs consumed for this purpose varying from country to country. 17,20
In addition to the effect of plants on milk quantity, their effect on milk quality is also important. Plants induce changes in the process of breastfeeding by altering the color, smell, taste, and quality of milk. 19,21 In Iran, breastfeeding has been known to people since long ago, with Avicenna mentioning this issue in The Canon of Medicine in the 10th century. 22
In Persian Medicine (PM), a holistic medical discipline which is run in Iran and western Asia for several ages, the greatest determinant of milk production is regarded as the production of high-quality blood humor, making proper nutrition highly influential in increasing the mother's breast milk. The scope of PM practitioners ranges from lifestyle modification to hands-on physical manipulations. In PM, lactating mothers are recommended to refrain from consuming certain plants in large volumes or for prolonged periods, some examples of which are garlic, onion, and lentils. This is because such plants can alter the quality of milk. 22 –25
Despite the crucial roles of breast milk in the child's health and all-round development (especially during the first 6 months of life), it is possible that the mother discontinues breastfeeding, particularly due to not having enough milk—an erroneous perception of insufficient milk supply, which commonly reinforced by the health professional. 26 Although various plant and food products are used by breastfeeding mothers in Iran, the precise range of compounds used is yet to be delineated in Shiraz, Iran. Meanwhile, despite the importance of the provision of appropriate TCIM prescriptions by medical staff, most breastfeeding mothers opt for self-medication when taking up TCIM. 12 Therefore, the present study was conducted to assess the prevalence of TCIM use and its determining factors among breastfeeding mothers in an urban area in southern Iran.
Materials and Methods
A cross-sectional study was conducted in the autumn of 2020 in Shiraz, Fars, Iran. The city of Shiraz is the most populous urban area in southern Iran, hosting a population of ∼2 million people. According to the latest statistics of Shiraz University of Medical Sciences, the demographic characteristics of women in Shiraz is as follows: literacy rate: 91.4%; employment rate: 64.6%; gender ratio (male/female): 0.98; proportion married: 75.1%; proportion in reproductive years: 59.8%; predominant ethnicity: Persian; official language: Persian; predominant religion: Muslim (Shia).
Study population
Mothers aged 18 years or older who were willing to breastfeed their child, who was aged between 0 and 24 months, were eligible for inclusion in the study. Mothers who lived outside Shiraz, lacked the ability to speak in Persian, or were pregnant were excluded. Mothers with systemic diseases (hypoglycemia, hypothyroidism, hyperthyroidism, uncontrolled blood pressure, etc.) or liver diseases (severe fatty liver, cirrhosis, etc.) were also excluded.
The sample size was calculated using the formula of the Cochran for prevalence studies. The authors assumed the prevalence of using herbal galactagogues to be 15%, with a first type error of 5% and a prevalence estimation accuracy of 20%. The response rate was considered to be 85%. Based on these assumptions, the sample size required was estimated to include 625 people.
Sampling was done using the multistage random cluster sampling technique. First, in each of the 10 urban regions of Shiraz, the authors determined and selected the central government facility providing mother and child health services. Then, the authors proceeded with sampling during all working hours and days at the selected centers for 2 months. All eligible mothers who referred to the centers were first acquainted with the study and its objectives before being invited to participate. Ultimately, mothers who expressed informed consent were interviewed.
Data collection
Data were collected using a structured interview based on a researcher-made questionnaire. Initially, a conceptual framework was designed based on a review of the literature and group discussion sessions. This conceptual structure included the mothers' views on the use of TCIM compounds in reinforcing breastfeeding, their experiences with the use of TCIM, common compounds used by breastfeeding mothers, reasons and factors that facilitate the use of TCIM compounds, and the mothers' interactions with mother and infant health service providers regarding the use of TCIM products.
A team consisting of a PM specialist, a gynecologist/obstetrician, a pediatrician, and a methodologist was formed, with each member being asked to design questions for each component of the conceptual framework. A total of 80 questions were designed, 27 of which were selected for the final questionnaire after multiple group discussions. The questionnaire included seven sections, namely demographic data (age, education, occupation, monthly income and expenses, place of residence, and ethnicity), information related to pregnancy, birth, and breastfeeding (number of pregnancies, duration of current breastfeeding, history of abortion, birth order, breastfeeding problems, history of breastfeeding, duration of previous breastfeeding, history of using TCIM compounds in previous breastfeeding, number of mother and child health services received, and use of formula feeding), and five other components of the conceptual framework.
