
Abstract
Objectives:
Prevalence of irregular menstrual cycle ranges from 81.7% to 96.3%. Recent research suggested that homeopathy is one of the most popular choices for women with various gynecological disorders. This trial was aimed at differentiating individualized homeopathic medicinal products (IHMPs) from identical-looking placebos in the treatment of menstrual irregularities in early reproductive women.
Design:
Double-blind, randomized (1:1), two parallel arms, placebo-controlled trial.
Setting:
D. N. De Homoeopathic Medical College & Hospital, Kolkata, West Bengal, India.
Subjects:
Ninety-two females with menstrual irregularities.
Interventions:
Group verum (n = 46; IHMPs plus concomitant care) versus group control (n = 46; placebos plus concomitant care).
Outcome Measures:
Primary—The proportion of early reproductive females in whom menstrual irregularities can be corrected for consecutive three cycles; Secondary—Menstrual Distress Questionnaire (MDQ) total score; all of them were measured at baseline and every month, up to 4 months.
Results:
Intention-to-treat sample (n = 92) was analyzed. Group differences were examined by chi-squared tests with categorical outcomes, two-way repeated measure analysis of variance accounting for the time–effect interactions, and unpaired t-tests comparing the mean estimates obtained individually every month. The level of significance was set at p < 0.05 two-tailed. After 4 months of intervention, the group difference in the primary outcome was nonsignificant statistically—IHMPs: 22/46 v/s placebo: 24/46, chi-square (Yates corrected) = 0.043, p = 0.835. The improvement observed in the MDQ total score (F 1,90 = 0.054, p = 0.816) and subscales scores were higher in the IHMPs group than in placebos, however statistically nonsignificant in most of the occasions, except for the behavioral change subscale (F 1,90 = 0.029, p < 0.001). Pulsatilla nigricans was the most frequently prescribed medicine. Kent’s Repertory and Zandvoort’s Complete Repertory were the most frequently used repertories. No harm or serious adverse events were reported from either group.
Conclusions:
The analysis failed to demonstrate clearly that IHMPs were effective beyond placebos in all but one of the outcomes. More appropriate outcome measures may be sought for future trials.
Clinical Trial Registration Number:
CTRI/2022/04/041659.
Introduction
Menstruation is the visible manifestation of cyclic physiologic uterine bleeding owing to the shedding of the endometrium following the invisible interplay of hormones mainly through the hypothalamic–pituitary–ovarian axis. 1 This monthly experience by females is a significant tool for assessing normal development and ruling out pathological conditions, and it is one of the determinants of a woman’s reproductive health. 2 The duration of menstruation is about 4–5 days, and the amount of blood loss is estimated to be 20–80 mL with an average of 35 mL. 1 The onset of menstruation is governed by a girl’s general health condition, and genetic, socioeconomic, and nutritional factors, and is coordinated by the actions of the hypothalamic–pituitary–ovarian axis. 3 However, 14%–25% of women have irregular menstrual cycles (International Classification of Diseases, Tenth Revision: N92.6), meaning the cycles are shorter or longer than normal, are heavier or lighter than normal, or are experienced with other problems, such as abdominal cramps. Irregular cycles can be ovulatory, meaning that ovulation occurs, or anovulatory, meaning ovulation does not occur. The most common menstrual irregularities include amenorrhea, oligomenorrhoea, puberty menorrhagia, prolonged menstrual bleeding, metrorrhagia, menometrorrhagia, and dysmenorrhea. Additional menstrual irregularities include polymenorrhagia, irregular menstrual periods, shortened menstrual bleeding, and intermenstrual bleeding. The prevalence of menstrual disorders has been recorded as high as 85.0%–93.4% in India. 4 –7 Prevalence of irregular menstrual cycle ranges from 81.7% to 96.3% and absenteeism from school owing to menstrual discomfort ranges from 63.5% to 80.6%, which was found in a study in West Bengal. 8
Homeopathy is a holistic approach to medicine, emphasizing the treatment of the whole person rather than just the symptoms of a specific disease. In the case of menstrual irregularities, a homeopathic practitioner would typically take into account not only the physical symptoms but also the mental and emotional state of the individual. This is known as considering the “totality of symptoms” when using mostly Kent’s repertory, 9 and modern repertories developed on Kent’s philosophy. 10,11 The process of choosing a homeopathic remedy involves fully assessing the individual’s symptoms. Different causes of menstrual irregularities have to be understood properly from their basic presenting symptoms in day-to-day practice.
