
Abstract
Approximately 170 million people are infected with the hepatitis C virus (HCV) worldwide. Infection with this pathogen is persistent in more than 80% of cases, frequently developing severe forms of liver damage such as cirrhosis and hepatocellular carcinoma. No preventive vaccine is available against HCV, and current treatment based on the combination of pegylated interferon and ribavirin is effective in ∼55% of patients infected with genotype 1, the most prevalent genotype. This review analyzes several factors influencing the achievement of a sustained virological response, namely undetectable HCV RNA at 6 months after conclusion of therapy. Particularly, the relevant issue of age and duration of infection is discussed in detail. Indeed, the final decision for starting treatment should be a case-by-case point. However, the cost–benefit analysis seems to indicate that in patients who are motivated and without contraindications, starting the treatment as early as possible is probably the best choice for success.
Introduction
H
Exposure to HCV-contaminated blood and blood-derived products is the main source of HCV infection. Individuals receiving transfusions, clotting factor concentrates, organ transplant, and hemodialysis have a risk for infection with HCV, especially before the implementation of current blood control screening policies. Moreover, illicit drug use, having multiple sexual partners, sharing razors or toothbrushes, folk medicine practices, including acupuncture and ritual scarification, as well as body piercing, tattooing, and commercial barbering when performed without appropriate infection control measures are potential modes for transmission of HCV infection (Alter and others 2004).
Patients suffering from acute symptomatic hepatitis C are rare and usually >50% of them clear the infection spontaneously (Gerlach and others 2003). Contrariwise, once the chronic infection is established, there is no possibility of viral clearance, unless a therapeutic intervention is performed. Symptoms associated with chronic hepatitis C disease usually appear only several years after infection with HCV (Thomas and Seeff 2005). In the meantime, unrecognized HCV patients can transmit the virus to uninfected people. Because of the lack of early symptoms, sometimes detection of infection occurs too late for achieving sustained viral clearance with current therapy, based on the combination of pegIFN plus ribavirin. These facts imply that the therapeutic window is short timed for a complete clearance to be achieved in a substantial percentage of patients. Patients who do not respond to therapy continue to be chronically infected, requiring a liver transplant in the future, if severe liver damage appears. Unfortunately reinfection after transplantation is universal (Gallegos-Orozco and others 2009). Given that an active screening for HCV-infected individuals in the general population around the world, although desirable, is not feasible nowadays, even for developed countries, having a more rational diagnosis policy that also considers what to do after a patient is detected is the most important point.
Early detection of HCV-infected individuals is vital for medical decision related to treatment and for stopping the spread of HCV. Several antibody-based (Colin and others 2001) and RNA-based methods for detection of HCV infection have been developed and are currently available (Scott and Gretch 2007). Anti-HCV antibodies are generally detectable after 3–6 months of HCV infection, and systems used for their detection are the usual first-line screening. Despite HCV RNA can be detected earlier than antibodies (generally after 10 days of HCV infection), its detection systems are generally used for confirmation of infection because of higher cost (Scott and Gretch 2007).
Successful treatment against HCV infection seems to be dependent on several factors (Aronsohn and Reau 2009; Maekawa and Enomoto 2009; Reddy and others 2009). In this review, some of these factors will be discussed. Particularly, the importance of starting therapy early after detection of HCV infection will be focused.
Therapy Against HCV
Nowadays, the best therapy is the weekly administration of pegIFN (1.5 μg/kg for pegIFN-α-2a or 180 μg for pegIFN-α-2b) and daily ingestion of ribavirin (1,000 mg for body weight <75 kg and 1,200 mg for body weight >75 kg), for 6 months (for HCV genotype 2 or 3) or 1 year (for HCV genotype 1 or 4). Prolonging therapy for additional 24 weeks can be considered in patients who are slow to respond (clearance of HCV RNA between weeks 12 and 24) (Berg and others 2006; Yuki and others 2009). The main goal of the therapy is to prevent complications and death from HCV infection, through the control of viremia. HCV infection is persistent in >80% of cases exposed to this pathogen. Nevertheless, >50% of acute symptomatic patients spontaneously and permanently clear HCV infection within the first 3–4 months after the onset of symptoms (Gerlach and others 2003). Individuals spontaneously clearing HCV infection are able to eliminate the virus in the first 6 months after virus exposition. Thus, chronic state is virologically defined as at least 6 months persistence of HCV RNA after viral exposure.