The content and face validity of the questionnaire were assessed by seven experts from the related disciplines, and the suggested corrections were made when deemed appropriate. Then, a pilot questionnaire was used to collect data from 15 breastfeeding mothers to detect and resolve any problems. Ultimately, the final questionnaire consisted of 25 multiple choice (Likert scale), yes/no, or short answer questions. To evaluate the reliability of the questionnaire, the test–retest method was used where 30 breastfeeding mothers aged 18 to 40 years were interviewed twice with a 2-week interval between the interviews. Among the questions, the lowest test–retest correlation coefficient obtained was 0.84, with a p-value of >0.001. The reliability of the questionnaire was also assessed using Cronbach's alpha, which was found to be equal to 0.79.
The interviews were conducted by 10 trained midwives working in the selected mother and child health care centers. The interviews lasted for an average of 15 min and were conducted in a private room at each center.
Statistical analysis
Data were cleaned and prepared. Descriptive statistics including mean, standard deviation, frequency, and relative frequency (%) were estimated and presented to describe the data. Age-standardized prevalence (ASP) proportion was estimated by applying direct standardization method. Two independent sample test was applied to univariate analysis of the association of continues predictors with the study outcome. Fisher's exact or chi-square tests were applied for univariate analysis of the association of categorical variables with the TCIM use.
Multivariable binary logistic regression modeling was applied to estimate the adjusted odds ratio (OR) and their 95% confidence interval (CI) as the measure of independent association of the studied variables with the TCIM use. Variable selection was performed based on a univariate p-value of <0.3. Stepwise modeling technique was applied. A p-value of <0.05 indicated statistical significance. Data analysis was carried out by using Stata software (Release 11.2; Stata Corp LLC, College Station, TX, USA). (See attached Supplementary Data).
Ethical considerations
The study protocol was based on the Declaration of Helsinki for Medical Research Involving Human Subjects. Before commencing the research, the protocol was approved by the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.REC.1397.1020).
Results
Of 625 breastfeeding mothers who were asked to participate, 483 mothers participated in the study (response rate = 77.3%). The mean age of the participants was 28.1 ± 5.6 years. About 63% (n = 300) had a university qualification, and about 79% (n = 360) were residents of urban areas. Approximately 35.4% (n = 164) of mothers worked outside the home (paid employment). The prevalence of TCIM usage was calculated as 91.7% (95% CI: 88.8%–93.8%), with the ASP being 52.1% (95% CI: 50.1%–54.1%) (Table 1).
Sociodemographic and Background Characteristics Associated with the Use of Traditional, Complementary, and Integrative Medicine Products (N = 483)
Row percentages.
SD, standard deviation; TCIM, traditional, complementary, and integrative medicine.
Notably, 90% of mothers who had a positive past experience with the use of TCIM galactagogues reported current use of these products. Of mothers who used TCIM to improve their breastfeeding, 75.6% (n = 317) believed that these compounds could be recommended to others. This figure was 62.5% (n = 25) among mothers who were not current users of TCIM galactagogues (p = 0.068). From the mothers who used TCIM products to improve lactation, 52.0% (n = 230) believed that these products have at least minimal side effects (Table 2).
Participants' Viewpoints and Experiences About the Traditional, Complementary, and Integrative Medicine and Chemical Drugs
Percentages were calculated based on the cumulative response numbers, as some mothers reported more than one TCIM products used during their breastfeeding period.
NA, not applicable.
The prime reason for selecting the use of TCIM galactagogues was recommendations by relatives (64.9%) and medical staff (64.9%). However, the low cost of TCIM compounds was the least common reason for choosing to use such compounds among mothers who used TCIM (Fig. 1).
