
Abstract
Objective:
Meta-analysis was used to quantitatively examine the effectiveness of Traditional Chinese Health-Promoting Exercise (TCE) as an adjuvant therapy for drug use disorders and rehabilitation based on previously published studies.
Methods:
Potential literature was retrieved by searching eight electronic databases (China National Knowledge Infrastructure [CNKI], Wanfang, Chinese Scientific Journal Database, China Biology Medicine [CBM], PubMed, Embase, Cochrane Library, and EBSCOhost) from January 2000 to May 2021, as well as through manual searches, including email. These literature reports comprised randomized, controlled trial studies and nonrandomized, controlled trial studies assessing the effects of TCE intervention on the physical and psychological (mental) health of drug addicts. The quality and bias risk of each study were assessed using the Cochrane bias risk assessment tool. The RevMan5.3 statistical software was employed to evaluate the methodological quality of the included studies, and sensitivity and subgroup analyses using the Stata16.0 MP software were performed to explore the sources of heterogeneity among the data. This study is registered on PROSPERO (CRD42021254124).
Results:
Data from 14 studies (1094 individuals with drug abuse) meeting the inclusion criteria were extracted for meta-analysis. Compared to the control group, TCE intervention induced significant improvements in the systolic blood pressure (standardized mean difference [SMD] = −0.42, p < 0.05), diastolic blood pressure (SMD = −0.34, p < 0.05), one-leg stand with eyes closed (SMD = 0.74, p < 0.05), Symptom Check List (SMD = −0.42, p < 0.05), anxiety scale (self-rating anxiety scale/STI) (SMD = −0.49, p < 0.05), and depression scale (self-rating depression scale/Beck Depression Inventory/Hamilton Depression Rating Scale for Depression) (SMD = −0.37, p < 0.05). Sensitivity and subgroup analyses of the individual outcome indicators with high heterogeneity (I 2 ≥ 50%, p < 0.10) were performed to further explore the source of heterogeneity. The results of the sensitivity analysis showed that, after removing studies one by one, the heterogeneity of the data remained high (I 2 > 50), and the difference of synthetic overall effect did not change (p < 0.05), indicating that the sensitivity was low and that the results were robust and reliable. The results of the subgroup analysis results indicated that the gender of the participants and the drug type were the sources of heterogeneity.
Conclusion:
As an effective mind-body movement intervention, long-term TCE is beneficial to improving the physical and mental health of drug addicts. The specific intervention methods are dependent on the gender of the addict and the drug type, and longer intervention times yielded greater impacts on their physical health.
Introduction
Substance abuse disorders are a major economic and health care burden throughout the world and can result in deleterious social consequences, such as divorce, crime, and unemployment. 1 In particular, illicit drugs, such as heroin, marijuana, methamphetamine, cocaine, and ketamine, cause physical, mental, and spiritual suffering for substance abusers, their families, and society. 2 According to the latest World Drug Report (2020) released by the United Nations Office on Drugs and Crime (UNODC), ∼269 million people reported using drugs worldwide in 2018, which is 30% higher than in 2009, and a total of 35 million people suffered from drug use-related disorders in 2018. 3 Because of the limited availability of treatment services worldwide, only one in seven drug abusers receives treatment each year. 4
Repeated drug abuse can often lead to drug addiction, which is a chronic brain disorder characterized by compulsive drug use, despite the harmful consequences, due to impairments in the brain's reward circuit. Drug addicts can experience a range of physical withdrawal symptoms, such as high blood pressure, lower limb fatigue, insomnia, and tachycardia, as well as psychological symptoms, such as depression and anxiety, upon cessation of chronic drug use, not to mention a high tendency of relapse. High relapse rates have ultimately affected the sustainability of global antidrug efforts. Methamphetamine abuse causes damage to the structure and function of the brain, and, at the same time, causes a variety of mental disorders. 5 Similar studies in animals and humans have found that long-term abuse of methamphetamine led to the destruction of dopaminergic and serotonergic nerve fiber pathways in the brain, resulting in the continuous depletion of dopaminergic neurotransmitters. 6 Stroke sequelae and somatic diseases like myocardial infarction are common manifestations in traditional drug abusers, and mental disorders are common in new synthetic drug abusers.
There are philosophical differences in medical care between Traditional Chinese Medicine (TCM) and modern western medicine. The theoretical basis of TCM is described in the Huangdi Neijing, written during the period of 475-225 BC. TCM has a holistic view that human health is the “unity of body, mind, and spirit” and that everyone is born with the ability of self-recovery. The best treatment according to TCM involves the balance of energy flow, which depends on the operation of “qi” in the body. TCM includes well-known herbal medicine, acupuncture, massage (tui na), and lifestyle modifications, such as dietary therapy and Traditional Chinese Health-Promoting Exercise (TCE) 7,8 ; TCE is a general term for a wide variety of traditional Chinese energy exercises and therapies, of which there are currently six different kinds promoted throughout the world, including Tai Chi, Yi Jin Jing, Ba Duan Jin, Five-Animal exercise, Six-character formula, and Mawangdui guidance. 9
TCE combines human physical activity with breathing regulation and psychological adjustment, but the emphasis on physical sensation and breathing in TCE is different from normal physical exercise, which focuses on actual performance. 10 Exercises or meditations, such as yoga, Reiki, Zen, Vipassana, and Transcendental Meditation, which are much more well known in Western civilization, are considered forms of TCM in China, and they are all classified as mind-body approaches. 11 Many scholars have utilized nonpharmacological mind-body approaches to stress reduction in difficult-to-manage populations. 12 In addition, regular practice of TCE has shown to be beneficial for improving the physiological function and psychological emotion of college students by promoting the synergy between the body (i.e., breathing) and the mind. 13
Even after physical detoxification and negative urine tests, drug addicts still experience symptoms of anxiety and depression, as well as sleep disorders, in varying degrees. According to TCM theory, long-term illicit drug use can cause an imbalance of the mind, as well as a dysfunction of “qi” and the yin (passive) and yang (active) nature of Zang-fu organs, leading to the development of sleep disorders, anxiety, and depression. The development of abnormal emotions without active treatment will lead to an imbalance of yin and yang in illicit drug users. 14
Since there is no single drug detoxification method, many individuals require long-term rehabilitation and comprehensive treatment processes. In China, TCE has been utilized as a treatment option for drug users and addicts. According to Tai Chi, Ba Duan Jin Wu Qin Xi, Yi Jin Jing, and others, TCE has gradually become an effective means to improve the physique and mental health of drug addicts. 15 Although it can be easily self-taught, success really requires concentration, relaxation, and daily practice. 16 Previous studies have reviewed the effectiveness of Taijiquan and qigong exercise in reducing anxiety and depression among drug addicts because anxiety and depression are the two most common comorbidities 17 ; however, the extent of literature in this area is small, and there is no analysis of the effects of TCE on physical health. Therefore, the purpose of this systematic review is to summarize the existing body of empirical evidence from randomized and nonrandomized, controlled studies on the effectiveness of TCE on the physical and psychological (mental) health of drug addicts as well as to provide more treatment options for detoxification and rehabilitation.
Methods
Registration
This research protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) on June 7, 2021 (Supplementary Data, CRD42021254124). Ethical approval was not required for this systematic review. The Preferred Reporting Items for Systemic Reviews and Meta-Analysis Statement (PRISMA) was adopted to guide the entire systematic review process. 18
Eligibility criteria
To be included for meta-analysis, the studies had to be randomized, controlled trials (RCTs) studies or nonrandomized, controlled trials (NRTs) published in either Chinese or English. The target population of the studies was Chinese citizens 18 years of age or older and diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders or the International Statistical Classification of Diseases and Related Health Problems as suffering from illegal drug abuse/dependence, excluding tobacco, alcohol, Internet, gambling, and other addictions. There was no statistical difference in age, sex, health status, or other demographics. The experimental group included in the form of TCE compared to the control group, with the intervention time being ≥12 weeks.
Outcome indicators included data on physical health indices, including blood pressure (systolic blood pressure (SBP), diastolic blood pressure (DBP), balance/stabilization (one-leg stand with eyes closed [OS]), and body mass index (BMI), as well as and psychological health indices, including the Symptom Check List (SCL-90), the self-rating anxiety scale (SAS), the self-rating depression scale (SDS), the Beck Depression Inventory (BDI), the State-Trait Anxiety Inventory (STAI), and the Pittsburgh Sleep Quality Index (PSQI). Excluded from the review were cross-designed; single-group, self-controlled; cross-sectional; and qualitative studies. In addition, studies that included participants suffering from infectious diseases were excluded. Animal experiments, case reports, reviews, systematic reviews, and republished literature, as well as literature that lacked full text (e.g., only abstracts) or relevant outcomes, were also excluded.