According to accumulated data, IFN-based treatment in the acute phase reduces the risk to evolve to chronic HCV infection and is consistently better than observation, as a strategy to follow with asymptomatic patients, who have little chance of spontaneous viral clearance and should, therefore, receive immediate antiviral treatment (Gerlach and others 2003; McGovern and others 2009; reviewed by Vogel and others 2009). In addition, it has been shown that IFN-based antiviral treatment of those acute symptomatic patients with persistent viremia, beyond 3 months after the onset of symptoms, results in a sustained viral elimination in 80% of treated patients (Gerlach and others 2003).
Further, studies conducted in individuals recently infected because of injecting drug use showed that treatment with pegIFN alone remains effective for HCV-monoinfected patients, when commenced at up to 12 months post-HCV infection (Dore and others 2009; reviewed by Vogel and others 2009). These data show the opportunity to offer less aggressive and toxic treatment variants for those individuals being diagnosed shortly after infection. Nevertheless, it is obvious that pegIFN monotherapy may be suboptimal depending on different factors that must be addressed, such as the infecting genotype and the viral load.
It is reasonable to treat nonsymptomatic, or symptomatic with HCV RNA detectable after 3 months, acutely infected individuals, for at least 12 weeks with IFN-based alternatives (Gerlach and others 2003) (Fig. 1). The optimal treatment regimen, including the use or not of ribavirin, and when it should be initiated, remains uncertain.
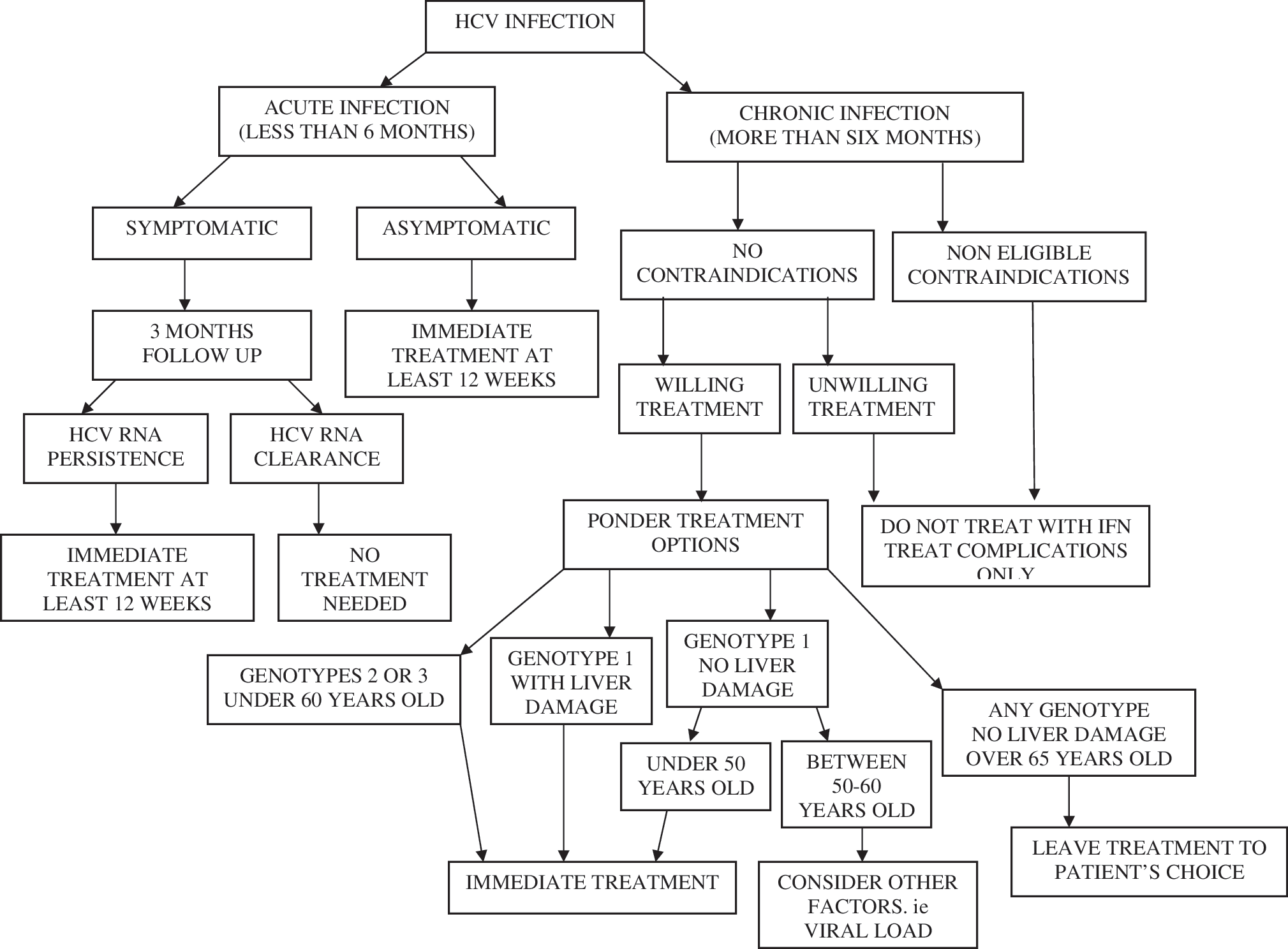
Treatment algorithm for managing and treating patients with HCV infection. HCV, hepatitis C virus.