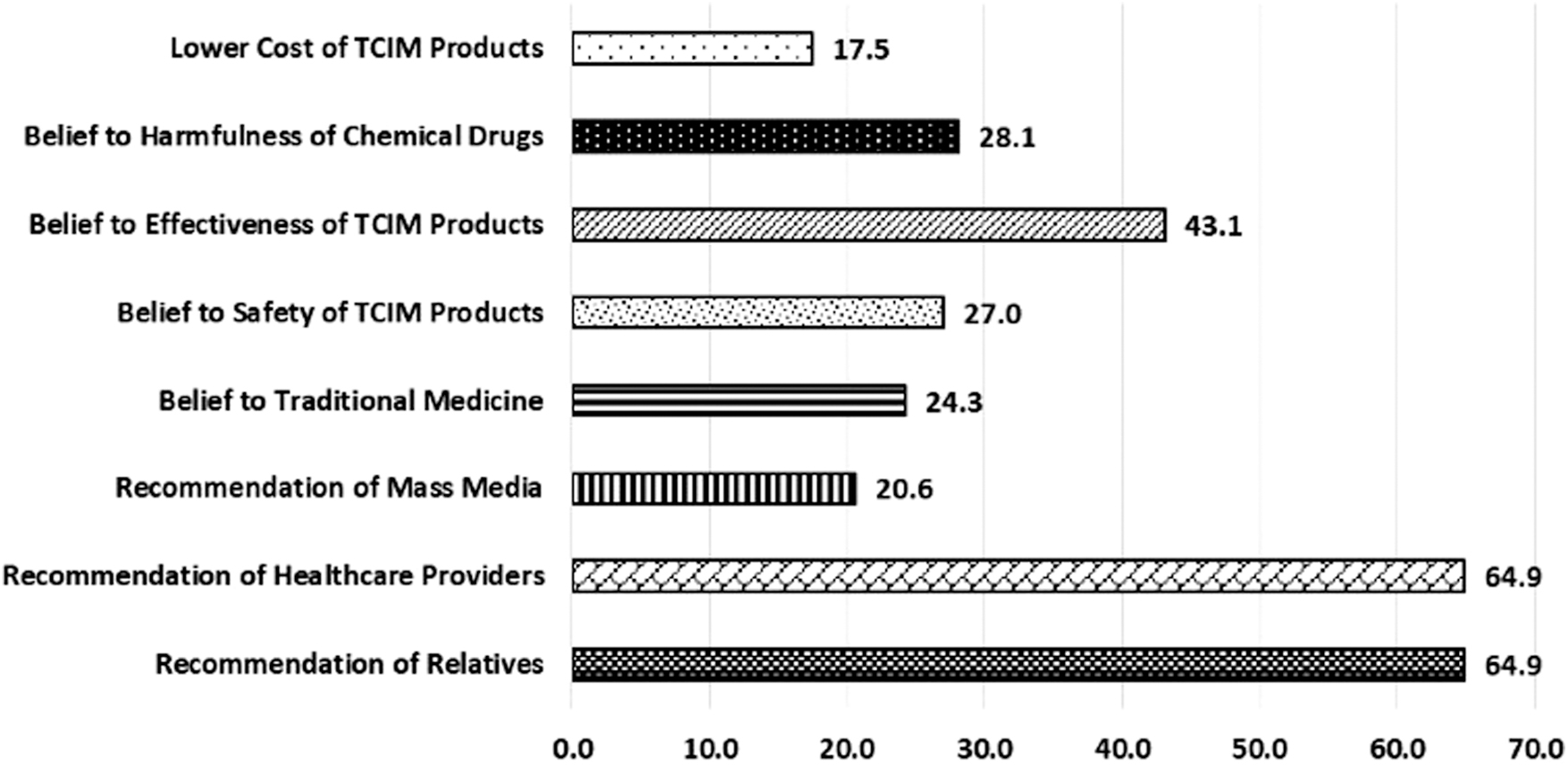
Reasons for the use of TCIM products in lactating mothers (in percent). TCIM, traditional, complementary, and integrative medicine.
According to the self-reported data from mothers participating in the study, natural products that were consumed for more than 10 days and in large quantities to induce lactation during breastfeeding included lentils (31.8%; n = 54), coffee (25.9%; n = 44), fresh parsley (15.9%; n = 27), garlic/onion (4.7%; n = 8), barley (15.9%; n = 27), lemon juice (3.5%; n = 6), and senna leaf (2.4%; n = 4). Interestingly, 62% of medical staff had asked mothers regarding the history of using TCIM while visiting medical centers, with 73% of mothers refraining from disclosing their TCIM use to their health care provider (Fig. 2).