Two reviewers (D.J. and Z.J.) independently examined the studies based on the Cochrane Collaboration System Evaluation Manual (version 5.1.0). Discrepancies were discussed, from which a consensus was reached by a third reviewer (Y.X.).
Databases searches
We ran searches in eight electronic databases (China National Knowledge Infrastructure [CNKI], Wanfang, Chinese Scientific Journal Database, China Biology Medicine [CBM], PubMed, Embase, Cochrane Library, and EBSCOhost) from January 2000 to May 2021 to identify literature reports. Potential studies were retrieved from the databases by combining three sets of search terms, one from each of the following categories: (1) “traditional Chinese medicine,” “traditional Chinese exercise,” “traditional medicine,” “Qigong,” “guide,” “Taiji,” “Tai Chi,” “Ba Duan Jin,” “Yi Jin Jing,” “Five-Animal exercise,” or “Wu Qin Xi”; (2) “substance abuse,” “drug abuse,” “addiction,” or “drug dependence”; and (3) “Randomized controlled,” “Randomized,” or “RCT.” Additional publications and detailed data were manually identified, such as by email and WeChat.
Data abstraction
A standardized data extraction form was developed to extract study characteristics from each of the identified studies, such as the author(s), year of publication, study design, sample size, gender and age of the participants, type and duration of the intervention, outcome measures, and main results. Disputes were resolved by the third investigator (Y.X.) during data extraction.
Methodological quality assessment
The quality of 14 studies was independently evaluated according to the Cochrane Collaboration's for Assessing Risk of Bias by two reviewers, and the differences were resolved by reaching a consensus. The type of bias was classified as selection bias (sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), reporting bias (selective outcome reporting), or other biases. The judgment of the reviewers on each of the seven domains of the included studies was assessed as either low risk of bias, high risk of bias, or unclear risk of bias. 19 To assess the quality of the studies, five or more items were considered a low risk of bias, three to four items were considered a moderate risk of bias, and less than three items was considered a high risk of bias.
Statistical analysis
RevMan Manager (RevMan 5.3) provided by the Cochrane assistance network was used for meta-analysis. The literature outcome indicators included in this article were all continuous variables (mean ± standard deviation). The fixed effect model was used to examine the homogeneity of outcome data among the included studies. The random effect model was used when there was statistical heterogeneity between the studies. The studies were considered heterogeneous when the I 2 and p values were ≥50% and <0.10, respectively. The standardized mean difference (SMD) and 95% confidence intervals (CIs) were calculated.
When I 2 > 75%, the studies were considered highly heterogeneous; thus, sensitivity and subgroup analyses (Stata16.0 MP) were performed to explore the sources of heterogeneity. Forest plots were then generated to graphically represent the analyzed data. Funnel plots of the primary outcomes (SBP, DBP, OS, SAS, and SDS) were used to explore publication bias if the number of studies included in each subgroup was >10. Two people (D.J. and J.Z.) independently assessed the certainty of the evidence, focusing on its clinical significance in relation to the certainty of the evidence.
Results
Literature search
As shown in Figure 1, 18 a total of 542 related references were initially identified from the database searches. A total of 229 potential literature references were retained after deleting duplicates, and 58 of those references were screened and filtered based on the completeness of the text. The remaining 26 references were evaluated by reading the full texts, and 13 references (including 14 RCT/NRT studies) were included in this meta-analysis. Of those 13 references, 11 were published in Chinese 20 –30 and two were published in English. 31,32
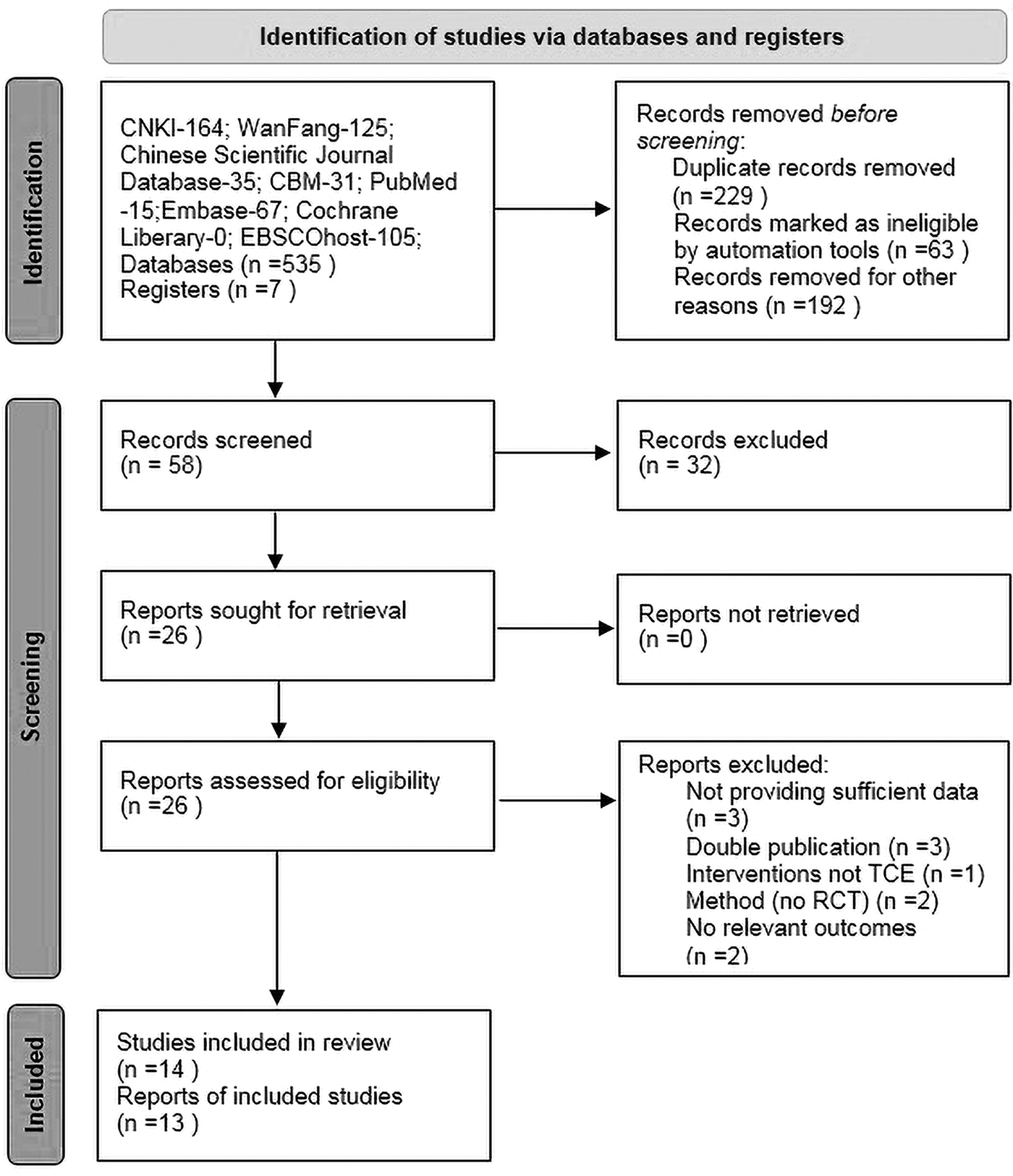
Flow diagram following the PRISMA 2020 for new systematic reviews. As shown in Figure, a total of 542 related references were initially identified from the database. Two hundred twenty-nine potential literature were retained after deleting duplicates and 58 references were screened. Finally, after evaluating the full text of the remaining 26 references, we included 13 clinical studies. Twenty-six references were evaluated through reading full texts, and 13 references (including 14 RCT/NRT studies) were included in this meta-analysis. Eleven references were published in Chinese and two in English. CBM, China Biology Medicine; CNKI, China National Knowledge Infrastructure; NRT, nonrandomized, controlled trial; PRISMA, Preferred Reporting Items for Systemic Reviews and Meta-Analysis Statement; RCT, randomized, controlled trial.
Study characteristics
The basic characteristics of the 14 eligible studies are shown in Table 1. One of the included literature references contained two studies. 23 Articles published after 2018 accounted for 50% of these studies (7/14). The sample size in each publication ranged between 12 and 100 participants (1094 total). In terms of the TCE methods employed, 11 studies reported using an intervention of Tai Chi, 2 studies reported using Ba Duan Jin, and 1 study reported using the five animal exercises. The intervention measures in the control group consisted of mainly routine training, and only one study in the control group was treated with methadone. 30 Of the 14 eligible studies, six studies had an intervention duration of 24 weeks, four studies had an intervention duration in the range of 13–23 weeks, and four had a duration of 12 weeks.