Homeopathy was developed by Samuel Hahnemann and is founded on the principle of “similitude,” which is backed by inductive reasoning and states that a drug can treat a condition if it causes similar symptoms in healthy individuals. He attempted to treat several illnesses with potentized dilutions of the corresponding elicitors following the theory of “similia similibus curentur” (let likes be treated by likes). 12,13 Hahnemann prepared medications during his research using a wide range of natural ingredients. He discovered that these ultradilutions had some sort of potent activity when the infinite dilutions of these compounds were applied in phases, each followed by a forceful shaking “succussion”—a process called “potentization.” High potencies, such as 30c and 200c, have high dilution factors (1060 and 10400, respectively), which are many orders of magnitude larger than Avogadro’s number, meaning that there shouldn’t be any detectable amounts of the original ingredients left in the finished product. This method of treatment has endured the test of time and is still in use in many nations for the treatment of a variety of chronic conditions, including female disorders, despite numerous controversies and persistent challenges regarding its efficacy from the scientific community. 14 In the footnote of §94 of Organon of Medicine, he mentioned that in chronic diseases of females, it is required to pay attention to features such as pregnancy, sterility, sexual desire, accouchements, miscarriages, suckling, and menstrual discharge. 15 It is crucial to determine if it occurs at short intervals, how long it lasts, its flow, quantity, color, and presence of leucorrhea. It is essential to understand the nature, sensations, quantity, and conditions under which it occurs. 15
There are several homeopathic studies with various designs that address various causes of irregular menstruation, randomized trials of individualized homeopathic medicinal products (IHMPs), 16 –19 and two case series as well. 20,21 Different outcome measures were chosen in different studies, for example, visual analog scale, numerical rating scale (NRS), verbal multidimensional scoring system (VMSS), and premenstrual symptom (PMS) score; however, there has not been much research done on any particular validated measure that covers the range of menstrual abnormalities. One of the most common diagnoses made in the obstetrics and gynecology outpatient clinics of Indian homeopathic hospitals is still irregular menstruation. 22,23 This trial was the first attempt to explore the effects of IHMPs in centesimal potencies against placebo in treating menstrual irregularities.
Materials and Methods
Trial design
This double-blind, randomized (1:1), placebo-controlled, two-parallel arms trial was conducted in the obstetrics and gynecology, PG3, and research outpatient departments of D. N. De Homoeopathic Medical College and Hospital, West Bengal.
Ethics approval
The study protocol was approved by the Institutional Ethics Committee (reference number DHC/Eth-45/2018/754/2021; dated October 26, 2021). The trial registration number CTRI/2022/04/041659 was assigned to the protocol, which was prospectively registered in the Clinical Trials Registry, India. The protocol complied with the Good Clinical Practice guidelines and the Declaration of Helsinki. 24 Before enrollment, all patients received a patient information leaflet in the regional vernacular, Bengali, and all participants gave their signed informed consent.