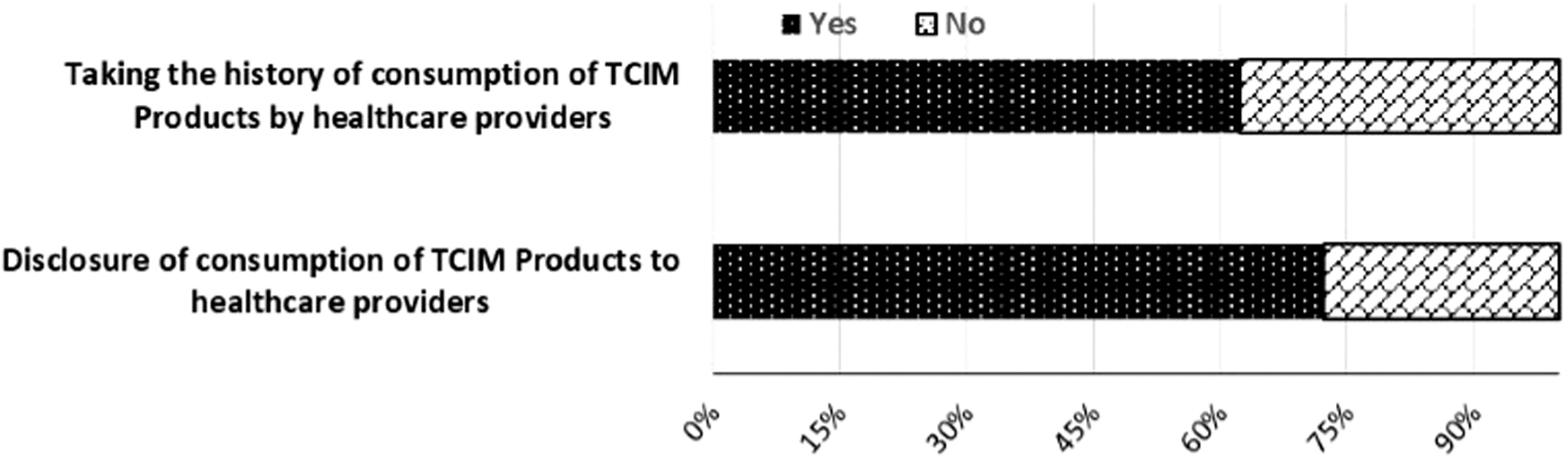
Participants' disclosure and health care provider's report about the TCIM products use during breastfeeding.
The highest prevalence of usage was related to iron supplementation (24%) and herbal galactagogue drops (21%) containing fennel, cumin, fenugreek, and dill extracts, whereas the lowest prevalence was related to folic acid (1%) (Fig. 3).
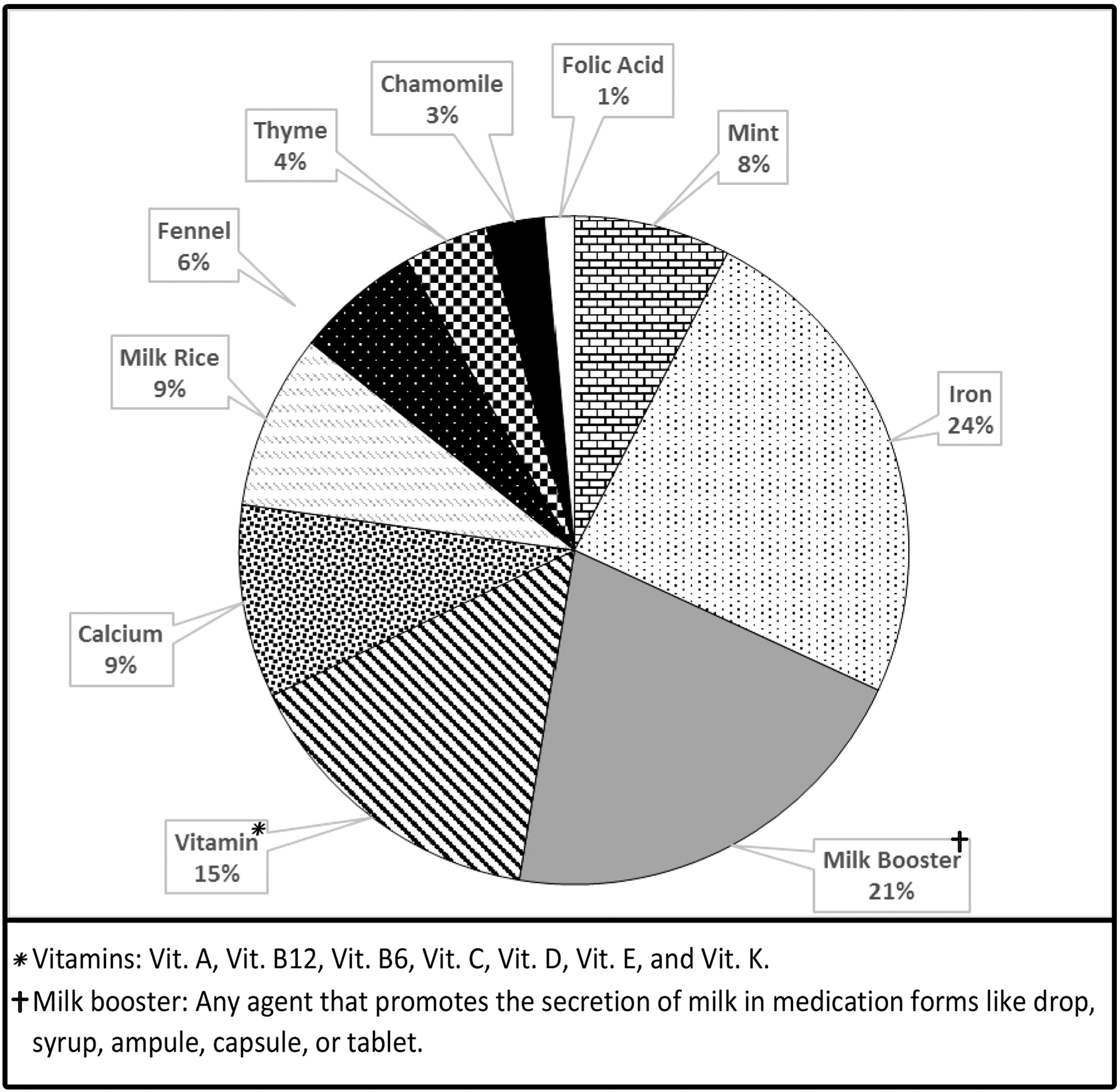
Participants' distribution of the TCIM products use during breastfeeding.
Based on multivariable logistic regression analysis, the likelihood of TCIM use among illiterate mothers was 96% lower relative to literate mothers (OR: 0.04, 95% CI: 0.006–0.32). Moreover, the prevalence of TCIM usage among mothers who did not have a history of its usage was about 80% lower than mothers who reported a positive past usage (Table 3).
Associated Factors with Traditional, Complementary, and Integrative Medicine Use Among Iranian Lactating Mothers, 2020
CI, confidence interval; OR, odds ratio.
Discussion
In this study, a significant percentage of mothers (97.1%) had used TCIM during breastfeeding, which is higher than the percentage of complementary medicine use in Australia (59.9%), China (45%), Taiwan (87.7%), the United States (16%), and Sierra Leone (37%), but is close to the results reported in Italy (97.3%). 