Summary of the Included Studies
BDI, Beck Depression Inventory; BMI, body mass index; C, control group; DBP, diastolic blood pressure; E, experimental group; HRSD, Hamilton Depression Rating Scale for Depression; Meth, methamphetamine; NRS, non-randomized study; NRT, nonrandomized, controlled trial; OS, one-leg stand with eyes closed; PSQI, Pittsburgh Sleep Quality Index; RCT, randomized, controlled trial; SAS, self-rating anxiety scale; SBP, systolic blood pressure; SCL-90, Symptom Check List; SD, standard deviation; SDS, self-rating depression scale; STAI, State-Trait Anxiety Inventory.
Methodological quality
Figure 2 shows the methodological quality assessment according to the quality assessment criteria (the Cochrane Collaboration's for Assessing Risk of Bias from the Cochrane Handbook for Systematic Review Interventions). Nine studies had a low risk of bias and high quality, four studies had a moderate risk of bias and moderate methodological quality, and one study had a high risk of bias and low methodological quality. As shown in the graph in Figure 3, the overall quality of the included studies improved significantly after removing unclear items, except for one study. 33
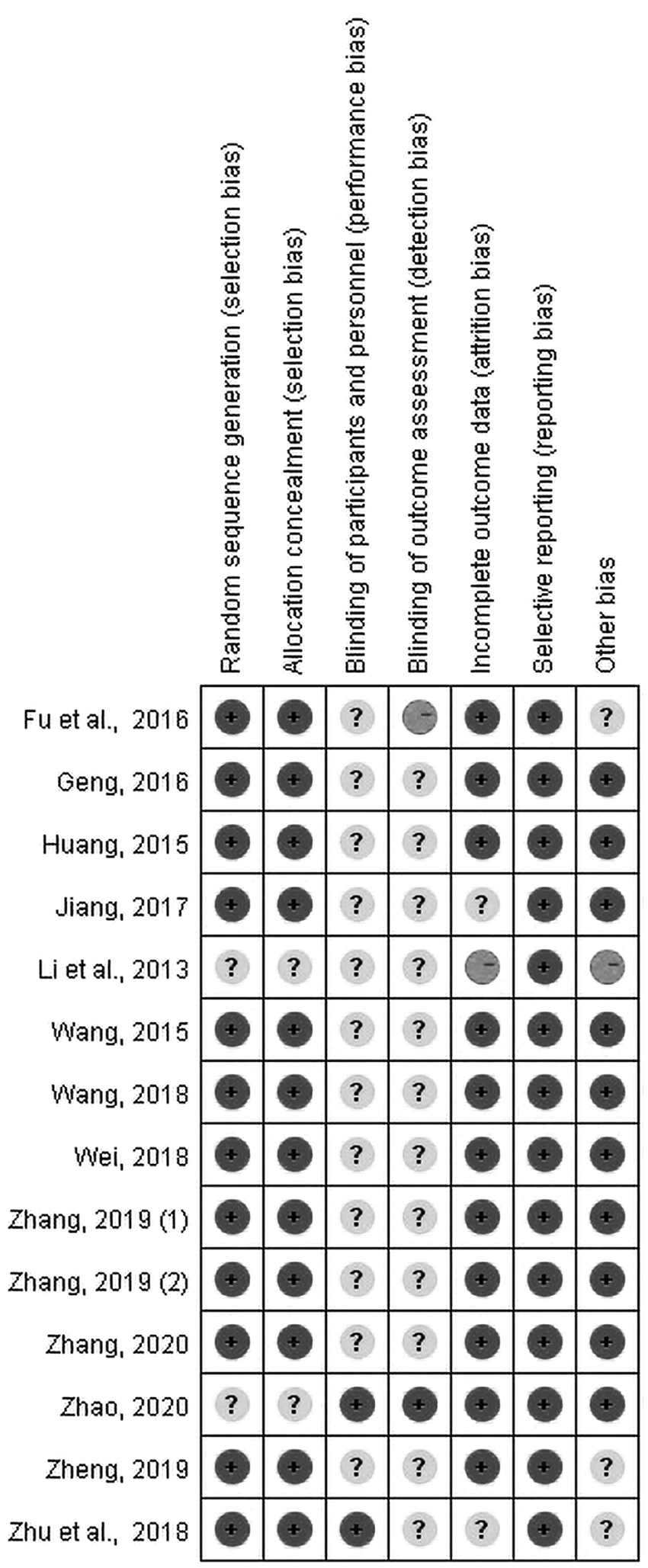
Methodological quality of included studies. Figure showed the methodological quality assessment according to the quality assessment criteria (the Cochrane Collaboration's for Assessing Risk of Bias from the Cochrane Handbook for Systematic Review Interventions). There are nine studies with low bias risk and high quality, four studies with moderate bias risk considered middle methodological quality, and one study with high bias risk considered low methodological quality.
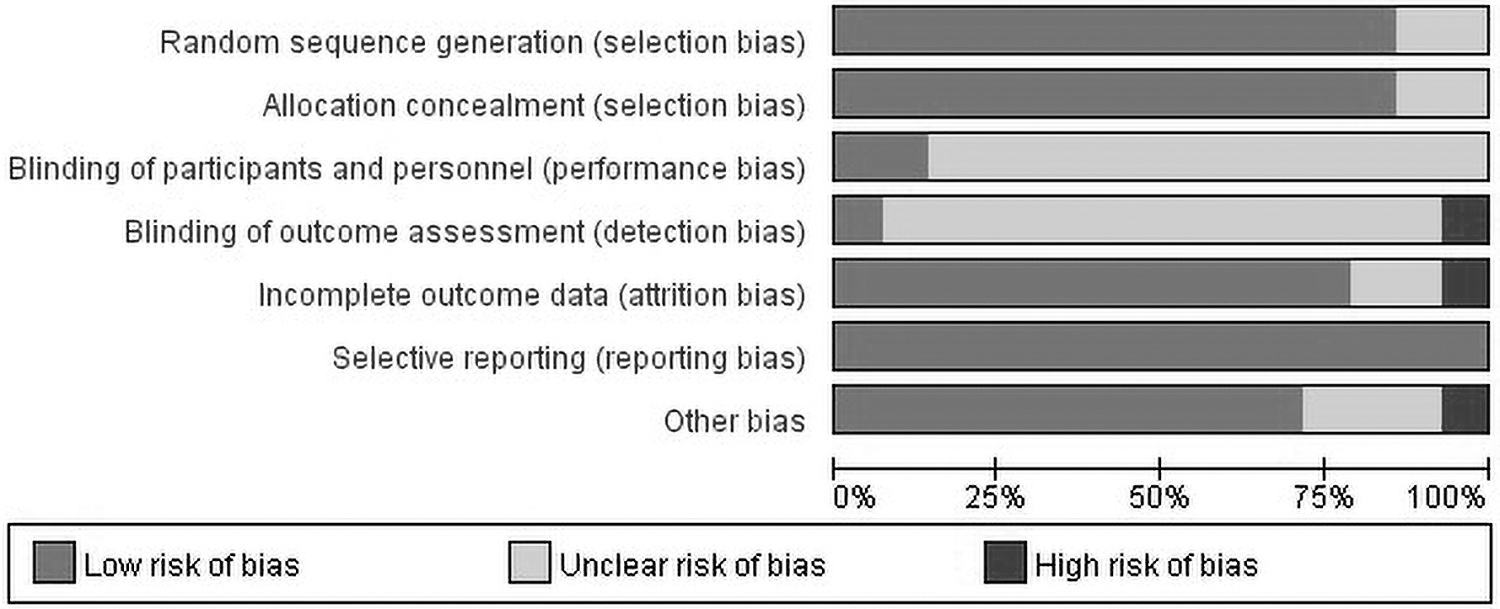
Distribution of the methodological quality of the included studies. As can be seen from the graph in Figure, the included studies showed an overall high quality after removing unclear items, except for one study.
Effects of TCE on physical health
Nine of the 14 studies evaluated the effects of TCE intervention on the physical health of the participants. The outcomes related to physical health mainly comprised three primary outcomes (SBP, DBP, and OS) and one secondary outcome (BMI). Among the 14 total studies, eight reported SBP outcomes, another eight studies reported DBP outcomes, nine studies reported OS outcomes, and seven studies reported BMI outcomes.
Meta-analyses were performed to compare the intervention of TCE to the non-TCE controls, and the random effects model was utilized to merge the outcome measures. The SMD and 95% CI were selected as the effect sizes for meta-analysis. As shown in Figure 4, the results of the heterogeneity test for SBP (χ 2 = 28.61, df = 7, p = 0.0002, I 2 = 76%) and OS (χ 2 = 24.79, df = 8, p = 0.002, I 2 = 68%) suggested significant heterogeneity among the studies. Therefore, sensitivity analysis was performed to further explore the potential heterogeneity of the SBP and OS outcomes (Figs. 5 and 6, respectively).