It is widely accepted that HCV-chronic individuals aged 18 years or older, with HCV RNA detectable in serum, liver biopsy showing chronic hepatitis, but having compensated liver disease (total serum bilirrubin <1.5 g/dL, international normalized ratio 1.5, serum albumin >3.4, platelet count 75,000 mm, and no evidence of hepatic encephalopathy or ascites), and acceptable hematological and biochemical indexes (hemoglobin 13 g/dL for men and 12 g/dL for women; neutrophil count 1,500/mm3 and serum creatinine <1.5 mg/dL), and willing to be treated and to adhere to treatment requirements, with no contraindications, should be treated.
Contrariwise, individuals with major uncontrolled depressive illness, solid organ transplant (renal, heart, or lung), autoimmune hepatitis, or other autoimmune conditions known to be exacerbated by pegIFN and ribavirin, untreated thyroid disease, pregnant or unwilling to comply with adequate contraception, severe concurrent medical disease (severe hypertension, heart failure, significant coronary heart disease, poorly controlled diabetes, and chronic obstructive pulmonary disease), age <2 years, and known hypersensitivity to drugs used to treat HCV should not be treated (Ghany and others 2009) (Fig. 1).
Successful therapy is considered as sustained virological response (SVR), established as undetectable HCV RNA at 6 months after the end of current standard treatment. Patients who achieve an SVR usually have improvement in liver histology and clinical outcomes. Two major predictors of an SVR have been found: the viral genotype and pretreatment viral load (Ferenci and others 2005; Francois and others 2009). SVR rates have been higher in patients infected with HCV non-1 genotypes (mostly genotype 2 and 3) and in those with a viral load of <600,000 IU/mL (Ghany and others 2009). In addition, several other baseline characteristics of patients have been associated with a favorable response, although less consistently. Female sex, age <40 years, non–African-American race, body mass index (<25), absence of insulin resistance, nonalcohol consumption, lack of coinfections with HIV or other comorbidities (thalasaemia, hemophilia, or organ transplant), absence of steatosis, and bridging fibrosis or cirrhosis on liver biopsy are other positive indicators for SVR (Pol and others 1999; Manns and others 2001; Fried and others 2002; Peters and Terrault 2002; Poynard and others 2003).
Even when the main goal of IFN plus ribavirin-based therapy is sustained viral clarification, as surrogate of the clinical endpoint, several studies indicate that chronic patients not achieving an SVR but being at least sustained biochemical responders may benefit from the therapy by improving their degree of irregular regeneration of hepatocytes and the F stage, thereby reducing the risk for HCC (Moriyama and others 2007). Indeed, mathematical modeling suggests that treatment of half or all of infected persons would result in decrease of complications of liver disease, such as liver failure by 39.4% or 78.9%, HCC by 30.2% or 60.4%, and liver-related deaths by 34.0% or 68.0% over the next decade (Davis and others 2010) (Fig. 2). Remarkably, sometimes SVR is not enough because liver cancer has been identified years later, especially if cirrhosis existed at the time of achieving an SVR (Kobayashi and others 2007).