16,19,21,25,27,28 Of course, if the authors consider the ASP, this rate (52.1%) will be very close to the results of Australia and China. Perhaps one of the reasons for the difference to the results of countries such as Taiwan or Sierra Leone is the lack of using the ASP index. Therefore, to facilitate comparison of prevalence indicators among different communities, standardization based on the ASP is suggested.
The rate of TCIM uses varies from country to country. 29 This may be due to variations in study design (sampling technique, inclusion/exclusion criteria, etc.), differences among individuals living in different communities (cultural, economic, etc.), variations in the definition of TCIM, or variations in herbal medicine species deepening on the native vegetation of each country. As a result, the availability and popularity of TCIM compounds vary between countries.
In this study, the main reason for using TCIM while breastfeeding was to induce lactation (66.4%). However, in Italy and Sierra Leone, mothers often used TCIM for other reasons, with only 2.8% and 2.1% of them using TCIM to induce lactation, respectively. 16,28 This figure was lower in Iran even compared with Australia, where more than half of mothers (60.4%) used complementary medicine to increase their milk. The high use of TCIM galactagogues in this study could be due to religious beliefs and the emphasis of Islam on breastfeeding. 30 Support for working mothers and national breastfeeding promotion programs in Iran 31 may also contribute toward continuing breastfeeding and making use of TCIM galactagogues.