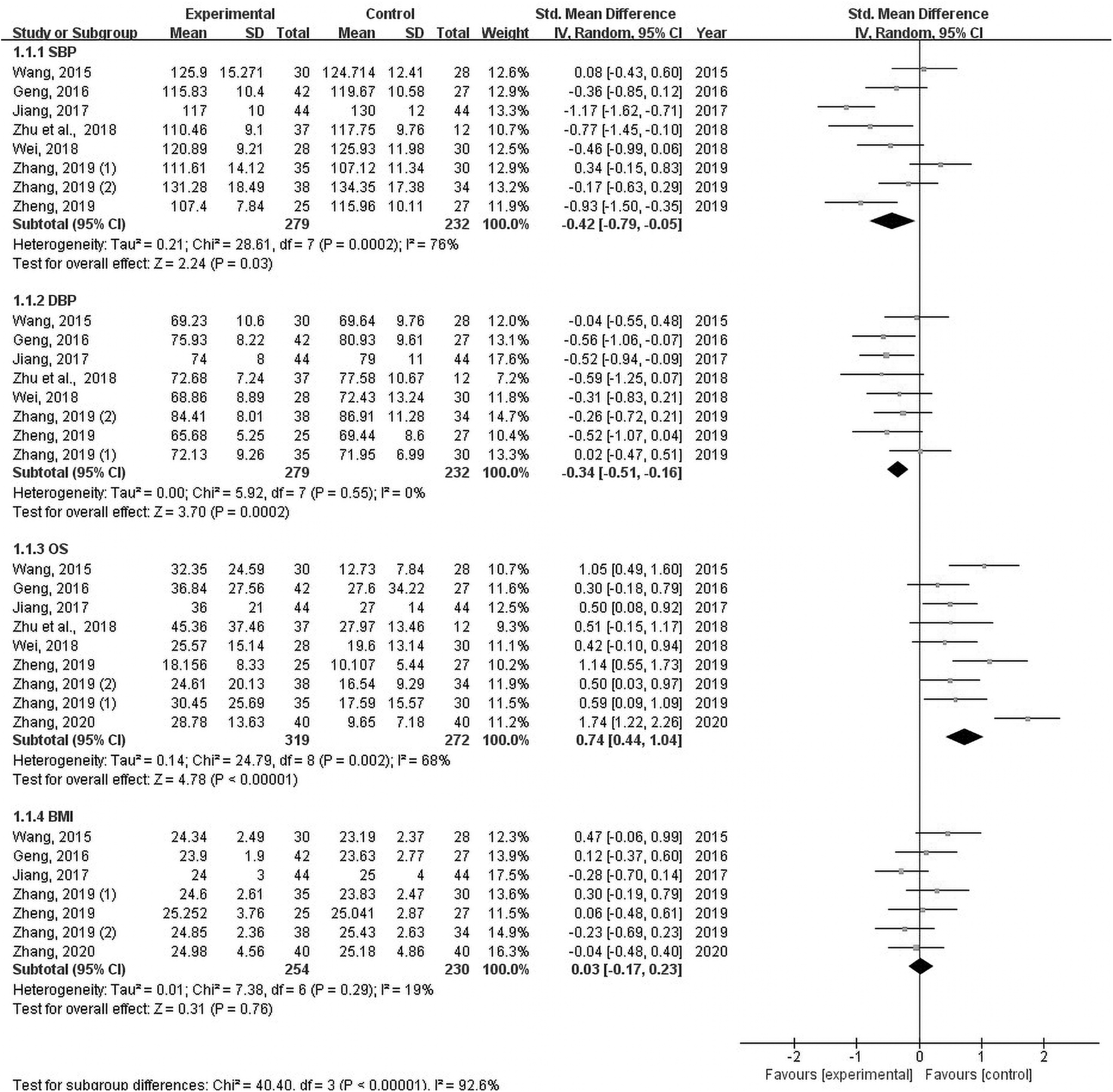
Forest plots of the effect sizes of TCE on physical health. Nine studies evaluated the effects on physical health. Outcomes related to physical health mainly comprised three primary outcomes (SBP, DBP, and OS), and one secondary outcome (BMI). Among them, the four outcome measures reported were SBP (eight studies), DBP (eight studies), OS (nine studies), and BMI (seven studies). Meta-analyses were performed to compare the TCE with non-TCE controls, and the random effects analysis was conducted to merge the outcome measures. SMD and 95% CI were selected as effect quantities for meta-analysis. As can be seen from Figure, the heterogeneity test results for SBP (χ 2 = 28.61, df = 7, p = 0.0002, I 2 = 76%) and OS (χ 2 = 24.79, df = 8, p = 0.002, I 2 = 68%) suggest significant heterogeneity. BMI, body mass index; CI, confidence interval; DBP, diastolic blood pressure; OS, one-leg stand with eyes closed; SBP, systolic blood pressure; SMD, standardized mean difference; TCE, Traditional Chinese Health-Promoting Exercise.
Sensitivity analysis of the SBP outcome. SBP, systolic blood pressure.
Sensitivity analysis of OS outcome. To explore SBP and OS potential heterogeneity, sensitivity analysis was performed, as shown in Figures 5 and 6. After removing the study one by one, we found that heterogeneity (I 2 > 50) was still high, and the difference of synthetic overall effect has not changed (p < 0.05), indicating that the sensitivity is low and the result is robust and reliable. OS, one-leg stand with eyes closed; SBP, systolic blood pressure.
After removing studies one by one, we found that the heterogeneity (I 2 > 50) was still high, and the difference in the synthetic overall effect did not change (p < 0.05), indicating that the sensitivity was low and the results were robust and reliable. This might have been due to the clinical heterogeneity; therefore, subgroup analysis was performed based on the gender of the participants, the type of drug used, and the duration of the intervention. As shown in Table 2, the I 2 values of the heroin and meth subgroups were 40% and 46%, respectively, indicating that there was no obvious heterogeneity in either of the two subgroups and that the drug type was one of the sources of heterogeneity on the SBP.
Subgroup Analysis of the Differences in Systolic Blood Pressure Between the Experimental and Control Groups
CI, confidence interval; MD, mean difference.
In addition, we also found that the I 2 values of the male and female were 33% and 0%, respectively, indicating that there was no obvious heterogeneity in each subgroup (Table 3). It also showed that gender was one of the sources of heterogeneity in OS.
Subgroup Analysis of the Differences in One-Leg Stand with Eyes Closed Between the Experimental and Control Groups
CI, confidence interval; MD, mean difference.
The results of the heterogeneity test showed that there was no significant heterogeneity in the DBP (χ 2 = 5.92, df = 7, p = 0.55, I 2 = 0%) and BMI (χ 2 = 7.38, df = 6, p = 0.29, I 2 = 19%) outcomes between studies, confirming that fixed effect models should be used. The test for overall effect of DBP (p = 0.0002) suggested that TCE intervention was associated with significantly improved DBP (mean difference [MD] = −0.34, 95% CI [−0.51 to −0.16]). However, the test for the overall effect of BMI (p = 0.76) suggested that TCE was associated with a statistically insignificant improvement in BMI (MD = 0.03, 95% CI [−0.17 to 0.23]). The meta-analysis results of the double-tailed test indicated that the combined differences between SBP (p = 0.03), DBP (p = 0.0002), and OS (p < 0.00001) subgroups were statistically significant, such that long-term (12–24 weeks) TCE was effective for improving the physical health of drug addicts.
Effects of TCE on psychological health
Because the methods for measuring and the representation units of anxiety and depression are different among different studies, SMD and 95% CI were selected as the effect sizes for meta-analysis. A total of 13 studies were selected for evaluating the effects of TCE on the psychological health of study participants. The included studies that analyzed the SCL-90, SAS (STAI), SDS (BDI/Hamilton Depression Rating Scale for Depression [HRSD]), and PSQI outcomes were combined to assess the overall homogeneity of each of the outcomes among the studies.
