
Abstract
Introduction:
Gastrointestinal immobility is experienced by many patients who undergo gastric surgery. This complication delays enteral nutrition, prolongs hospitalization, and causes discomfort. Acupoint stimulation is a popular alternative nonpharmacological treatment for gastrointestinal immobility. This study aimed to explore the effects of acupoint stimulation on gastrointestinal immobility after gastrectomy.
Design:
Systematic review and meta-analysis.
Methods:
Databases (PubMed, Cochrane, Joanna Briggs Institute EBP Database, Medline, CINAHL Complete, and Airiti library) were searched from their inception to April 2022 for relevant articles. Articles in Chinese and English were included, without limitations on year, region, or country. The inclusion criteria were studies with participants >18 years of age, postgastric surgery, and hospitalization. In addition, randomized controlled trials (RCTs) were included. Data were analyzed using random effects models, and data heterogeneity was investigated using subgroup analysis. Meta-analysis was performed using Review Manager 5.4 software.
Results:
We included 785 participants from six studies. Invasive and noninvasive acupoint stimulation reduced the time of gastrointestinal mobility better than usual care. In the control group, the time of first flatus was 43.56 ± 9.57 h to 108 ± 19.2 h, and the time of first defecation was 77.27 ± 22.67 h to 139.2 ± 24 h. In the experimental group, the time of first flatus and defecation was 36.58 ± 10.75 h to 79.97 ± 37.31 h and 70.56 ± 15.36 h to 108.55 ± 10.75 h, respectively. Subgroup analysis showed that invasive acupoint stimulation with acupuncture reduced the time of first flatus and defecation to 15.03 h (95% confidence interval [CI] = −31.06 to 1.01) and 14.12 h (95% CI = −32.78 to 4.54), respectively. Noninvasive acupoint stimulation, including acupressure and transcutaneous electrical acupoint stimulation (TEAS), reduced the time of first flatus and defecation to 12.33 h and (95% CI = −20.59 to −4.06) and 12.20 h (95% CI = −24.92 to 0.52), respectively.
Conclusions:
Acupoint stimulation improved the gastrointestinal immobility of postgastrectomy. In the included RCT articles, invasive and noninvasive stimulations were effective. However, noninvasive acupoint stimulation, such as with TEAS and acupressure, was more efficient and convenient than invasive stimulation. Overall, health care professionals with adequate training or under the supervision of an acupuncturist can effectively perform acupoint stimulation to improve the quality of postgastrectomy care. They can select commonly used and effective acupoints to enhance gastrointestinal motility.
Clinical relevance:
Acupoint stimulation, such as acupressure, electrical acupoint stimulation, or acupuncture, can be included in postgastrectomy routine care to improve gastrointestinal motility and reduce abdominal discomfort.
Introduction
In Taiwan, 41,014
Vagotomy causes loss of antral contraction and pyloric relaxation, leading to food retention in the stomach. 9 Patients experienced constipation, diarrhea, abdomen fullness, nausea, and vomiting; however, bowel obstruction is absent. In usual care, the time of first flatus is 43.56 ± 9.57 h to 108 ± 19.2 h, and the time of first defecation is 77.27 ± 22.67 h to 139.2 ± 24 h. 10 –15 These complications delay enteral nutrition, prolong hospitalization, and cause discomfort to the patients. Patients usually require a nasojejunal or jejunostomy tube when oral intake is insufficient. Parenteral nutrition is used when enteral feeding is not tolerated. 7
In the clinical setting, the general management principles for gastrointestinal immobility include maintenance of hydration, electrolyte balance, correction of nutritional deficiency, and dietary modifications. In addition, pharmacological treatments include prokinetic agents (metoclopramide and domperidone), tricyclic antidepressants, and erythromycin. 3,9 However, a randomized control trial (RCT) showed that erythromycin did not significantly improve bowel function compared with a placebo. 16,17 Moreover, pharmacological treatment is not an optional method for treating this complication and has many side effects, including extrapyramidal symptoms with metoclopramide (61%), hypoglycemia with domperidone (41%), and severe reaction to tricyclic antidepressants (40%). 3 Consequently, nonpharmacological remedies, such as acupoint stimulation, can be used as a complementary therapy.
Acupoint stimulation is a modality of Chinese medicine based on modulating the yin/yang and qi/blood in the body's meridians. The yin/yang, qi/blood, and five elements form basic pathology and physiology in Chinese medicine. 18 In humans, the qi is the yang, and the blood is the yin; these are separate circulatory systems that work together in balance. 18 Moreover, the Jin Luo is a pathway that transports energy around the body, and many acupoints along this pathway are on the body's surface. 18 Acupuncture can correct the imbalance of yin and yang by adjusting the qi/blood Jin Luo of the body's meridians. De qi sensations reflect acupuncture efficiency and include soreness, numbness, distention, heaviness, and other sensations. 13,18 The mechanisms of acupuncture include the activation of descending pain inhibitory systems, internal organ system modulation, and immune modulation.