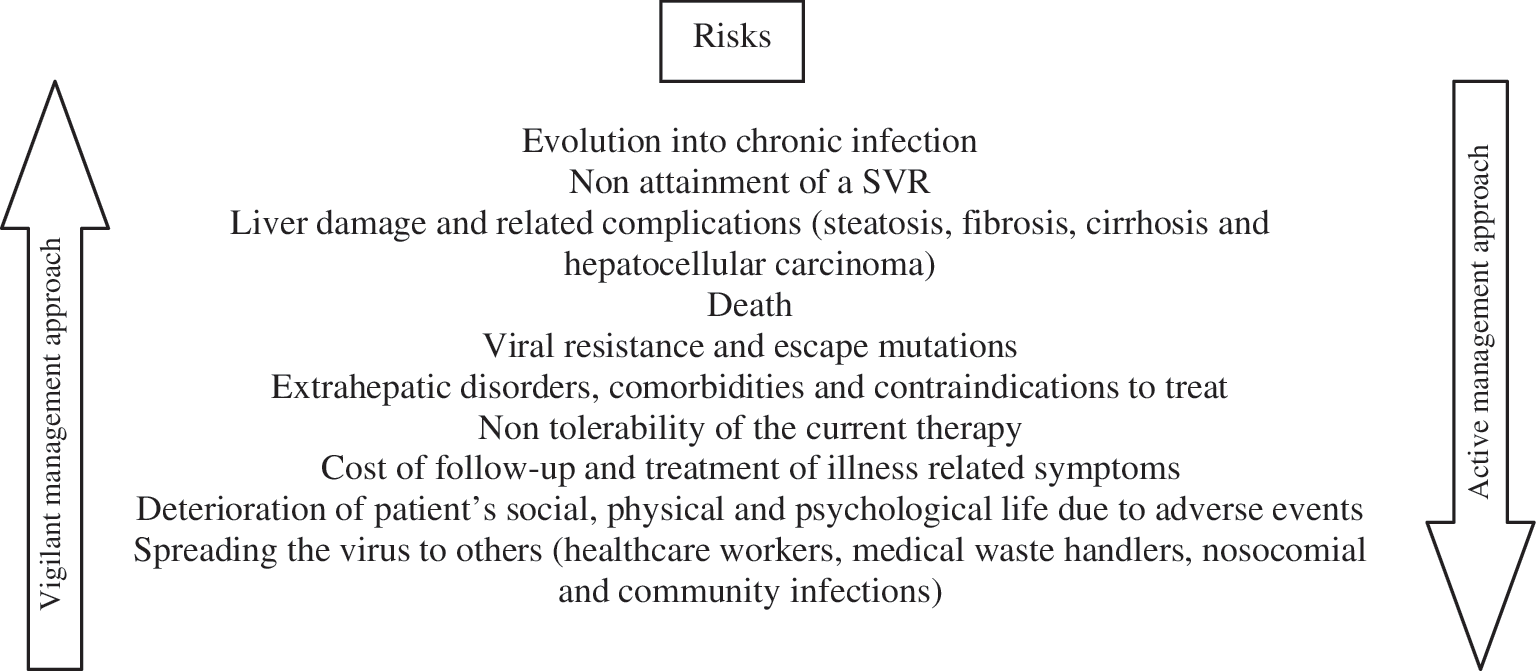
Factors to be analyzed for decision of active or vigilant management approach. SVR, sustained virological response.
In Kaplan–Meier survival analysis, HCV infection was associated with a shortened survival, and this effect persisted after adjusting for several of the common comorbidities, specifically increasing risk of death by ∼37%. Among subjects with HCV infection, those who did not receive treatment also had a shortened survival compared with those who received 48 weeks or more of treatment for HCV. Treatment decreased the risk of death in a “dose-dependent” manner, with increasing duration of treatment being associated with decreasing mortality (Butt and others 2009a) (Fig. 2).
IFN-based treatments, and particularly the current therapy, do not accelerate or increase the risk for the development of liver damage, independently of the result concerning HCV RNA clearance or persistence. On the contrary, even in the case of persistent HCV infection after unsuccessful treatment, data have accumulated about the antifibrotic effect of IFN-based treatment in chronic patients. IFN-α inhibits collagen secretion and increases the capacity of the liver to degrade type I and type III collagen. The antifibrotic effect of IFN-α seems to be mediated by cytokines (Inagaki and others 2003; Giannelli and others 2006). On the basis of these elements, maintenance therapy with pegIFN with the goal of delaying or preventing progression to cirrhosis and/or hepatic decompensation is currently being assessed. Any benefit in this regard, even if only transient, is supposed to have a positive impact in the health-related quality of life for patients. In fact, although some discrepancies may be observed regarding the preventive effect of IFN-based therapy on HCC development, the pooled estimate is significantly in favor of IFN treatment, even in nonresponder and cirrhotic patients (Miyake and others 2009). Multiple courses of IFN treatment as well as prolonged IFN treatment are speculated to be more advantageous to prevention of HCC development (Miyake and others 2009).