Participants
The inclusion criteria were women aged between 11 and 25 years, presented with menstrual irregularities (the cycles are shorter or longer than normal; are heavier or lighter than normal; or are experienced with other problems, such as abdominal cramps) 25 with a history of suffering for 3 months or more, literate, and capable of reading both Bengali and English. The most common menstrual irregularities include amenorrhea, oligomenorrhea, menorrhagia, prolonged menstrual bleeding, and dysmenorrhea. Exclusion criteria were those denying consent to participate; the females who had carcinoma of the cervix, chronic tubo-ovarian mass, endometrial carcinoma, and genital tuberculosis; vulnerable population—unconscious, nonambulatory, too sick for consultation, differently abled, terminally or critically ill patients, and mentally incompetent people; the existence of mental or neurological conditions that impair life quality; blood hemoglobin level <7 g/dL; substance abuse and/or dependence; self-reported immunocompromised state; simultaneous participation in any other clinical trial; and the patients willing to avail and continue homeopathy and allopathy treatment concurrently or having received homeopathic treatment for any chronic illness during the previous 3 months.
Interventions
The subjects were randomized to receive either control (identical-looking placebos plus concurrent care) or verum (IHMPs plus concurrent care). IHMPs were prescribed in centesimal potencies (6cH, 30cH, 200cH, and 1000cH) and customized dosages following homeopathic principles. Six to eight medicated cane sugar globules (no. 20) made up each dosage. The participants were instructed to take them orally, with an empty stomach and a clean tongue. The frequency of administration was also individualized and was decided by the homeopathic doctors as appropriate to the cases. The follow-up visits were scheduled every month in person, for 4 months. Coded LM (50 millesimal) potencies could not be arranged for infrastructural constraints.
Comparable-looking placebos were administered to the control group like that of the verum group. Six to eight nonmedicated cane sugar globules (no. 20) soaked with rectified spirit made up the placebo.
Regardless of the codes they were given, all participants received generic nonmedical management advice, that is, to take iron-containing food, fiber-rich diet, and foods rich in phytoestrogens, as appropriate.
All the medicines were procured from a Good Manufacturing Practice-certified firm, Hahnemann Publishing Company Pvt. Ltd., Kolkata. Every unique prescription was supported by materia medica consultation, opinion of three homeopaths, and repertorization utilizing software (RADAR®, version 10.0.028 [ck], Archibel 2009, Belgium; and HOMPATH ZOMEO®, version 3.0), where needed. If required, subsequent visits involved adjusting the medications, potencies, and dosages following the traditional homeopathic principles. One of the homeopaths had been teaching classical homeopathy for more than 20 years and held a master’s degree in homeopathy. The remaining homeopaths were the organization’s postgraduate trainees. Each of the participating homeopaths was a member of their state council. Follow-up visits and weekly phone calls guaranteed adherence to suggestions. A medication accountability journal was kept, which tracked the dosages consumed and globules returned.
Outcomes
Primary outcome measures were the proportion of patients in whom menstrual irregularities (duration, quantity, or associated complaints; please see inclusion criteria mentioned above) in the early reproductive age group can be corrected for consecutive 3 cycles. The secondary outcome was the Menstrual Distress Questionnaire (MDQ) score.
26
It consisted of 47 symptoms on a six-point Likert scale (0–5) and constructed into eight clusters: Pain (items 5, 9, 16, 22, 25, 37)—muscle stiffness, headache, cramps, backache, fatigue, general aches, and pains; Concentration (items 2, 6, 7, 24, 29, 33, 35, 42)—insomnia, forgetfulness, confusion, lowered judgment, difficulty concentrating, distraction, accidents, and lowered motor coordination; Behavioral change (items 4, 8, 15, 20, 41)—lowered school or work performance, taking naps; staying in bed, staying at home, avoiding social activity, and decreased efficiency; Autonomic reactions (items 17, 23, 26, 28)—dizziness, cold sweat, nausea, vomiting, hot flushes; Water retention (items 1, 10, 30, 34)—weight gain, skin disorders, painful breasts, and swelling; Negative affect (items 3, 11, 21, 27, 36, 38, 40, 45)—crying, loneliness, anxiety, restlessness, irritability, mood swings, depression, and tension; Arousal (items 13, 14, 18, 31, 47)—affectionate, orderliness, faintness, feelings of well-being, bursts of energy, and activity; Control (items 12, 19, 32, 39, 43, 46)—the feeling of suffocation, excitement, ringing in the ears, heart pounding, numbness, tingling, blind spots, and fuzzy vision.