Acupuncture at a single location can induce responses in different brain regions and, at different acupoints, elicits different cerebral activity changes. 19 The seed-base functional connectivity of ST-36 (Zusanli) can increase the endogenous analgesia functional network. 20 Similarly, other acupoints, including GB-37 (Guangming), PC-6 (Neiguan), and PC-7 (Daling), can influence cerebral functional connectivity. 19 Fibroblasts and endothelial cells are mechanical adhesions in the extracellular collagen matrix and intracellular cytoskeleton. When the acupuncture needle rotates, a mechanical signal is transduced to connective tissue and increases the extracellular concentrations of purines, adenosine, and ATP metabolites. 18
Acupoint stimulation, such as in acupuncture, transcutaneous electrical acupoint stimulation (TEAS), and acupressure, can improve gastrointestinal dysfunction. 21 The mechanisms involve activating large myelin nerve fibers, including the vagus nerve, releasing γ-aminobutyric acid, adenosine, and nitric oxide, which alleviate pain. This reduces anesthetic dosage, 22,23 releases motilin to increase small bowel motility, 15 and decreases inflammatory processes through the cholinergic anti-inflammatory pathway. 24 Notably, research results have been inconsistent; therefore, this study aimed to conduct a meta-analysis to explore the effects of acupoint stimulation in improving gastrointestinal motility after gastrectomy.
Methods
Search strategy and study selection
We systematically searched electronic databases, including PubMed, Cochrane, the Joanna Briggs Institute EBP Database, Medline, CINAHL Complete, and Airiti library. Studies were retrieved from the inception of each database until April 2022. Keywords, MeSH terms, and truncation symbols were applied in the search strategy, including “Gastrectomy”[Mesh] AND “Acupressure”[Mesh] OR “Acupuncture”[Mesh] OR “Acupuncture Therapy”[Mesh] OR “Acupuncture Points”[Mesh] OR “Acupuncture, Ear”[Mesh] OR “Meridians”[Mesh] OR “Electroacupuncture”[Mesh] OR “Qi”[Mesh] OR “stimulate certain point” OR “electrical acupoint stimulation” OR “transcutaneous electric nerve stimulation”; Gastre* AND Acup*. In addition, language was restricted to Chinese or English, without year and country limitations.
First, we screened retrieved titles and abstracts retrieved for relevant studies. Next, we reviewed the articles' contents and included or excluded texts that conformed to the inclusion or exclusion criteria and outcomes. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses search and screening strategies. The inclusion criteria were (1) studies with participants >18 years of age and postgastric surgery and hospitalized patients; (2) RCTs; (3) studies comparing the effect of acupoint stimulation and routine care; and (4) studies with outcomes comprising a time of first flatus and defecation. The exclusion criteria were as follows: (1) studies reporting gastrectomy combined with other surgeries; (2) articles discussing gastric immobility prevention; (3) reports on participants with diabetic gastroparesis; (4) articles with no full text; and (5) protocol and pilot studies.
Data extraction
We extracted data from original reports using (1) year of publication; (2) country; (3) study design; (4) sample characteristics (sample size and population type); (5) type of intervention (acupuncture, acupressure, and TEAS); and (6) comparison groups and results (“time of first flatus” and “time of first defecation”). Two independent reviewers conducted the literature search, data extraction, and quality assessment, and a third reviewer was included when inconsistencies remained after discussion. All data were managed by importing them into Endnote 20.
Risk-of-bias assessment
The Cochrane Collaboration tool 25 was used to assess the risk of bias of the included RCTs. The six domains in this tool include random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. The domains were classified as “low risk,” “unclear risk,” and “high risk” based on the assessment. Besides acupoint stimulation, the study designs included sham-TEAS 10 and sham-electroacupuncture. 13 However, blinding the intervention provider was difficult in these studies because they always knew who received acupoint stimulation. Nevertheless, performance bias was not the main focus of our study; hence, the articles were not excluded, despite being unblinded.
Statistical analysis
Review Manager 5.4 software was used to synthesize the extracted data. The various acupoint stimulations, including acupuncture, TEAS, or acupressure, are independent variables. The heterogeneity of results across studies was assessed using the I 2 statistic. I 2 values <30% and >50% were considered mild and notable heterogeneities, respectively, 26 and a random effects model was adopted if I 2 was ≥50%. Finally, subgroup analyses were performed based on the type of acupoint stimulation (invasive or noninvasive) and comparison group (usual care).
Results
Search results and included studies
The initial search resulted in 305 studies. Next, 284 studies were retained after removing duplicate documents. Next, after reviewing titles and abstracts, we excluded 276 documents. Afterward, eight studies were selected for full-text review, and only six RCTs were finally included. The screening process followed the PRISMA guidelines (Fig. 1).