Certainly, the current therapy against HCV infection is expensive, time consuming (6 months or 1 year, according to the virus genotype), and ineffective in approximately half of cases and takes toll on patient's social, psychological, and physical life (Ghany and others 2009). These factors undoubtedly contribute to the fact that only a minority of HCV-infected individuals receive antiviral treatment, with values as low as 10% in some particular groups as HIV-coinfected patients (Wagner and others 2009). Approximately 75% of patients treated with pegIFN plus ribavirin experience one or more side effects, requiring concomitant medication in some cases, otherwise compliance and tolerance to medication may be adversely affected (reviewed by Zickmund and others 2006).
It is expected that new alternative treatments become available in the near future as a solution for patients who fail to therapy with pegIFN plus ribavirin. In fact, recent results of clinical trials with protease inhibitors, particularly Boceprevir (Berman and Kwo 2009) and Telaprevir (Hoofnagle 2009), have indicated promising actions against HCV infection. Additionally, several therapeutic vaccine candidates are currently being evaluated in clinics with relevant immunogenicity and accurate safety profiles (Alvarez-Lajonchere and others 2009; Habersetzer and others 2009; Wedemeyer and others 2009). For the moment, retreatment with the same regimen leads to an SVR in fewer than 5% of patients and, therefore, requires an individualized analysis.
Immune System in HCV-Infected Patients: Impact on Treatment Results
Different evidences show that HCV can replicate in, or at least enter into, the cells of the immune system, in addition to hepatocytes (Castillo and others 2005; Pham and others 2005). In fact, several mechanisms of the immune system, both the innate and adaptive responses, related with the potential clearance of HCV infection are affected in the chronic phase: increased resistance to IFN, defects in the function of antigen-presenting and natural killer cells, and specific T-cell impairment and exhaustion, among others (Grakoui and others 2003; Bode and others 2007). These defects may result in uncontrolled viral replication and high viral load, which could be linked to the nonattainment of an SVR (Fig. 2). Therefore, some authors recommend starting therapy early in infection, at the time of lower viremia (McGovern and others 2009).
On the other hand, inaccurate immune response is involved in complications associated with HCV infection. In fact, autoimmune hepatitis is frequently detected in HCV patients, particularly in those coinfected with HIV (Ramos-Casals and others 2003). Additionally, HCV infection is associated with numerous hematologic, renal, dermatologic, rheumatic, and autoimmune disorders (El Serag and others 2002; Zignego and others 2007; Craxi and others 2008; Antonelli and others 2009; Perico and others 2009). Mixed cryoglobulinaemia and its vasculitic manifestations are one of the more frequent HCV associated-extrahepatic manifestations (Poanta and Albu 2007; Sansonno and others 2009). The chronic fatigue syndrome, the sicca syndrome, the non–insulin-dependent diabetes mellitus, malignant B-cell proliferations, mainly the HCV-related splenic lymphoma with villous lymphocytes and the production of autoantibodies, and thyroid cancer are other extrahepatic manifestations of interest (Poanta and Albu 2007; Zignego and others 2007). At least 10%–15% of HCV-infected individuals show extrahepatic complications (Sansonno and others 2009), and their detection is supposed to increase with age and years of HCV infection. Mechanistic immunological explanations for all these extrahepatic manifestations are not generally completely defined. In the case of mixed cryoglobulinemia and vasculitic manifestations, their management may be critically changed because of the increasing use of anti-CD20 therapy (Roccatello and others 2008; Saadoun and others 2008). Besides, nonsteroidal anti-inflammatory drugs, low-dose corticosteroids, hydroxychloroquine, methotrexate, penicillamine, combined antiviral therapy, cyclosporin A, and anti–tumor necrosis factor-α agents, among others, are currently being evaluated as treatment options for HCV-associated extrahepatic manifestations (Buskila 2009). Controlled studies are needed to further establish the treatment indications, efficacy, and safety of these agents.