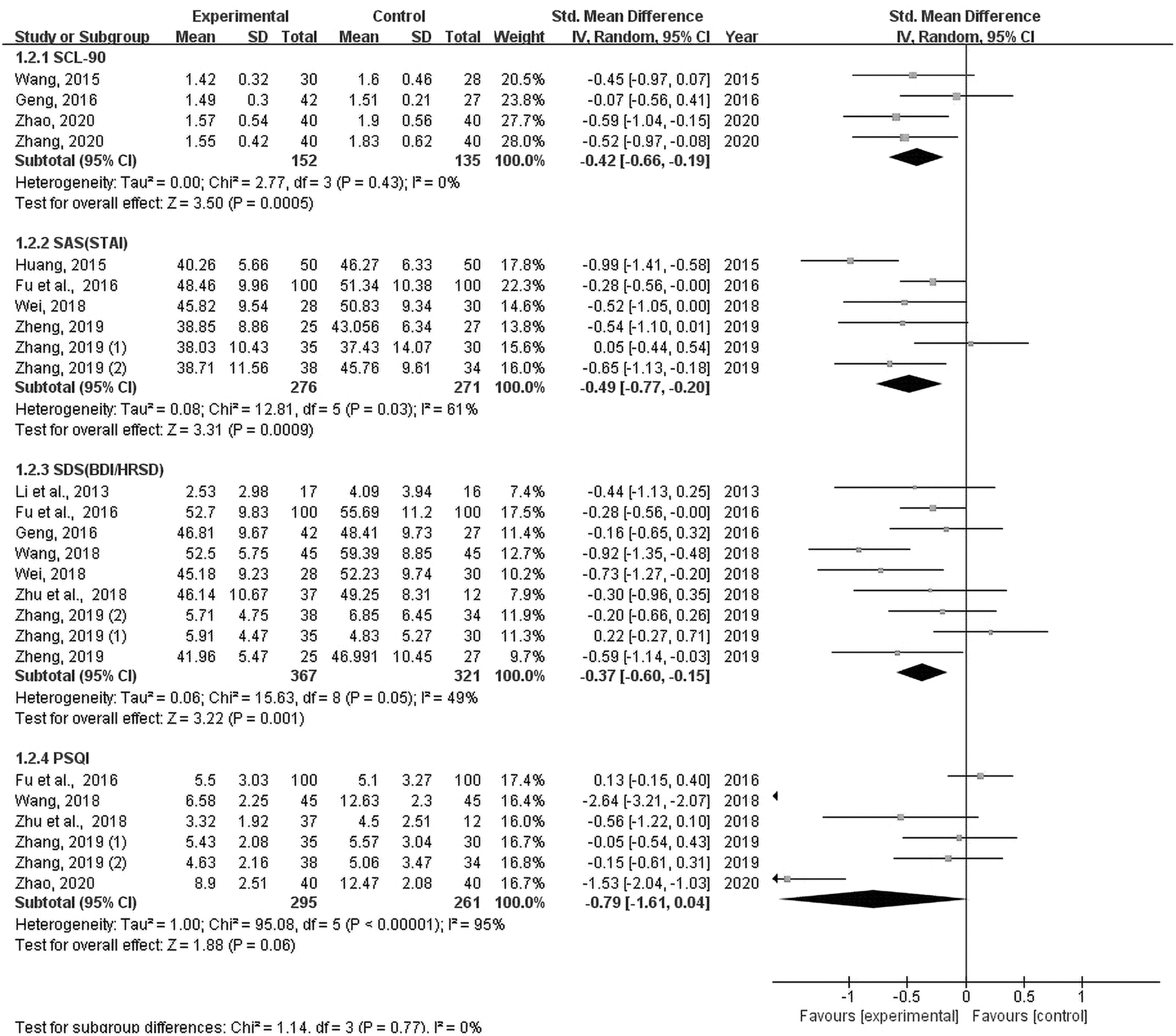
As shown in the forest plots of the effect sizes of TCE on psychological health in Figure 7, heterogeneities were present in the SAS (STAI), SDS (BDI/HRSD), and PSQI data, so the random effect model was employed to further analyze the heterogeneity. The results of the heterogeneity tests on anxiety (SAS/STAI) (χ 2 = 55.32, df = 6, p < 0.000001, I 2 = 89%), depression (SDS/BDI/HRSD) (χ 2 = 51.09, df = 9, p < 0.000001, I 2 = 82%), and PSQI (χ 2 = 95.08, df = 5, p < 0.000001, I 2 = 95%) suggested significant heterogeneity. However, there was no significant heterogeneity in the SCL-90 data (χ 2 = 2.77, df = 3, p = 0.43, I 2 = 0%) among the studies. The test for the overall effect of SCL-90 (p = 0.0005) suggested that TCE was associated with significantly improved mental symptoms (SMD = −0.42, 95% CI [−0.66 to −0.19]).
Forest plots of the effect sizes of TCE on psychological health. Because the measurement methods and representation units of anxiety and depression are different among different studies, SMD and 95% CI are selected as the effect quantity to meta-analysis. A total of 13 studies were evaluating the effects on psychological health. After combining the included studies of SCL-90, SAS (STAI), SDS (BDI/HRSD), and PSQI were combined to assess the overall homogeneity, respectively. Figure showed that there were heterogeneities in SAS (STAI), SDS (BDI/HRSD), and PSQI, so the random effect model was used to analyze the heterogeneity. The heterogeneity test results on anxiety (SAS/STAI) (χ 2 = 55.32, df = 6, p < 0.000001, I 2 = 89%), depression (SDS/BDI/HRSD) (χ 2 = 51.09, df = 9, p < 