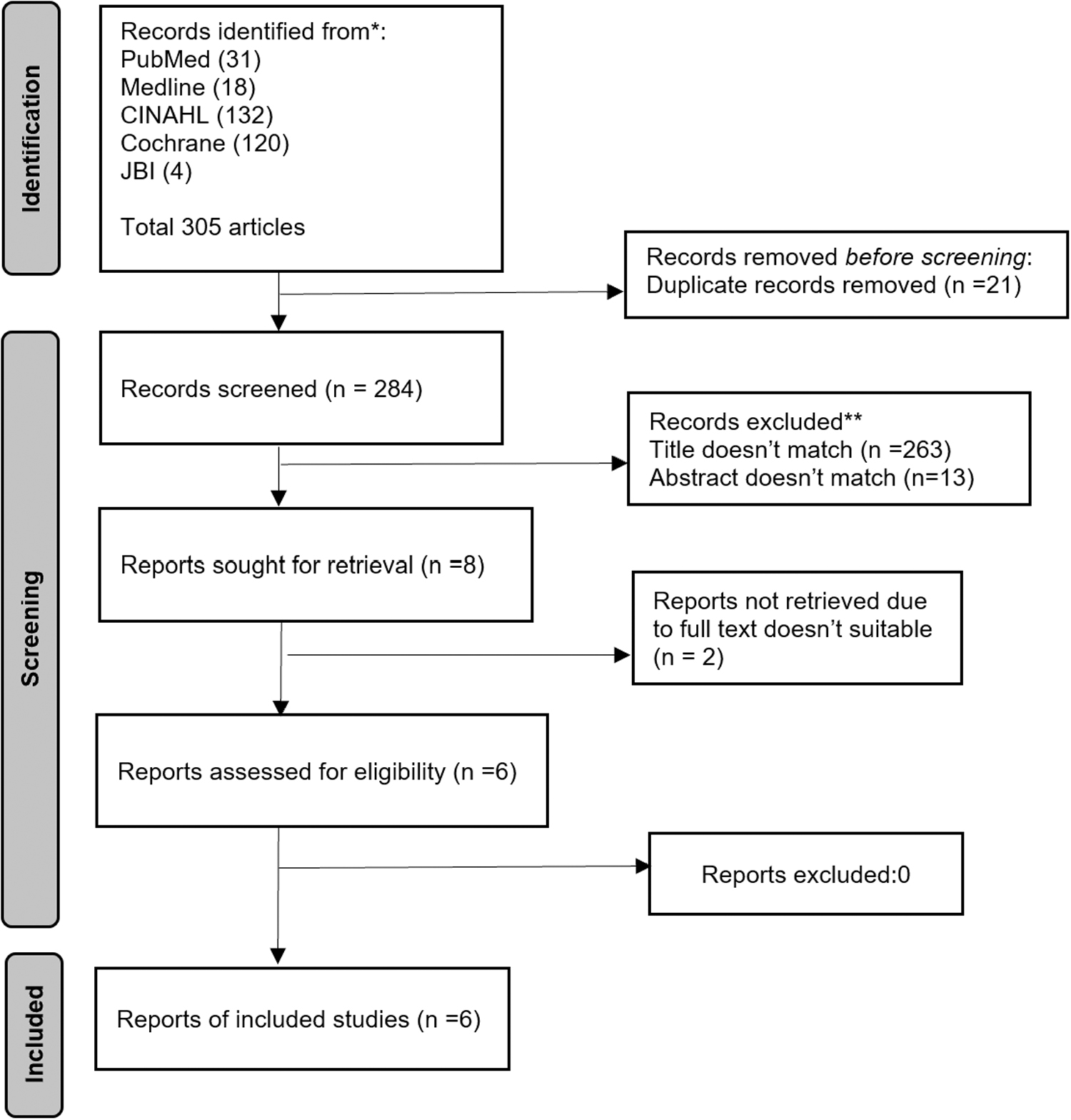
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart describing the selection process.
The included articles were from Taiwan, China, and Korea. In the six articles, 785 participants received gastrectomy, 403 received acupoint stimulation, and the others received usual care. Moreover, the acupoint stimulation was invasive (acupuncture) and noninvasive (acupressure and TEAS). In addition, of the six articles, one included acupressure, 11 two included TEAS, 10,15 and the others included acupuncture 12 –14 (Table 1). The providers were fully trained acupuncturists (with an average of 15 years of practice and experience), 13 researchers who received training in Traditional Chinese Medicine, 11 nurses and surgeons who received acupuncture training, 14 and doctors of Traditional Chinese Medicine. 12 Each article used the two acupoints ST-36 and PC-6.
Characteristics of Studies Included in Meta-Analysis
All the articles are randomized controlled trials; time is represented by (mean ± SD).
The acupoints were bilateral Zusanli (ST-36), Sanyinjiao (SP-6), Hegu (LI-4), Ziagou (TE-6), Taichong (LV-3), and Quchi (LI-11), and unilaterally at Baihui (GV-20), Yintang (EX-HN3), Shuigou (GV-26), and Chengjiang (CV-24).