Timeline
For a maximum of 4 months, all the results were measured at monthly intervals.
Sample size
In the absence of any minimal clinically important difference (MCID) data of the primary outcome measure and any published paper claiming the effects of IHMPs in menstrual irregularities, pilot data for sample size calculation was not available. With an assumption of medium effect size (0.3) to detect statistically significant differences between proportions of females in whom normal menstrual cycle could be established using a chi-square test, a study with 88 (2 × 44) patients would provide 80% power, based on a two-sided significance level of 5%. The provision of a 5% attrition rate would further increase the target sample size to 92 (46 × 2).
Randomization
A list of 92 random numbers was generated using StatTrek centrally by an independent third party by restricting 9 permuted blocks of fixed size 10 plus another single block of 2 random numbers; that is, 90 + 2 = 92, preserving a 1:1 balance among groups. Participants were thus randomized evenly between the control and verum groups. This random number chart was given to the blinded pharmacist to distribute medication. Another impartial third party classified identical amber-colored glass vials as either “1” or “2,” denoting either identical placebos or medications. The random number chart determined which participant would get the vials in sequential order. After the dataset was frozen, the codes were broken after the trial.
Blinding
Throughout the study, everyone involved—participants, treating physicians, pharmacists, outcome assessors, and data entry operators—remained blinded. By asking the participants which group they thought they were in, the blinding was verified both before and after the study.
Allocation concealment
Participants were screened, enrolled, and assigned serial numbers by blinded postgraduate trainees and registration counter workers. The blinded homeopaths then conducted interviews with the blinded subjects to determine the prescription. As a result, allocation concealment was accomplished by keeping the random number sequence concealed from both the trial recruiters and the treating physicians.
Statistical methods
All enrolled participants were included in the final analyses, which were conducted using the intention-to-treat (ITT) approach. Predicted values from a linear regression model were used to impute the missing values. Shapiro-Wilk tests, Q-Q plots, and histograms were used to analyze the data distribution; no discernible deviation from normalcy was found. Baseline sociodemographic data was presented using descriptive statistics. The intragroup changes were presented in terms of descriptive statistics: mean and 95% confidence intervals (CI). Group differences were examined by Pearson’s chi-squared tests with categorical outcomes, two-way repeated measure analysis of variance accounting for the time-effect interactions, and unpaired t-tests comparing the mean estimates obtained individually every month. The effect sizes were presented in terms of partial eta-squared (small effect, 0.01–0.059; moderate effect, 0.06–0.137; and large effect, >0.138) and Cohen’s d (small effect, 0.2; medium effect, 0.5; large effect, 0.8). p-Values that were two-tailed and <0.05 were deemed statistically significant. The Statistical Package for the Social Sciences for Windows (version 23.0; IBM Corp., Armonk, NY, USA) was used to do all statistical computations.
Adverse events
The participants were advised to notify the outpatients immediately or over the phone about any injury, major adverse event, unanticipated effects, or uncomfortable aggravations (disease, medicinal, or homeopathic).
Trial reporting
Two guidelines were followed in reporting this trial—CONSORT and RedHot (Supplementary Data S1 and S2). 27,28
Results
Participant flow
In total, 92 of the 142 individuals who underwent screening were assigned to the verum (n = 46) or control (n = 46) groups upon enrolment in the trial. Some of the individuals stopped during the 4-month follow-up; these withdrawals were all caused by pregnancy, using alternative treatments, and living far away. Nevertheless, all 92 individuals finished the experiment and were included in the final analysis when they showed up for the last visit in the fourth month after receiving many phone reminders (Fig. 1).