0.000001, I 2 = 82%), and PSQI (χ 2 = 95.08, df = 5, p < 0.000001, I 2 = 95%) suggest significant heterogeneity. As for the SCL-90 (χ 2 = 2.77, df = 3, p = 0.43, I 2 = 0%), there have no significant heterogeneity in the result of heterogeneity test. The test for overall effect of SCL-90 (p = 0.0005) suggested that TCE is associated with significantly improved mental symptoms (SMD = −0.42, 95% CI [−0.66 to −0.19]). BDI, Beck Depression Inventory; CI, confidence interval; HRSD, Hamilton Depression Rating Scale for Depression; PSQI, Pittsburgh Sleep Quality Index; SAS, self-rating anxiety scale; SCL-90, Symptom Check List; SDS, self-rating depression scale; SMD, standardized mean difference; STAI, State-Trait Anxiety Inventory; TCE, Traditional Chinese Health-Promoting Exercise.
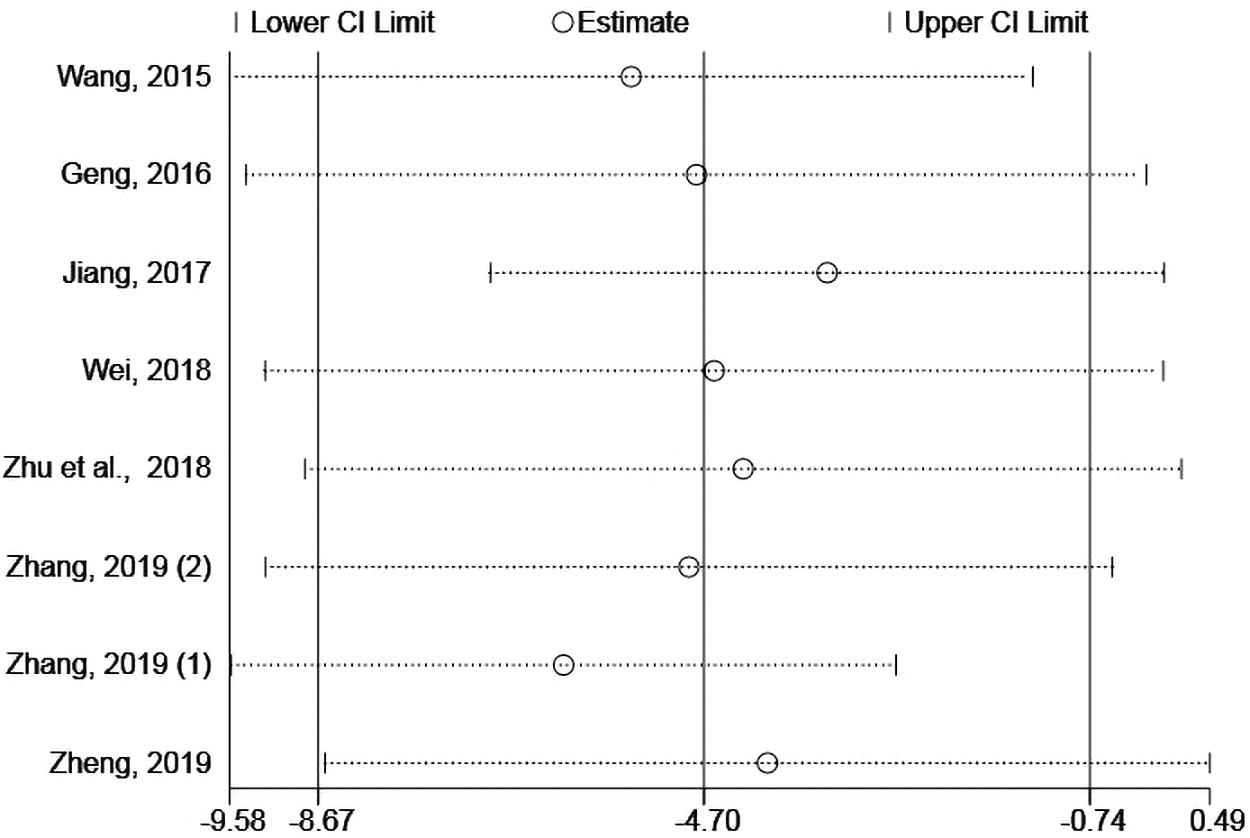
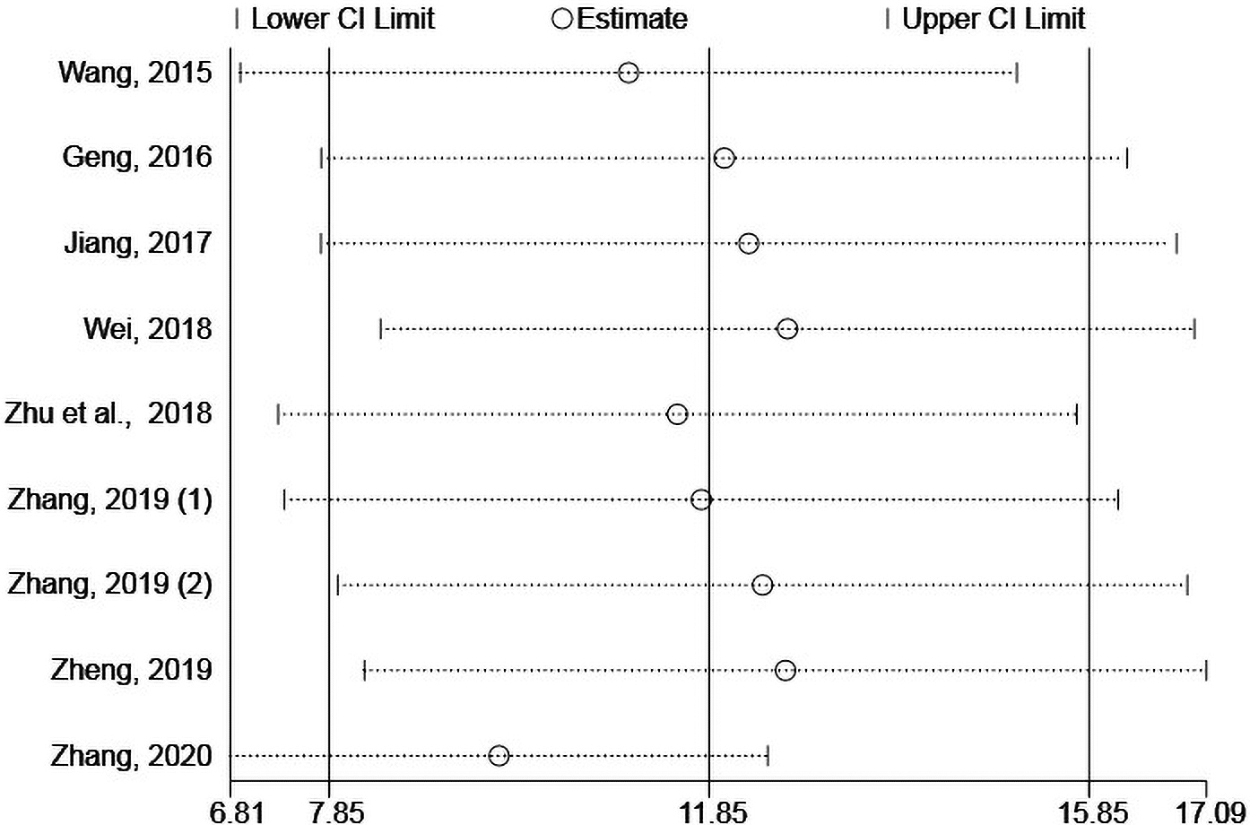
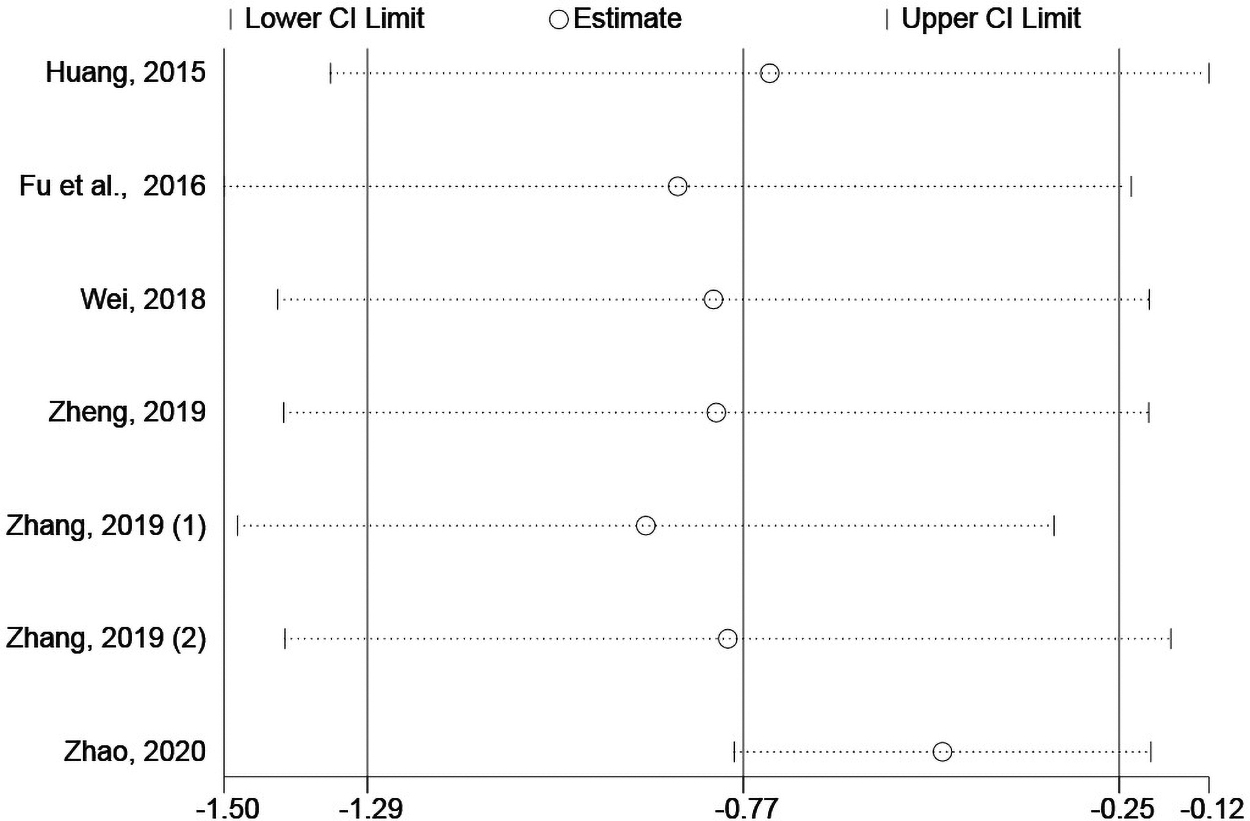
To further explore potential heterogeneity of anxiety and depression, sensitivity analysis was performed (Figs. 8 and 9, respectively). After removing one study (Zhao, 2020), we found that the heterogeneity of the measured outcomes of the two mental disorders decreased significantly, and the difference of synthetic overall effect did not change (p < 0.05), indicating that the sensitivity is high and the removed literature may cause heterogeneity. We considered this to be low-quality evidence due to imprecision and reporting bias; therefore, subgroup analysis was performed based on the gender of the participant, the type of drug abused, and the duration of intervention after removing the study (Zhao, 2020).
Sensitivity analysis of anxiety.