TEAS, transcutaneous electrical acupoint stimulation.
The main result was “time of first flatus” and “time of first defecation.” Some patients had first flatus and defecation after gastrectomy. In the control group, the time of first flatus was 43.56 ± 9.57 h to 108 ± 19.2 h, and the time of first defecation was 77.27 ± 22.67 h to 139.2 ± 24 h in the control group. In the experimental group, the time of first flatus was 36.58 ± 10.75 h to 79.97 ± 37.31 h, and the time to first defecation was 70.56 ± 15.36 h to 108.55 ± 10.75 h. 10 –15 We used the random effects models and subgroup analysis, such as differentiating invasive and noninvasive acupoint stimulation, due to high heterogeneity (I 2 = 92%, 93%).
Overall, 125 participants received noninvasive acupoint stimulation (TEAS and acupressure), and 127 received usual care. Furthermore, noninvasive acupoint stimulation significantly decreased the time of first flatus and defecation to 12.33 h (95% confidence interval [CI] = −20.59 to −4.06) and 12.2 h (95% CI = −24.92 to 0.52), respectively. Moreover, 278 participants received invasive acupoint stimulation (acupuncture) and 255 received usual care. Acupuncture significantly decreased the time of first flatus and defecation to 15.03 h (95% CI = −31.06 to 1.01) and 14.12 h (95% CI = −32.78 to 4.54), respectively. Overall, acupoint stimulation decreased the time of first flatus to 14.22 h (95% CI = −23.17 to −5.26) and that of first defecation to 13.14 h (95% CI = −23.84 to −2.45) (Figs. 2 and 3).
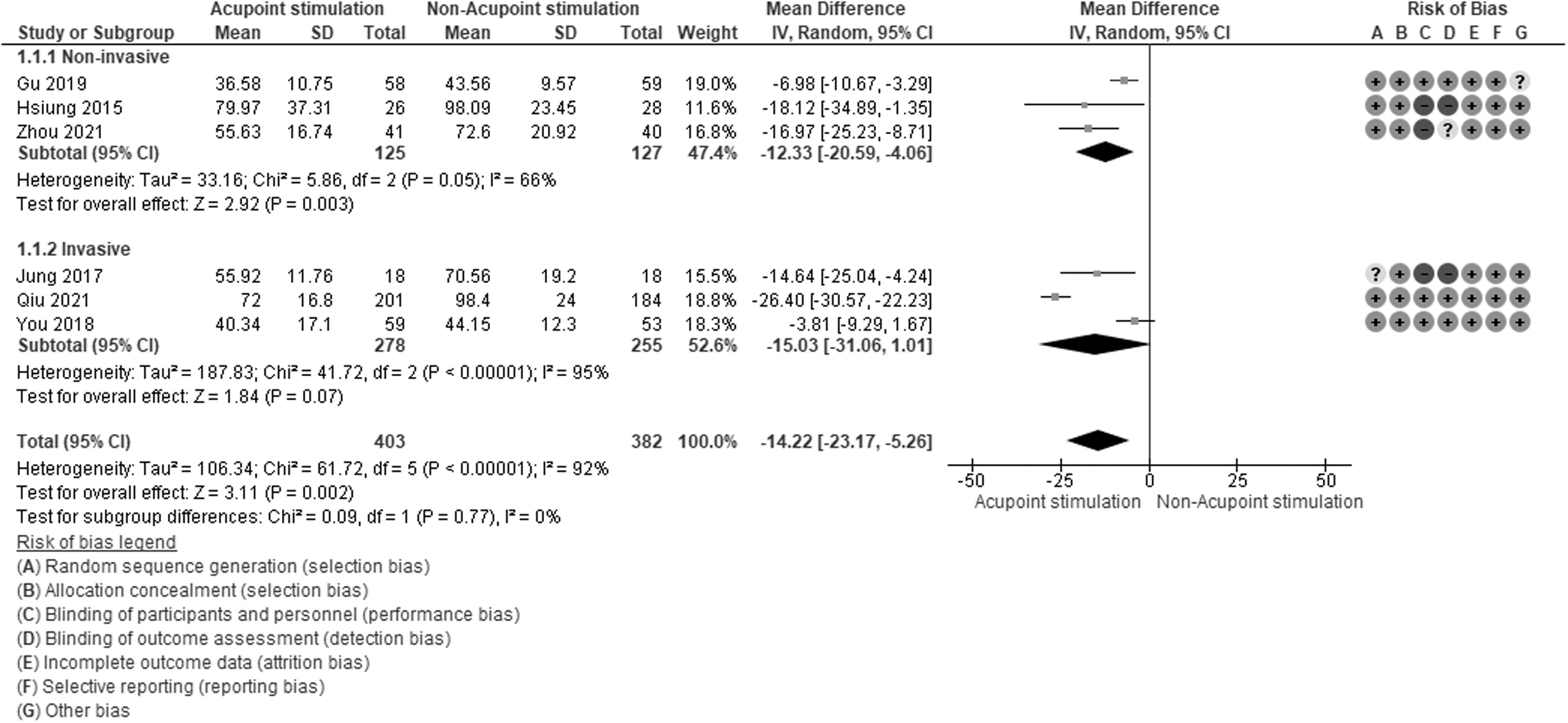
Forest plot of the meta-analysis illustrating the overall weighted effect size of acupoint stimulation includes invasive and noninvasive to reduce time to first flatus (h) in patients after gastrectomy. The diamond on the bottom of the forest plot represents the overall weighted estimate. CI, confidence interval.