In this study, 64.2% of mothers who used TCIM had received academic education (higher than high school diploma). This figure is lower relative to the United States (81%) and Macau (87%), but higher compared with Sierra Leone (5.7%) and Malaysia (18.1%). 16,25,32,33 A number of recent studies have shown a positive association between higher education and increased TCIM usage. 34 It is possible that with higher education, a greater awareness of the benefits and risks of TCIM is achieved, resulting in increased rational use of TCIM products. In the present study, multivariable regression analysis also showed a much higher prevalence of TCIM usage among breastfeeding mothers with higher education relative to those with lower education.
Interestingly, the authors found that 36.6% of breastfeeding mothers using TCIM were employed, which is less than the figures reported in the United States (56%), Malaysia (89.2%), and Sierra Leone (52.1%). 16,25,33 However, the multivariable regression analysis showed that working mothers used TCIM about 75% less than housewives. Perhaps one of the reasons behind this difference is the lack of enough time of working mothers to utilize TCIM services due to employment and less opportunity for regular follow-ups. If this is the case, local health systems must work toward raising awareness about the risks of missing regular maternity follow-ups.
In this study, as in similar research conducted in Taiwan and Australia, the mothers were predominantly primiparous (64.4%). 2,27 This may be explained by a higher rate of referrals among women in this group due to less experience concerning the breastfeeding process. Although the authors selected a representative sample of breastfeeding mothers and did not have access to population distribution of the order of pregnancy, it is impossible to rule in/out the selection bias. Notably, 65.8% of mothers who had used TCIM did not have breastfeeding problems. The high rate of TCIM usage (97.1%) in this group may be due to the effect of advertisements regarding the use of galactagogues or the mothers' desire to boost their milk quality and achieve better infant weight gain.
In this study, most recommendations regarding TCIM usage came from relatives and medical staff (general practitioners and midwives). The extent to which Iranian physicians prescribe TCIM products and consider them to be effective has been investigated in prior studies. 35 In comparison, the highest proportion of recommendations regarding the use of complementary medicine came from friends in the Malaysian study (60%) and from family in the Australian study (61.5%), showing consistency with the data. 2,33 In Italy, however, obstetricians/gynecologists made the most TCIM recommendations (44%). 28
Belief in the effectiveness of complementary medicine (43.1%), in the harm of chemical drugs (28.1%), and in the safety of TCIM (27%) were other factors contributing to high rate of TCIM use seen in this study. In Sierra Leone, the affordability, availability, effectiveness, and safety of TCIM products contributed to their usage. 16 In the Malaysian study, most mothers (65%) chose herbal galactagogues because of their natural components. 33 Attention to these factors and planning to provide correct information to breastfeeding mothers should be prioritized by infant health planners at the national and regional levels.
One substantial finding of the present study is that most breastfeeding mothers (73%) were reluctant to report the use of TCIM compounds to medical staff. In line with this finding, 88.6% of mothers did not report TCIM treatments in Sierra Leone, mostly because they deemed it to be unnecessary. 16 Also, in this study, only 62% of the medical staff had asked regarding the history of TCIM usage. The need to inform mothers about the use of TCIM according to their health status is a matter that should be discussed, 36 and it seems necessary for staff in health centers to ask all breastfeeding mothers about TCIM usage.
In this study, 39% of mothers who used TCIM believed that TCIM reported no side effects. Also, 51.9% considered complementary medicine to have minimal complications, and 99.8% of mothers who used herbal galactagogues during breastfeeding had experienced no side effects. According to a recent review, most mothers believe that herbal medicines to be safer than chemical medicines. 32 Likewise, most mothers in Italy held that herbal medicines are safe and low risk. 28 This is while herbal medicine is not completely harmless. For example, fennel, which has been introduced as a galactagogues in several studies, can lead to photosensitivity, dermatitis, diarrhea, and estrogenic effects. Due to the possibility of cross-allergenicity, mothers who are allergic to products of the Apiaceae family (e.g., carrots and celery) must avoid using fennel. 17,28,37 Although the risk of complications is higher in the breastfeeding mother, the infant may also experience adverse effects following the use of herbal medicine by the mother. 17 Therefore, medical staff should discuss the effectiveness and side effects of TCIM with breastfeeding mothers, and the safety and effectiveness of TCIM products should be evaluated. 27 In fact, some studies have shown that mothers themselves desire to be provided with further information about TCIM. 2,36
Numerous studies have been performed on galactagogues, although in many cases the studies have not been sufficiently valid or have not used an appropriate method. 17,38 In galactagogues, such as other TCIM drugs, the authors must consider contaminations and effective substances. Standardization and the development of pure herbal products are also important, and their safety should be checked against the Generally Recognized As Safe list. 17,39
Despite the fact that 59.5% of breastfeeding mothers in this study reported that the use of galactagogues had led to a definite increase in breast milk, and although side effects were reported in only two cases, about 60% of mothers who used TCIM during breastfeeding believed that TCIM galactagogues could not be recommended to all mothers. According to the literature, this lack of recommendation may be due to the low efficacy of TCIM or the possibility of adverse effects. 40 The effects of past TCIM usage and a higher number of past deliveries should also not be overlooked, where the multivariable regression analysis showed that these two factors boost the chance of choosing to use TCIM by ∼80% and 60%, respectively.