It should be noted that both the pharmaceutical components involved in the current anti-HCV treatment are able to influence the immune system. In addition to the direct antiviral effect, IFN-α has a broad spectrum of immunomodulatory activities on both the innate and adaptive immune responses. These include upregulation of major histocompatibility complex class-I and class-II, increased natural killer cell activity, enhancement of dendritic and T cells activation, and increased lymphocyte trafficking and effector functions (Ji and others 2003; Tamir and others 2005). On the other hand, ribavirin promotes T helper 1 (Th1) reactivity, while inhibiting Th2 cytokine production (Tam and others 1999; Shiina and others 2004). The exact role of the immunomodulatory actions of IFN and ribavirin on the final result of treatment is not completely clear. However, it has been previously demonstrated that early therapeutic intervention with IFN-based treatment can reconstitute the pool of long-lived polyfunctional memory T cells (CD127- and Bcl-2-positive cells), which has been associated with the clearance of HCV infection (Badr and others 2008). In contrast, the inability to rescue such a polyfunctional response when treatment is initiated late in the chronic infection may increase the possibility of virus recurrence and relapse upon discontinuation of therapy (Badr and others 2008).
Cytopenias have been observed in treatment-naive HCV infections (Ramos-Casals and others 2003). Elderly patients are at greater risk of cytopenia during antiviral therapy for hepatitis C (Nudo and others 2006). In addition, hematological adverse events related to pegIFN and ribavirin therapy include leukopenia, particularly neutropenia. The decrease in the number of white blood cells places the individuals at increased risk of infection with other pathogens. The use of growth factors to treat cytopenias has been evaluated, mainly administering granulocyte colony-stimulating factor (Koskinas and others 2009; Laguno and others 2009). This strategy can obviate dose reductions and potentially improve the patients' health-related quality of life.
In our opinion, satisfactory modulation of the immune system to clear HCV infection or to avoid/stop undesirable complications seems to be more successful in younger state and shorter duration of infection.
Time: A Relevant Issue
Natural history of HCV infection is marked by the slow evolution of hepatitis C disease. First evidences of chronic liver damage usually appear after 10 years of infection and the following 2 decades are required for development of liver cirrhosis and potential liver failure (Moriyama and Arakawa 2006). The annual rate of progression of F stage has been estimated as 0.10–0.13 per year (Moriyama and Arakawa 2006). Host factors that are associated with an accelerated rate of progression include male sex, infection after the age of 40 years, and alcohol excess. Additionally, older age, longer duration of HCV infection, obesity, and history of diabetes mellitus are independent clinical parameters associated with advanced fibrosis (Hu and others 2009). Once liver cirrhosis is established, 7% of patients develop HCC each year (Moriyama and Arakawa 2006).
A particular group of HCV-infected individuals (10%–30%) has an even slower progression of hepatitis C disease, showing a normal liver for 2–3 decades. However, the “healthy carrier state” is not fully defined and seems to be transient because eventually liver abnormality appears even in the presence of normal values of transaminases (Puoti 2004). A reliable study was conducted by the Trent Hepatitis C Study Group to evaluate the risk of alanine aminotransferase (ALT) flare and fibrosis progression in a large geographically determined population of patients with HCV infection (Lawson 2010). There was no statistically significant difference in the rate of fibrosis progression between the persistently normal alanine aminotransferase (PNALT) patients and those with an elevated ALT and it was also shown that within 5 years of the initial definition period for PNALT, over 60% of patients with PNALT had a recorded ALT over the normal limit (Lawson 2010). Patients with a PNALT seem, therefore, to be as much at risk of disease progression as those with an elevated ALT and warrant the same consideration with respect to treatment (Lawson 2010). Patients with normal liver tests can be treated with the same response rates as patients with elevated transaminases (Bini and Mehandru 2006). Remarkably, slow fibrosis progressors have better SVR than fast progressors (Myers and others 2003).
It is well known that HCV develops several strategies for persistence in the host, including increased heterogeneity of quasispecies, emergence of very efficient escape mutants, and direct action over immune system (Grakoui and others 2003). After decades of infection, some consequences of these viral events on the host might not be reversible.