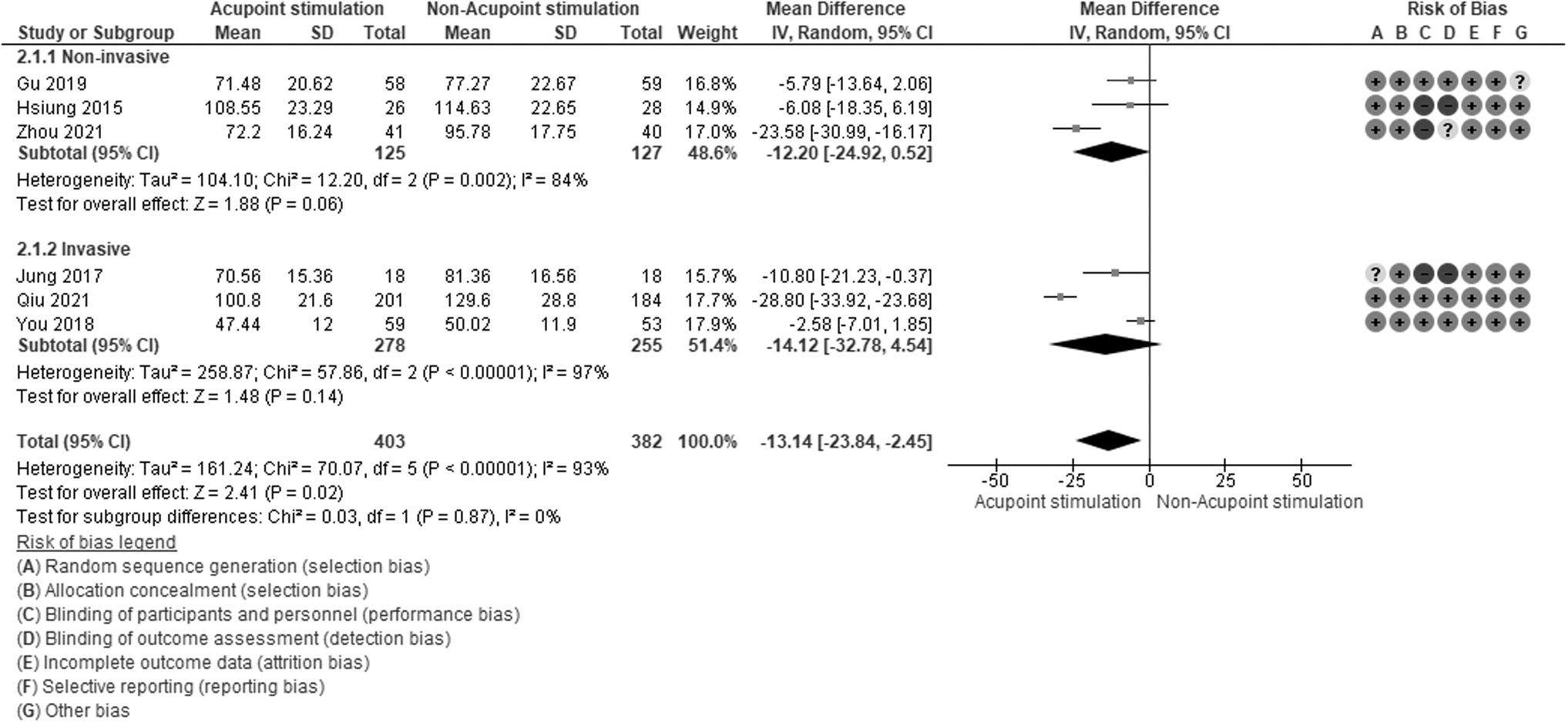
Forest plot of the meta-analysis illustrating the overall weighted effect size of acupoint stimulation includes invasive and noninvasive to reduce time to first defecation (h) in patients after gastrectomy. The diamond on the bottom of the forest plot represents the overall weighted estimate. CI, confidence interval.