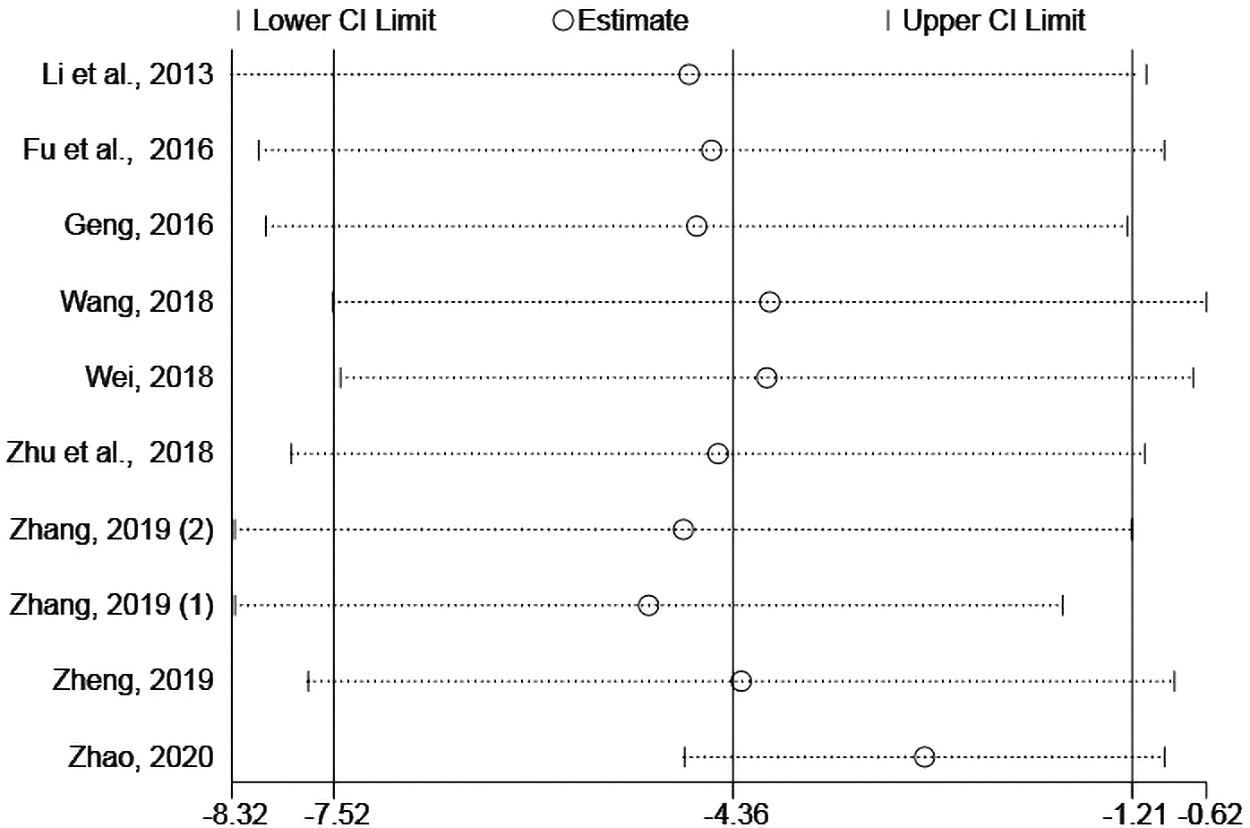
Sensitivity analysis of depression. To explore anxiety and depression, potential heterogeneity, sensitivity analysis was performed, as shown in Figures 8 and 9. After removing one study (Zhao, 2020), we found that heterogeneity is getting low, and the difference of synthetic overall effect has not changed (p < 0.05), indicating that the sensitivity is high and the removed literature may cause heterogeneity.
The I 2 values for heroin and meth were 39% and 36%, respectively, indicating that there was no obvious heterogeneity in either of the subgroups among the studies analyzed (Table 4). Therefore, the drug type was one of the sources of heterogeneity on anxiety. In addition, we also determined that the I 2 values for males and females were 41% and 0%, respectively, in the gender subgroup, whereas the I 2 values for heroin and meth in the drug subgroup were 40% and 42%, respectively, indicating that there was no obvious heterogeneity in any of the subgroups (Table 5). It also showed that the gender and drug type were the sources of heterogeneity when assessing depression. We did not use funnel plots to conclude publication bias because the number of studies included in each subgroup was not greater than 10.
Subgroup Analysis of the Differences in Anxiety Between the Experimental and Control Groups
CI, confidence interval; SMD, standardized mean difference.
Subgroup Analysis of Differences in Depression Between the Experimental and Control Groups
CI, confidence interval; SMD, standardized mean difference.
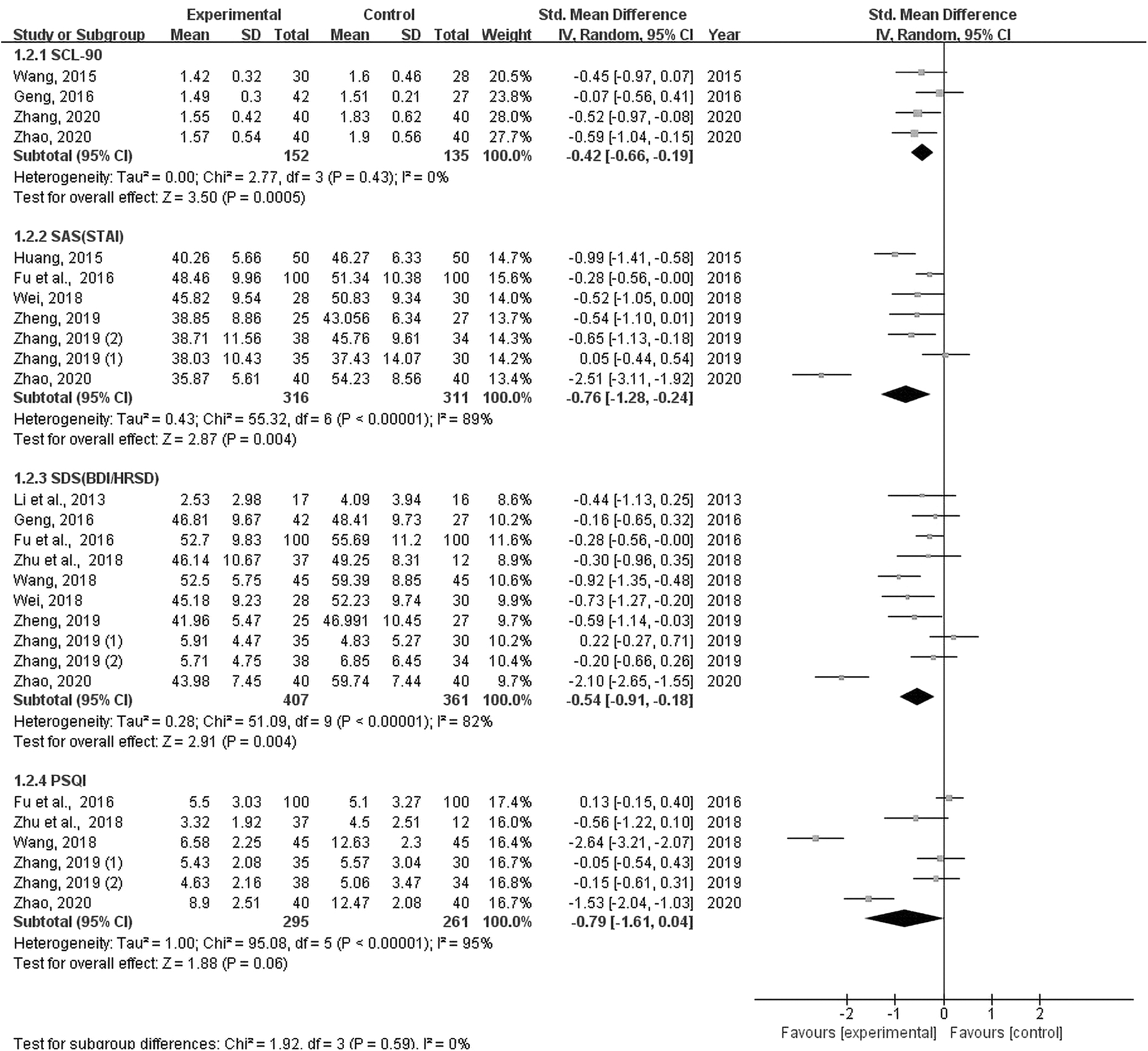
Above all, the results of the fixed model meta-analysis of the double-tailed test showed that the combined differences between groups of SCL-90 (p < 0.001), SAS (STAI) (p < 0.001), SDS (BDI/HRSD) (p < 0.001), and PSQI (p < 0.001) data were statistically significant (Fig. 10), indicating that long-term (12–24 weeks) TCE was effective for improving the mental health conditions and sleep status of drug addicts.
Forest plots of the effect sizes of TCE on psychological health after removing one study. The fixed model meta-analysis results of double-tailed test showed that the combined differences of multiple groups of SCL-90 (p < 0.001), SAS (STAI) (p < 0.001), SDS (BDI/HRSD) (p < 0.001), and PSQI (p < 0.001) were statistically significant, as shown in Figure. BDI, Beck Depression Inventory; HRSD, Hamilton Depression Rating Scale for Depression; PSQI, Pittsburgh Sleep Quality Index; SAS, self-rating anxiety scale; SCL-90, Symptom Check List; SDS, self-rating depression scale; STAI, State-Trait Anxiety Inventory; TCE, Traditional Chinese Health-Promoting Exercise.
Discussion
To the best of our knowledge, this meta-analysis was the first to comprehensively assess the effects of TCE on the physical and psychological health of drug addicts. The meta-analyses conducted in this review demonstrated that TCE was an effective adjunct therapy compared to no treatment or methadone therapy (control), leading to a reduction in SBP and DBP levels, while prolonging the duration during which the participants could stand on one leg with their eyes closed (balance). In addition, depression, anxiety, and sleep disorders were all greatly reduced among the drug addicts.
These results were supported by a systematic review, which also showed that Tai Chi and qigong exercises appeared to have the same positive effects on the improvement of depression and anxiety in individuals with substance abuse disorders. 17 However, we did not include resting heart rate in the main outcomes because the heart rate is less reflective of sympathetic activation of the heart. 32
We found that most studies that we used for meta-analysis were conducted in Chinese compulsory drug rehabilitation centers. In China, more than 780 drug maintenance treatment clinics have been set up throughout the country, with a total of 384,000 drug addicts participating in drug maintenance treatment. In addition, more than 300,000 drug addicts were isolated in 678 drug rehabilitation centers, but the rate of receiving rehabilitation treatment was <1.5%. 23 Therefore, finding effective treatment options and rehabilitation methods to alleviate withdrawal symptoms, promote mental health, and improve their quality of life remains an important concern.