Nowadays, life expectancy in several countries is over 70 years or more. Therefore, most individuals becoming chronically infected before 50 years of age are at high risk for suffering important liver damage associated with HCV infection, if no successful treatment is carried out. In this scenario, morbidity and mortality associated with HCV infection might become an important negative factor for extending life expectancy and could seriously affect health-related quality of life in the third age. In addition to the aforementioned elements, previous studies have found that HCV infection is associated with higher risk of coronary artery disease (Butt and others 2009b) and lower response rates to vaccination (Kramer and others 2009). People infected with HCV, even having none or only minimal symptoms and liver damage, can transmit the virus and constitute a potential source for spreading of this pathogen, even if preventive measures are taken.
Despite dissatisfactions related to therapy, recommendation for starting treatment early after detecting established chronic infection is probably the best choice. Older age is a worst prognostic factor for tolerability of current therapy and achievement of SVR (Horsmans 2010; Huang and others 2010). Moreover, adherence to therapy is a critical factor for successful treatment; in general, the physical state of individuals deteriorates with time, immune system turns weaker, physiologic and metabolic disorders accumulate, and an important number of comorbidities appear (Fig. 2). Older patients suffer more frequently from anemia, depression, insomnia, heart disease, hypertension, diabetes mellitus, insulin resistance, steatosis, lung disease, and other disorders, which cause worst results after therapy or even contraindication to treat (Aronow 2009; Denys and others 2009; Fetveit 2009; Small 2009; Van Puyvelde and others 2009; Ramani 2010). Particularly, patients with insulin resistance show a slower early viral kinetics (virus-RNA decay observed at 24 h after the first injection of pegIFN), which results in a significant difference in the percentage of patients achieving rapid (week 4) SVR (Bortoletto and others 2009).
In other aspects, the cost for continuous follow-up of HCV infection increases with years of infection, in direct laboratory testing and medical evaluation, as well as in absence to work or reduced efficiency due to illness-related symptoms, including psychological stress, or visits for medical assistance and evaluation (John-Baptiste and others 2009). Also, consumption of medicaments to treat illness-related symptoms, as well as the cost involved, increases with years of infection with HCV. In addition, HCV patients with liver damage are limited to receive medications, if they are hepatotoxic, to treat non-HCV diseases or symptoms, with the obvious inconveniences. In general, the longer the HCV infection and greater the liver damage, the worst will be the health-related quality of life for patients (Fig. 2).
Another pivotal aspect related to continuous follow-up of HCV patients is that this infection represents an important occupational hazard for healthcare workers, even in the developed world. Reports of transmission rates after needle-stick injuries vary from 0.2% to 1.8% (reviewed by Ozaras and Tahan 2009). Also, medical waste handlers are at risk of exposure to HCV infection, with prevalence estimates of up to 2.7% (Franka and others 2009). On the other hand, this virus can be nosocomially transmitted (Thompson and others 2009), constituting a serious risk, principally in developing countries with an endemic background, in which safe clinical and infection control practices are deficient or lacking (Fig. 2).
Concluding Remarks
Many factors influence the decision to treat an individual infected with HCV. According to the most recent guidelines and recommendations for the management of hepatitis C, young patients who are infected with HCV genotype 2 or 3, highly motivated, and without contraindication may be treated, even without histological assessment. In contrast, a strategy of nonintervention might be preferred in HCV patients with none or minimal liver damage and who are above the age of 60–65 years, have major contraindication to antiviral therapy, or are reluctant to be treated. In other cases, a personalized analysis is required. As IFN-based treatments do not accelerate or increase the risk for the development of liver damage, but conversely seems to delay it or reduce it and increase health-related quality of life, at least transiently, it is probably better to treat as soon as possible those individuals who are under 45–50 years of age, motivated, and without contraindications, even if liver damage is undetectable. Delays in starting therapy might sometimes mean decreasing opportunities of attainment of an SVR or even becoming ineligible for treatment. Clearance of HCV infection in early chronic phase is expected to diminish the chances for transmission of virus to new individuals, contributing to the control of HCV spreading, and more important, it will have a positive global health impact by reducing the appearance of severe forms of liver disease and thus related morbidity and mortality. Anyway, whether an active or vigilant (delay therapy in hopes of individualized nonsevere liver damage progression or better future treatment options) management approach is used, advance of effective programs for promoting patient treatment willingness is critical to ensure greater therapy uptake. This should have a direct effect by increasing life expectancy in several countries.
Footnotes
Author Disclosure Statement
No competing financial interests exist.