Discussion
We found that acupoint stimulation could improve gastrointestinal motility, consistent with a previous meta-analysis. 27 Acupoint stimulation reduced the time of first flatus and defecation to 14.22 and 13.14 h, respectively, compared with usual care, where time to first flatus and defecation was 43.56 ± 9.57 h to 108 ± 19.2 h and 77.27 ± 22.67 h to 139.2 ± 24 h, respectively. 10 –15 This indicates that acupoint stimulation is an effective alternative therapy in clinical care; it may help patients recover gastrointestinal mobility, improve appetite and nutrition, and reduce abdomen distention and hospitalization. The acupoints ST-36 and PC-6 were stimulated in all articles; other acupoints used are listed in Table 1. We used subgroup analysis to compare the effects of invasive and noninvasive acupoint stimulation. Noninvasive acupoint stimulation, such as acupressure and TEAS, improved gastrointestinal motility and was better than invasive acupoint stimulation.
Notably, real acupoint stimulation, such as TEAS and hand needling combined with electroacupuncture, shows significant improvement in gastrointestinal motility compared with sham acupoint stimulation. 10,13 Therefore, acupoint stimulation effectively improves gastrointestinal motility after gastrectomy. Overall, in usual care, the time to first flatus and defecation was 1.4–5 days and 2.2–6.8 days, respectively; acupoint stimulation reduced this time by >12 h, thereby improving discomfort, reducing patient stress, and enabling the early establishment of nutrients through the gastrointestinal tract.
The six RCTs included had reference appraisals of 4–7 points. Moreover, low-risk performance and detection biases were 50% (Figs. 4 and 5), and it was difficult to blind participants and investigators. A systematic review of data from participant with diabetic gastroparesis included 32 studies; however, only one was blinded. 27 In this review, participants, data collectors, nurses, and data analysts were blinded in one article. Another study on sham acupoint stimulation was blinded. 10,13,14 We rated these as having a low risk of performance bias.
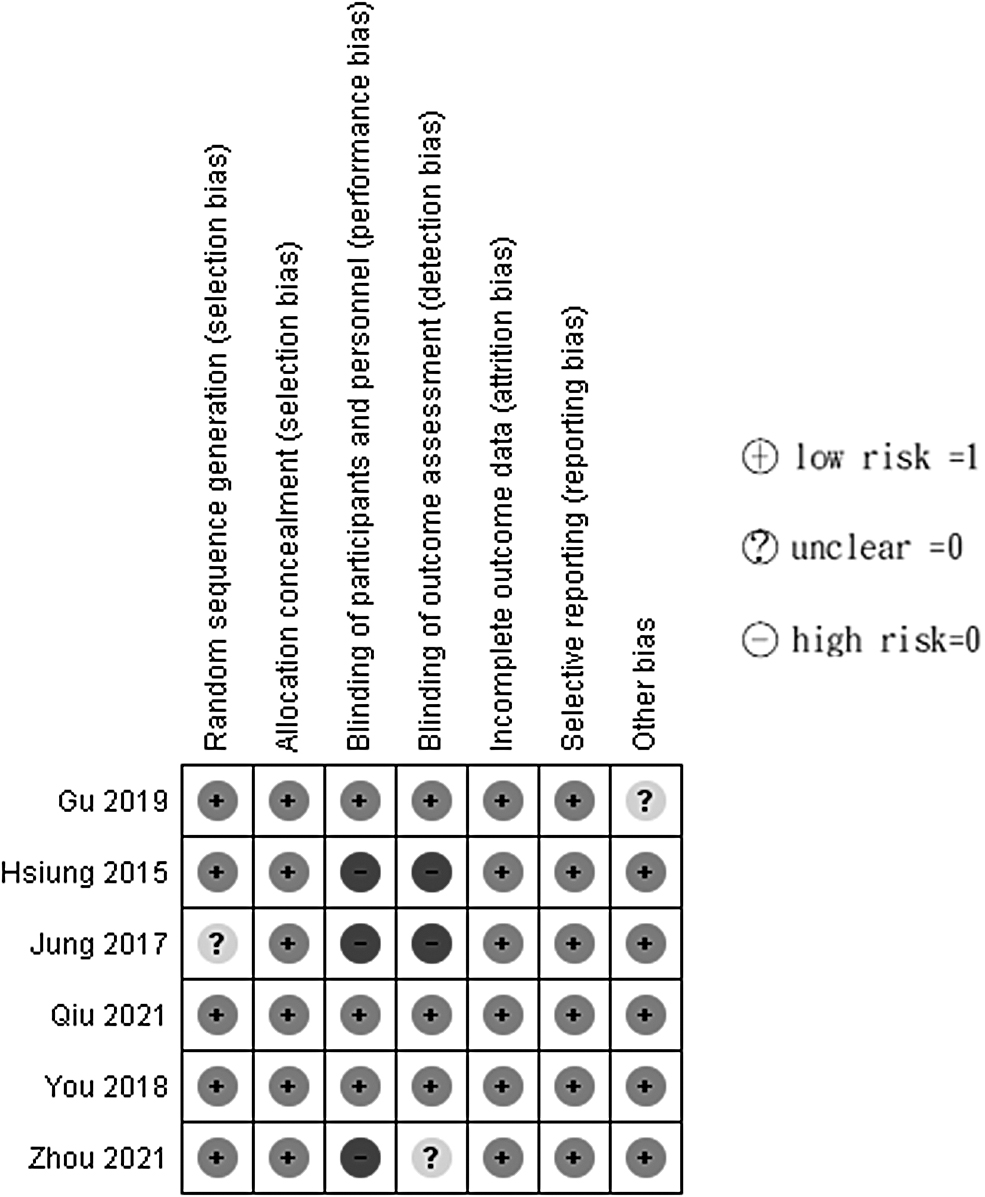
Risk of bias graph for included study.