As a cost-effective therapy, TCE is a widely accepted multimodal exercise modality with moderate intensity that focuses on psychosomatic training, which requires the coordination of the practitioner's mind and breathing using slow body movements during meditation. 34
Physical health is defined as a state in which a person's physical condition is suitable to carry out activities without restriction. Physical fitness is considered to be the most basic physical health condition needed to meet the needs of life and to complete all kinds of physical activities. At present, the blood pressure index is not only a necessary metric to assess physical fitness in any person but also is an important evaluation index of the progress of drug abusers' physical rehabilitation. In addition to physical deterioration, long-term drug use may cause serious damage to the brain, often resulting in physical discomfort, general weakness, weight loss, slow response to stimuli, difficulty moving, and unstable gait.
Therefore, in this study, the effect of TCE intervention on coordination and balance in the drug addicts was assessed by conducting blind, one-legged standing tests. This test is an evaluation of vestibular function because it requires maintaining a stable posture without visual references or external means of stabilization. Finally, BMI is an important health indicator that changes with age and other factors. 35 BMI is often used as a risk indicator for predisposing cardiovascular and metabolic diseases and certain cancers. 36 Therefore, we measured the effects of TCE intervention on BMI because drug ingestion is associated with both acute and chronic cardiovascular disease, including myocardial infarction and stroke.
The interactions between physical and mental health are apparent, that depressed people generally have lower physical activity levels than people without depression and lower physical activity levels also exacerbate depression resulting in a negative feedback cycle. 37 The mental health status of drug addicts in compulsory isolation is generally low. SCL-90 is a widely used scale to assess the mental health status, contributing to awareness of mental illness. 38 The SCL-90 scale is used to evaluate a broad range of psychological problems and symptoms based on nine dimensions, including somatization, interpersonal sensitivity, obsessive-compulsive behavior, anxiety, depression, phobic anxiety, paranoid ideation, hostility, and psychoticism. These nine dimensions are divided into 10 factors, which are mainly used to evaluate the mental health of subjects.
Because anxiety and depression are the two most common comorbidities in drug addicts, we used SAS and SDS as the main outcome indicators. In addition, because sleep disruption and poor sleep quality are common manifestations associated with drug addiction and withdrawal, the PSQI score was used to measure the extent of these symptoms. 39
According to the results of the meta-analysis, there were considerable heterogeneities in the data that explored the effect of TCE intervention on SBP (I 2 = 76%) and OS (I 2 = 68%). However, removing literature sources one by one to reduce the sensitivity did not reduce the heterogeneity (I 2 > 50%) of the main outcome indicators. The gender, drug type, and duration of intervention subgroups were then analyzed, the results of which showed that the homogeneity of the SBP data in the drug type subgroup and the OS data in the gender subgroup was low, indicating that the drug type and gender were sources of heterogeneity in SBP and OS data. Methamphetamine, which is a potent sympathomimetic drug with alpha agonist-like effects, increased SBP. 40 In addition, increased heart rate and blood pressure are known to occur after abrupt opioid withdrawal. 41
Psychological stress is a risk factor for hypertension and coronary artery disease. 42 TCE practitioners are required to keep their mind calm and remain relaxed during the exercises, which keeps the cerebral cortex in a highly orderly relaxed state, significantly reducing the excitability of the sympathetic nerve and improving the excitability of the vagus nerve. Twisting movements of the joint muscles can also accelerate venous reflux to improve blood circulation and peripheral vascular resistance for reducing blood pressure.
A previously published meta-analysis summarizing seven randomized control studies using Tai Chi exercises for TCE intervention showed that Tai Chi improved the participants' flexibility and stability, which helped to improve balance control and prevent falls. 43 Compared to other interventions or medical treatment, Tai Chi was more effective for preventing falls in frail and high-risk adults. 44 For the normal population, as they became older, the results of many balance indices were poor, 45 such that there was no difference in the balance index between men and women. 46 However, no literature has been published that concludes TCE plays a better role compared to ordinary exercise in promoting enhanced balance in men compared to women.
In this study, Tai Chi exercise did not have a positive effect on BMI, as there was no statistically significant difference in the BMI of participants before and after intervention (p = 0.76). However, changes in BMI might be dependent on the amount and intensity of the exercise. For low-to-moderate-intensity exercise used for risk control, increasing the amount of exercise might manifest a more significant effect on changes in BMI. The body weight of drug addicts in this study increased, resulting in an increase in the BMI index. This might have been related to the standardized schedule and diet management in the drug rehabilitation centers. It was also found that an intervention duration of 24 weeks had the best overall effect in improving SBP in male heroin addicts, while a duration of only 12–16 weeks had the best effect in improving OS in female meth addicts.
In addition, heterogeneity was also found when conducting meta-analysis of the psychological health outcomes among drug addicts. Heterogeneities were identified in the data corresponding to SAS (STAI) (I 2 = 89%), SDS (BDI/HRSD) (I 2 = 82%), and PSQI (I 2 = 95%). Following this, sensitivity analysis was performed, which identified that the heterogeneity of data significantly decreased after removing one study (Zhao, 2020). Subgroup analysis was then conducted based on gender, type of drug, and duration of intervention to explore the potential sources of heterogeneity, which showed that the drug type was one of the sources of heterogeneity in the anxiety data, while both gender and drug type were sources of heterogeneity in the depression data. Negative emotions, cravings, and withdrawal symptoms, which are considered risk factors for heroin relapse, might interact with each other. 47
The intensity of TCE intervention was moderate, and chronic moderate aerobic exercise has been shown to significantly stimulate the release of dopamine and norepinephrine, which can improve one's mood so as to relieve pain and make them feel comfortable during exercise. 48 Addicts are required to shift their attention from their unpleasant past experiences and their own illness to focusing on the fun of exercise to continuously transmit excitatory signals to the brain, stimulate a sense of pleasure, and promote the improvement of mood. The atmosphere of group training is relatively relaxed, so participants do not have a sense of tension and restraint, and the communication and mutual trust between participants can help improve communication and ultimately mental health.
In addition to drug and mental health treatment, exercise is typically used as an adjuvant treatment. Exercise can reduce the severity of sleep disorders, increase self-esteem, and reduce stress, all of which may help to reduce the risk of drug relapse. 49 One form of TCE, Taijiquan, can be a healthy exercise for people with sleep problems, but it should be done during the day, not at night. 50
It was also found that a Taijiquan intervention duration of 12–16 weeks had the best effect on improving anxiety in male heroin addicts, while a duration of 12–16 weeks had the best effect on improving depression in male heroin addicts. Compared to normal people or male addicts, female addicts more likely have a variety of psychological problems and poorer mental health. In addition, depression and anxiety are more common among women compared to men. 51 When physical health and emotional state were factored into demographic, health behavior, and work status variables, the relationship between sleep and BMI was found to be irrelevant. 52
This meta-analysis has several limitations. First, it was predominantly based on randomized, controlled studies. The sample sizes of most of the studies were small, which affected the ability to identify statistical differences. Second, regarding outcome results, publication bias might be a worrying issue. However, the bias could not be tested due to the small number of studies contained in the bias sample. Third, the studies analyzed were solely derived from China because Tai Chi and healthy qigong are more popular and recognized by Asian people. 53 These exercises are not nearly as popular among non-Chinese people, so it is difficult to assess the impact of this population difference. Moreover, the TCE crowd is mainly concentrated in rehabilitation centers, so more research is needed to quantify the benefits of long-term practice for drug addicts after returning to society.
Conclusions
This is the first study to systematically examine the effects of TCE on the physical and mental health of drug addicts isolated in drug rehabilitation centers in China. As an effective mind-body movement intervention, we concluded based on the systematic, statistical analysis of several studies that long-term TCE is beneficial to the physical and mental health of drug addicts. The specific intervention methods were dependent on the gender of the drug addict and the drug type, and longer intervention times had a greater impact on physical health. Long-term TCE intervention and the formation of a healthy physical lifestyle are vital for helping addicts quit illicit drug use and prevent relapse.
Footnotes
Authors' Contributions
D.J. and Y.X. contributed to the conceptualization and design of the review; D.J. applied the search strategy; J.Z. and D.J. applied the selection criteria; J.Z. and D.J. completed the assessment of risk bias; and D.J. and Y.X. wrote, reviewed, and edited the article. All authors analyzed and interpreted the data. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Key Medical Disciplines of Hangzhou and the 2022 Soft Science Research Program of Zhejiang Province (2022C35056).
Supplementary Materials
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.