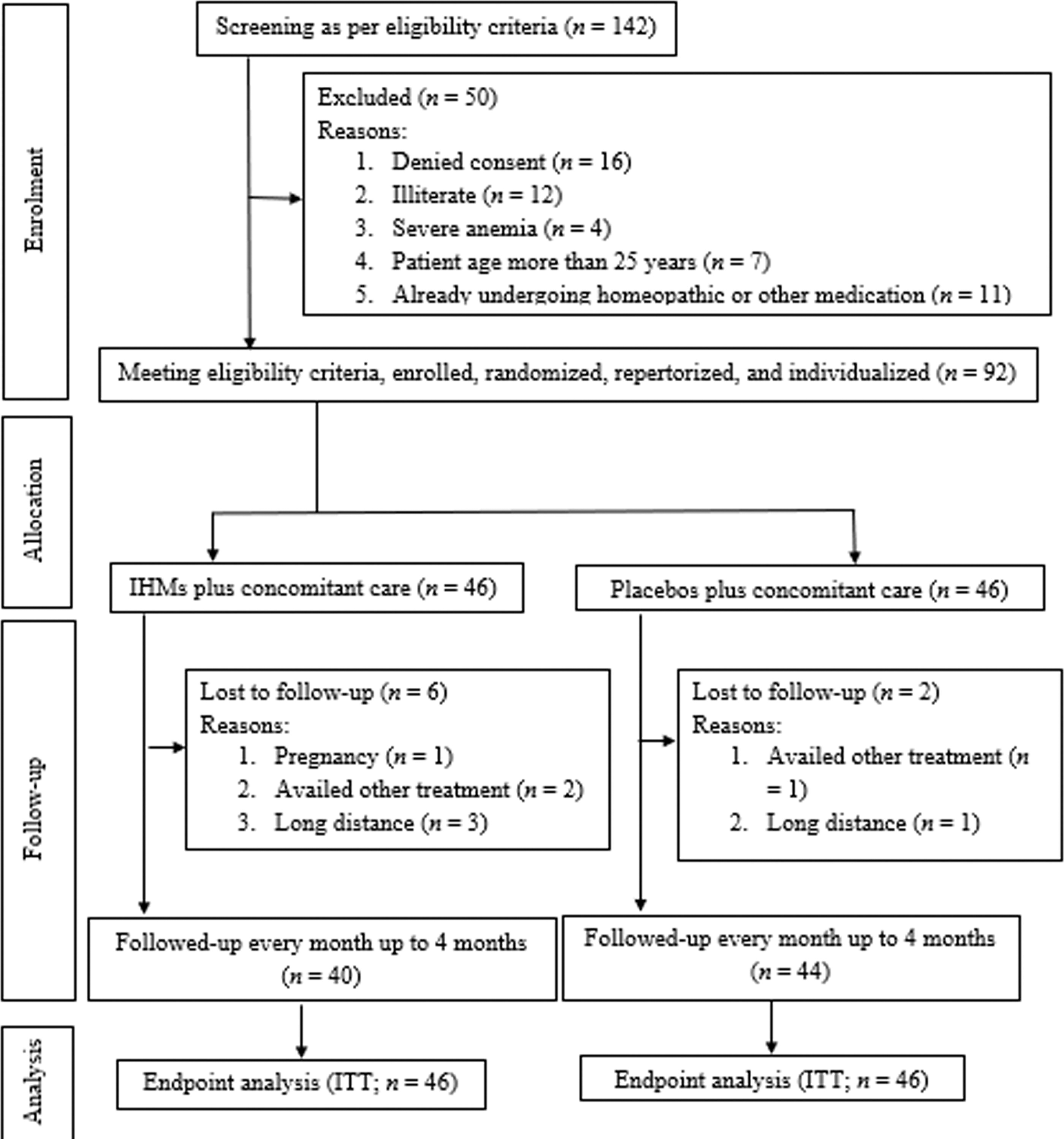
CONSORT study flow diagram.