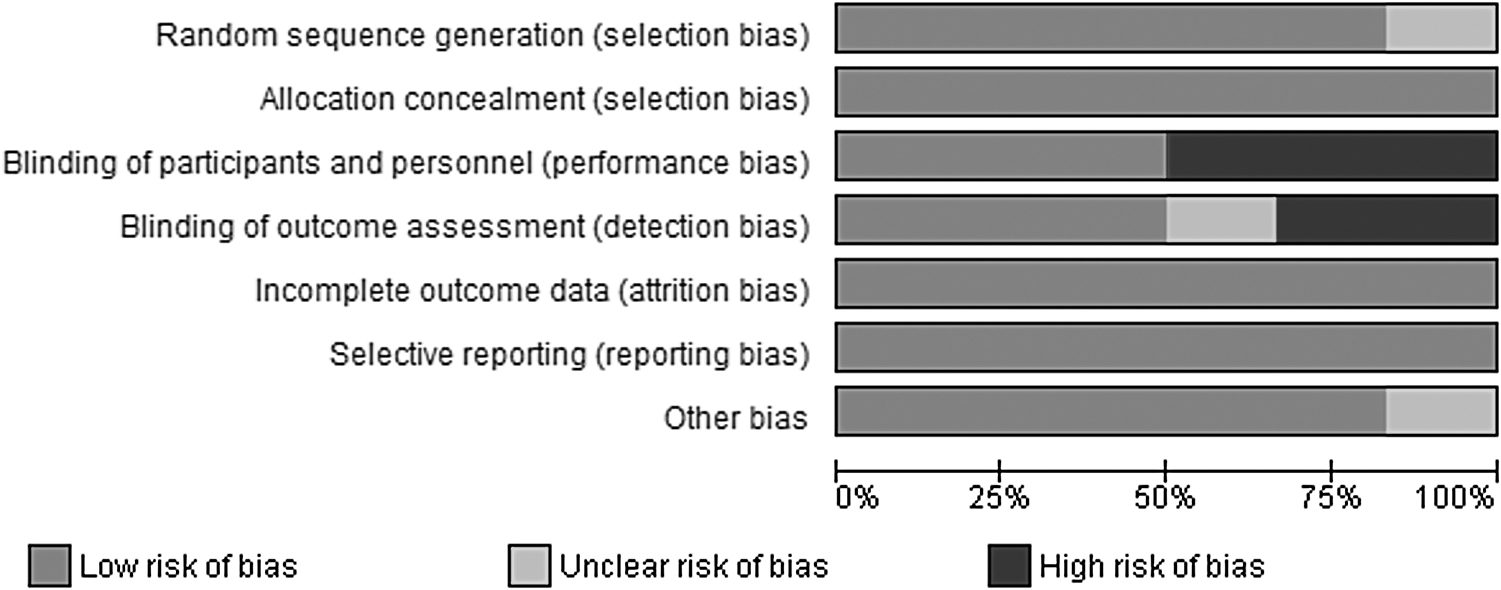
Risk of bias summary for all graphs.