According to the findings, the most commonly used herbal medicines among breastfeeding mothers were mint, fennel, thyme, and chamomile, with the predominant reason of usage being to induce lactation. In the U.S. study, chamomile and cranberry were most widely used among mothers following childbirth, whereas the Italian study revealed fennel, licorice, and aloe to be the most commonly used herbal products. 25,28 In Australia, the plants most widely used during breastfeeding were fenugreek and ginger. Furthermore, chamomile was used in 7.2% of cases, predominantly for relaxation purposes, whereas 4.9% of breastfeeding mothers reported the use of fennel for increasing their milk and minimizing infantile colic. 2
The most common non-herbal medicine used by breastfeeding mothers in this study was iron supplements (24%). In the U.S. study, omega-3 was found to be the predominantly used supplement among postpartum mothers (6.6%). 25 This difference can be due to culture dissimilarities and variations in the availability, affordability, and the method of use of these products in different countries and regions.
Among the plants that were used for more than 10 days were garlic and senna, which should be avoided during breastfeeding according to the references of PM. Rhazes 41 stated that plants that have a cold and dry or very hot temperament reduce breast milk, although some studies have revealed that garlic and senna can increase breast milk. In the studies of Bazzano et al. 42 and Nice, 43 garlic was included in the list of common herbal galactagogues. However, Mennella and Beauchamp used garlic capsules and placebos in their study and found no significant differences in lactation between the intervention and control groups, with infantile colic being reported as an adverse effect in both groups. 44 Another study showed that garlic can alter the smell of milk, thereby making it undesirable for the infant. In the study by Nice, 43 it was noted that garlic can prolong the duration of breastfeeding but can also cause discontinuation if it is inappropriate for the infant. It seems that studies on the use of these two herbs during breastfeeding are contradictory, meaning that the advice of PM scholars to avoid their long-term use (more than 10 days) is perhaps reasonable.
In the present work, the study population was mothers who referred to government health centers, who may differ in terms of demographic characteristics from those who attend private health sector. Nonetheless, it should be noted that the majority of Iranian mothers refer to government health centers during breastfeeding. However, the findings are based on data obtained using a structured interview, where the possibility of inaccurate responses from the mothers cannot be overlooked. One of the strengths of this work is the use of multivariable regression analysis, which removes the effects of confounding factors.
Conclusions
The present study showed the high prevalence of TCIM usage among breastfeeding mothers in Shiraz as a sample of the Iranian population. Various factors influenced the volume and type of TCIM products used, the most important of which were literacy, employment, number of deliveries, and past TCIM use. The authors recommend performing similar studies in nearby countries to establish a comprehensive comparison, thereby facilitating health policymaking. Furthermore, such data would allow us to design accurate, evidence-based clinical trials to determine the effectiveness and safety of TCIM products in breastfeeding women.
Footnotes
Authors' Contributions
Conceptualization: H.M.V. and M.P. Methodology: H.M.V., Z.S., and M.P. Data curation: Z.S., F.A., and M.P. Formal analysis: H.M.V., Z.S., and M.P. Investigation: Z.S., H.C., and M.P. Writing—original draft: H.M.V., Z.S., F.A., H.C., and M.P. Writing—review and editing: H.M.V., H.C., and M.P. Supervision: H.M.V. and M.P. All authors have read and approved the final article.
Acknowledgments
The authors appreciate all the breastfeeding mothers participating in this research study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.