Recruitment
A 4-month therapy phase followed a 15-month recruitment phase that ran from mid-April 2022 to July 2023 in this trial. By the end of July 2023, the final patient to be enrolled had received their follow-up.
Baseline data
Sociodemographic data and baseline outcome measures were presented using descriptive statistics (Tables 1 and 2).
Comparison of the Sociodemographic Characteristics Between Two Groups at Baseline (n = 92)
Continuous data presented as means ± standard deviations.
Continuous data presented as median (interquartile ranges).
Categorical data presented as absolute values (percentages).
IHMPs, individualized homeopathic medicinal products.
Numbers analyzed
Even though a small number of individuals dropped out during the first and second follow-up months, after 4 months, all recruited participants (n = 92) had completed their outcomes. The final analysis was conducted on 92 participants. Pregnancy, receiving other treatments, and distance were the reasons for discontinuation (Fig. 1).
Outcomes
The group difference in the main outcome was not significant—IHMPs: 22/46 vs. Placebo: 24/46, chi-square (Yates corrected) = 0.043, p = 0.835.
Group differences in MDQ total scores were not significant—two-way repeated measure analysis of variance (ANOVA), F 1, 90 = 0.054, p = 0.816, partial eta-squared = 0.001; unpaired t-test, mean difference −0.9, 95% CI: −1.2 to 3.0, p = 0.392, d = 0.179. All other MDQ subscales revealed similar nonsignificant trends of group differences, except the MDQ behavioral change subscale: two-way repeated measure ANOVA, F 1, 90 = 0.029, P = 0.865, partial eta-squared = 0.001; unpaired t-tests, mean difference −2.2, 95% CI: −2.9 to −1.4, p < 0.001, d = 1.242) (Table 2).
Comparison of the Secondary Outcome at Baseline and at Different Time Points (n = 92)
p < 0.05.
p < 0.001.
ANOVA, analysis of variance; CI, confidence interval; IHMPs, individualized homeopathic medicinal products; MDQ, menstrual distress questionnaire; p (a), intergroup differences detected by unpaired t-tests; p (b), intergroup differences detected by two-ways repeated measure ANOVA models; SD, standard deviation; SE, standard error; (a) Unpaired t-tests; t 90, t score at 90 degrees of freedom.
Medicines and repertories used
At baseline, 27 different medicines were prescribed—Pulsatilla nigricans (21.7%), Calcarea carbonica (18.5%), Natrum muriaticum (9.8%), Sulphur (7.6%), Sepia officinalis (6.5%), Phosphorus (4.3%), and Thuja occidentalis (3.3%) being the most frequently prescribed remedies (Table 3). Eight different repertories were used for selecting the remedies: Kent’s Repertory (35.9%), Complete Repertory (27.2%), Boger Boenninghausen’s Characteristics and Repertory and Boericke’s Repertory (9.8% each), Boenninghausen’s Therapeutic Pocket Book (7.6%), Minton’s Uterine Therapeutics (5.4%), and Synthesis Repertory and Murphy’s repertory (2.2% each). Methods used for repertorization were Kentian second method (64.1%), Boger’s and Boericke’s method (9.8% each), Hahnemann–Boenninghausen’s method (7.6%), Minton’s uterine method (5.4%), and Kentian third method (2.2%).
Prescribed Medicines in the Two Groups at Baseline (n = 92)
IHMPs, individualized homeopathic medicinal products.
Adverse events
Throughout the study, two adverse events were reported in the IHMPs group: one case of cough and cold and the other one suffered from a cut injury. The former was prescribed Belladonna 30cH, twice for 2 days. The latter was given a mother tincture of Calendula officinalis that healed her wound promptly. Two adverse events were reported in the placebo group—one case of coryza and another of diarrhea—and were treated with uncoded actual medicines. The former was prescribed Aconitum napellus, 30cH, twice for 2 days. The latter one was given Podophyllum peltatum 30cH twice for 2 days.