This systematic review confirmed that acupoint stimulation was better at improving bowel movement than usual care. The reduction in the time to first flatus and defecation after gastrectomy is possibly due to the release of motilin, which increases small bowel motility. 15 These results are consistent with a previous study that performed acupuncture at 3 and 5 days postoperatively and identified using abdominal radiograph that the number of remnant Sitz marker capsules that moved forward decreased in the small bowel. 12 Another study showed that TEAS could promote bowel activity after gastrointestinal surgery, 28 and plasma motilin concentrations were significantly increased in a TEAS group. 29
This study had high heterogeneity due to varying acupoint stimulations; therefore, we classified the studies according to the pathway of acupoint stimulations: invasive and noninvasive, including acupuncture, 12,14 acupressure, 11 TEAS, 10,15 and electroacupuncture. 13
Moreover, we performed a subgroup analysis, Noninvasive acupoint stimulation significantly decreased the time to flatus and defecation more than invasive acupoint stimulation. Acupoints were chosen all over the body, and acupuncture angle, depth, and maneuver were different for individuals. Nevertheless, there were still differences. Notably, consistency among different operators was challenging when implementing the intensive acupuncture treatment. For example, a 0.25 × 30 mm needle was used for acupuncture on Zusanli in a patient with a normal BMI and 0.30 × 40 mm for overweight patients. 14 Furthermore, the “de qi” is a subjective sensation (feeling of soreness, numbness, warmth, heaviness, or distention around the area) when acupuncture is on the correct acupoint. 10,14
TEAS contacts a broader area than acupuncture, places lead on the acupoint region, and sets current strength for acupoint stimulation. Moreover, compared with acupuncture, TEAS intensity can be adjusted according to the patient's tolerance, improving its acceptability by patients. Therefore, TEAS would be better than acupuncture in improving gastrointestinal motility. Overall, acupoint stimulation is effective and safe. No adverse reaction was observed during the TEAS and acupuncture. 12,15
In addition, in the electroacupuncture group (n = 385), only one patient complained of dizziness, and no skin injury or hemorrhage was observed. 13 The acupoints that can improve gastrointestinal motility—PC-6 and ST-36—appeared in every article. PC-6 is located on the palmar aspect of the forearm, with the forearm and palm facing upwards; it is 2 cun (5 cm) above the wrist crease, between the tendons of the long palmar muscle and the radial flexor muscle of the wrist. ST-36 is located on the lower leg, 3 cun (7.5 cm) below the knee and about 0.5 cun (1.5 cm) from the anterior crest of the tibia when sitting with the foot in a relaxed, dropped-down position.
These acupoints can balance both qi and blood, enhance the regularity of gastric myoelectric activity, modulate digestive function, and relieve gastrointestinal discomfort, leading to improved digestive function. 10,11 Regarding acupoints, health care professionals who are not acupuncturists maybe can provide acupoint stimulation to patients by identifying commonly used and effective acupoints, such as ST-36 and PC-6, for enhancing gastrointestinal motility. They can receive appropriate training and guidance from acupuncturists to ensure safe and effective treatment.
This study had some limitations. First, the study had high heterogeneity due to different acupoint stimulation methods; although the operators were professional, the acupoint stimulation technique differed. Therefore, we performed a subgroup and random effect model analyses to determine their effects. in addition, the number of RCTs on acupoint stimulation methods was insufficient for a meta-analysis. Consequently, we combined the acupoint stimulation methods into invasive and noninvasive to compare the effects. In the future, we will compare individuals to know which acupoint stimulation technique is effective. Moreover, we focused on only gastrectomy-induced gastrointestinal immobility and compared time to flatus and defecation; this provided a short-term effect and benefits of different acupoint stimulation methods. Therefore, studies assessing long-term effects over 4–12 weeks are needed to confirm the benefits of acupoint stimulation in gastrointestinal discomfort.
Furthermore, these original studies were conducted in Asia, including Chinese, Taiwanese, and Korean patients; therefore, these results may not be generalizable to other regions. Therefore, studies recruiting more diverse populations will be needed. Finally, the providers knew who received acupoint stimulation; therefore, performance bias was difficult to prevent. Nevertheless, this study provided statistical evidence that acupuncture stimulation is effective in enhancing gastrointestinal motility after gastrectomy. In clinical practice, we should consider patients' emotions and expectations, in addition to treatment effectiveness. To optimize the implementation process and prioritize patient-centered care, future research should include qualitative studies to emphasize patient experiences.
Conclusions
Acupoint stimulation improved gastrointestinal motility after gastrectomy. By selecting the corresponding acupoints for gastrointestinal function and stimulating them, the balance of qi, blood, yin-yang, and physiological mechanisms of meridians can be regulated to improve gastrointestinal motility after gastrectomy. Noninvasive acupoint stimulation, such as TEAS and acupressure, was more effective than invasive acupoint stimulation. Acupoint simulation techniques can be implemented without complex and expensive equipment in clinical settings. However, acupoint stimulation requires training, and only well-trained health professionals can perform this procedure to improve the quality of postgastrectomy care. Nevertheless, this study provides statistical evidence that acupuncture stimulation is effective in enhancing gastrointestinal motility after gastrectomy. In clinical practice, besides effectiveness, we should also consider patients' emotions and expectations. To optimize the implementation process and prioritize patient-centered care, future research should include qualitative studies to emphasize patient experiences.
Footnotes
Acknowledgment
The authors would like to thank Dr. Lok-Hi Chow, Anesthesiologist of Taipei-Veterans General Hospital, Taiwan, for valuable advice on the mechanism of acupoint stimulation and systematic review methodology.
Authors' Contributions
Y.-L.C. developed the research framework and search strategy and performed study selection, data extraction, quality assessment, methodology, and statistical analysis, and wrote the initial draft of the article. T.-F.H. carried out the methodology, analyses, and article writing and revision. Y.-Y.K. provided advice on the mechanisms of acupoint stimulation and systematic review methodology and revised the article. Y.-C.C. developed the research framework, conducted the literature search, data extraction, and quality assessment, and contributed to writing, review, and editing of the article. All authors reviewed and approved the article before submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.