Discussion
In this randomized trial on 92 women with menstrual irregularities of the early reproductive age group, the proportion of patients in whom menstrual irregularities corrected for consecutive 3 cycles was nonsignificant statistically. The improvement observed in the MDQ total score and subscales scores was higher in the IHMPs group than in placebos, however statistically nonsignificant in most of the occasions, except for the behavioral change subscale; therefore, for menstrual abnormalities, it did not prove that the medication worked better than a placebo. This simply meant that during the trial, everyone got better, which is not unusual and is less likely to have been caused by the intervention because it happened in both groups. Only the MDQ behavioral subscale reflected the advantages of IHMPs over placebos. The subscale consisted of symptoms such as lowered school or work performance, taking naps, staying in bed, staying at home, avoiding social activity, and decreased efficiency; however, it is difficult to explain why this outcome might have been different than the others. Numerous additional factors, such as context and/or placebo effects, the administration of dietary recommendations mutually to all, and the covert use of any concomitant medicinal modalities, can also account for this. Pulsatilla nigricans, Calcarea carbonica, Natrum muriaticum, Sulphur, and Sepia officinalis were the most frequently prescribed medicines. Neither group reported any significant adverse events or injuries. Trials using diverse outcome measures are necessary to reach a definitive conclusion before making any recommendations.
The main advantages of the trial included allocation concealment, double-blinding, and randomization. The enrollment was prospective, meaning that the protocol was announced before the first patient was enrolled. Regarding the statement of protocol, either conduct or reporting, the study was transparent. All enrolled patients have been included in the final analysis, following the ITT method. The conventional principles of homeopathy were followed in the prescription of IHMPs, follow-up appointments, and dosage selection or adjustments. This was reinforced by the use of the consensus prescribing technique, which involved three homeopathic physicians for each visit.
Concerns about compromised external validity in randomized controlled trials (RCTs) persisted. One limitation on how the results could be interpreted was that the patients were carefully selected to participate in RCTs, and the patients seen in routine practice were not at all like the patients included in the trials—who have to fill out multiple self-administered questionnaires and receive extra attention and care during the consultation. Dietary guidelines that were jointly suggested to all recruited participants may have made it more challenging to employ robust two-way repeated measures ANOVA models to discover group differences, particularly overall group differences. For each patient, a four-month follow-up period may not be sufficient. In this study, all of the outcome measures were self-administered, subjective questionnaires. The experiment was significantly impacted by the withdrawal of follow-up visits by a considerable number of participants after the first, second, and third months owing to pregnancy, treatment availed, and long-distance travel. Because of the lack of the outcome measure’s MCID and pertinent published data from comparable trials, the estimated effect size and the sample size that followed were rather ambiguous.
Earlier, a pilot trial was conducted by Yakir et al. 19 between 1992 and 1994 in Israel on 23 women of age 20–48 years with PMS. The intervention was IHMPs, and the comparator was a placebo. The outcome measure of this study was scores of a daily MDQ, measured before and after treatment. With active treatment, mean MDQ scores decreased from 0.4 to 0.1 (p < 0.05), whereas with placebo, they decreased from 0.4 to 0.3; p = 0.057 (between groups). In total, 90% of patients getting active treatment and 37.5% receiving a placebo experienced improvement of greater than 30% (p = 0.048). The improvement observed in mean MDQ scores was much less (∼27%) in our trial than that of Yakir (∼70%). Yakir et al. prescribed five commonly used homeopathic medications that were described by specific clusters of guiding symptoms—Lachesis mutus, Natrum muriaticum, Sepia officinalis, Nux vomica, and Pulsatilla pratensis. All types of PMS symptoms improved, with water retention, functional complaints, and mental symptoms showing the largest effects. The least affected symptom was appetite. Compared with a placebo, homeopathic treatment was found to be more successful at reducing PMS symptoms. In another RCT by Yakir et al., 16 involving 105 women with premenstrual syndrome between the ages of 18 and 50, conducted in Israel between 1996 and 1999, the intervention was IHMPs and the comparator was placebo, and differences in changes in mean daily PMS scores by the MDQ served as the major end measures. The active medication group showed a significantly higher improvement in mean premenstrual ratings from 0.4 (± 0.3) to 0.3 (± 0.2) than the placebo group, from 0.4 (± 0.3) to 0.3 (± 0.4); p = 0.043. Improvement in mean MDQ scores was similar (27%) to that of Yakir et al. (35%). When compared with a placebo, homeopathic medications specifically recommended for each patient improved PM ratings more than placebo. There was an identical-looking placebo for each of the 14 homeopathic medications used in the study—Argentum nitricum, Arsenicum album, Calcarea carbonicum, Causticum, Lycopodium clavatum, Natrium muriaticum, Nux vomica, Phosphorus, Platina, Pulsatilla nigricans, Sepia officinalis, Sulphur, and Zincum metallicum. The improvement was greater in the active medication group than in the placebo group for all medications except one (Phosphorus). According to a study by Ghosh et al., 18 conducted in West Bengal in 2020, 128 women with primary dysmenorrhea between the ages of 13 and 45 participated in an RCT. The intervention was IHMPs, and the comparator was placebo. Primary and secondary outcome measures were 0–10 NRS measuring the intensity of pain of dysmenorrhea and VMSS, respectively. IHMPs outperformed placebos at all time points according to group differences in pain NRS and VMSS (all p < 0.001), with medium-to-high effect sizes. The two drugs that were most frequently prescribed were Natrum muriaticum and Pulsatilla nigricans (n = 20 each; 15.6%).
Subsequent investigations ought to focus on independent replications employing suitable result metrics, 50 millesimal potencies, and updated prescribing methodologies (such as cluster-symptoms methodology and polarity analysis). A continuous scale is more sensitive because all occurrences of disagreement are not treated equally, but a dichotomous scale, similar to that used in this trial whether the irregularities corrected or not, makes the presence or absence of agreement easier to understand and analyze. 29 The use of 50 millesimal potencies may help avoid unpleasant aggravations and thereby may help to avoid its untoward impact on the outcomes. 30 A novel method to improve the accuracy of homeopathic prescriptions is polarity analysis. 31 The cluster technique helps to enhance the precision and reproducibility of prescribing homeopathic medicines. 16 Menstrual abnormalities may be effectively treated with a range of homeopathic remedies, but these must be provided on a highly customized basis. In such instances, concurrent care measures or a mistaken remedy prescription may have obscured the benefits of homeopathy. An extra control group consisting solely of dietary advice could prove beneficial for future research.
Conclusions
In this RCT on 92 women of early reproductive age group with menstrual irregularities, the analysis failed to demonstrate clearly that IHMPs were effective beyond placebos in all but one of the outcomes. Future trials should consider different outcome measures.
Footnotes
Acknowledgments
The heads of the academic and hospital divisions of the institutions are acknowledged by the authors for enabling them to carry out the trial. The authors are also grateful to Dr. Susmita Lakra and other fellow postgraduate trainees—Dr. Indrani Halder, Dr. Sagarika Muduli, Dr. Nazia Anjum, and Dr Ankit Saha—hospital staff, pharmacists, and patients for their unwavering support and genuine involvement in the study.
Authors’ Contributions
U.N.: Clinical study and data acquisition; S.S.: Concept and literature search; R.K.P., S.M.A., T.P., R.G., P.D., and S.S.: Clinical study, data acquisition, and preparation of the article; M.K., U.R., and J.A.: Clinical study and data acquisition; M.K. and S.S.: Design, data interpretation, statistical analysis, and preparation of the article. All the authors reviewed and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Statement
The project received no external funding. The institution has no role to play in the analysis of the study results and publication of the paper.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.