
Abstract
In the present scenario, doctors have to rely on radiological methods for diagnosis of acute abdomen in addition to their clinical skill. The use of serum markers for assessing the outcome of such patients is still debatable. Our aim was to evaluate whether the combined use of serum lactate, interleukin (IL)-6, and C-reactive protein (CRP) is able to simultaneously establish both the septic status and the prognosis of acute abdomen. Ninety-nine patients undergoing surgery for acute abdomen were taken up for the study. The patients were divided into 4 groups based on the level of sepsis. Serum lactate, IL-6, and CRP were determined in the serum of all the subjects. It was found that serum lactate determination, using the cutoff value < 3.9 mM, had a high sensitivity (100%) and specificity (83%) in differentiating patients with severe sepsis from those with sepsis. IL-6 came next with a sensitivity of 87% and a specificity of 81%. The AUC for serum lactate (0.922), IL-6 (0.912), and CRP (0.719) in differentiating between patients with severe sepsis and those with sepsis also proves the superiority of serum lactate and IL-6. The combined use of serum lactate and IL-6 would allow us to simultaneously establish the prognosis of patients with acute abdomen (r 2=0.368, P=0.008). The combined use of serum lactate and IL-6 is useful in simultaneously establishing both the severity of sepsis and, hence, the prognosis of acute abdomen.
Introduction
C
Patients and Methods
One hundred thirty-six consecutive cases of acute abdomen brought to the emergency department of our hospital were selected for the study. Patients who had not given informed consent, those with psychoses, and those with a history of malignancies, chronic renal and hepatic insufficiency, and chronic pancreatitis were excluded from the study, thus restricting the list to 99 cases. Ninety-nine healthy subjects, randomly selected in the same time period from blood donors and subjects who underwent medical check-ups, were also studied; there were 55 men and 44 women (mean age, 54 years; range, 18–82 years). They had been screened by means of an interview, physical examination, and routine blood analysis and showed no evidence of illness. No significant differences in gender and age were found among the 3 groups of subjects studied. For the 99 cases, relevant blood and radiological investigations were taken to arrive at a diagnosis.
After obtaining informed consent, blood samples for analysis of IL-6, Serum lactate, and CRP were taken at the time of admission. Serum for IL-6 collected using standard sampling tubes was transported to the laboratory within 5 h at 20°C–25°C. The samples for IL-6 were analyzed using Elecsys 2010 cobas e 411 analyser by Electrochemiluminescence immunoassay. The measuring range of IL-6 is 1.5–5,000 pg/mL (defined by the lower detection limit and the maximum of the master curve). The normal value for IL-6 in a healthy individual is expected to be <7 pg/mL. The samples of Serum lactate collected from a stasis-free vein were analyzed using RANDOX analyzer using the colorimetric method. The normal value of serum lactate is 0.5–2.22 mM. The test is linear up to a Lactate concentration of 12.21 mM. The samples for CRP were measured immunoturbimetrically using RANDOX analyzer. Serum is used undiluted, and CRP remains stable in the serum for at least 3 days at 15°C–25°C. The measuring range of CRP is 0–220 mg/L, the normal value of CRP being <5 mg/L. Relevant blood and radiological investigations were taken to arrive at a diagnosis. According to ACCP guidelines, the patients were divided into the 4 grades of sepsis, namely systemic inflamatory response syndrome (SIRS), sepsis, severe sepsis, and septic shock (Bone and others 1992). The classification was performed without knowledge of the results of the tests under investigation. The complications arising after surgery were also documented.
The patients were then operated on and were followed up for a period of 1 month. The presence or absence of complications developing (medical complications such as renal failure, acute respiratory distress syndrome (ARDS) etc., or surgical complications such as anastomotic leaks, fistulas, abscesses etc.) was documented during the period.
Descriptive statistical analysis
Receiver operating characteristic (ROC) curves and the respective areas under the curves were calculated for each marker to provide information about the accuracy of IL-6, serum lactate, and CRP in predicting the prognosis of the patients. Nonparametric estimates of the areas under the ROC curves and the respective standard errors were applied (Hanley and McNeil 1982). A procedure involving paired data was applied to compare areas under the ROC curves (Hanley and McNeil 1983). The best cutoff was chosen as the value that maximized the likelihood ratio (LR) obtained using the following formula: LR=(probability of true positive+probability of true negative)/(probability of false positive+probability of false negative). The best cutoff values are reported as ranges in which the diagnostic performance of the method does not change. Using these cutoff values, we calculated the sensitivity, specificity, and percentage of correct results in simultaneously establishing the severity of sepsis and prognosis of acute abdomen for serum lactate, IL-6, and CRP. The Yates-corrected x2 and the Mann–Whitney U-test were applied to compare different groups of subjects. All statistical evaluations were performed running the SPSS/PC1 statistical package on a personal computer. A 2-tailed P<0.05 was used to define statistical significance.
Results
Patient characteristics
Of the 99 patients, 67 patients were men (67.67%) and 32 were women (32.32%). Thirteen cases underwent appendicectomy (13.13%), 49 patients underwent perforation closure (49.49%), and 37 patients underwent intestinal obstruction (37.37%). Two patients were admitted with SIRS (2.2%), 25 patients with sepsis (25.25%), 61 patients with severe sepsis (61.61%), and 11 patients with septic shock (11.11%). After surgery, 64 patients (64.64%) were discharged without complications, whereas 19 patients (19.19%) developed complications, and 15 patients (15.15%) died, as shown in Table 1.
Total number of patients is 99.
SIRS, systemic inflammatory response syndrome.
Mean levels of serum markers
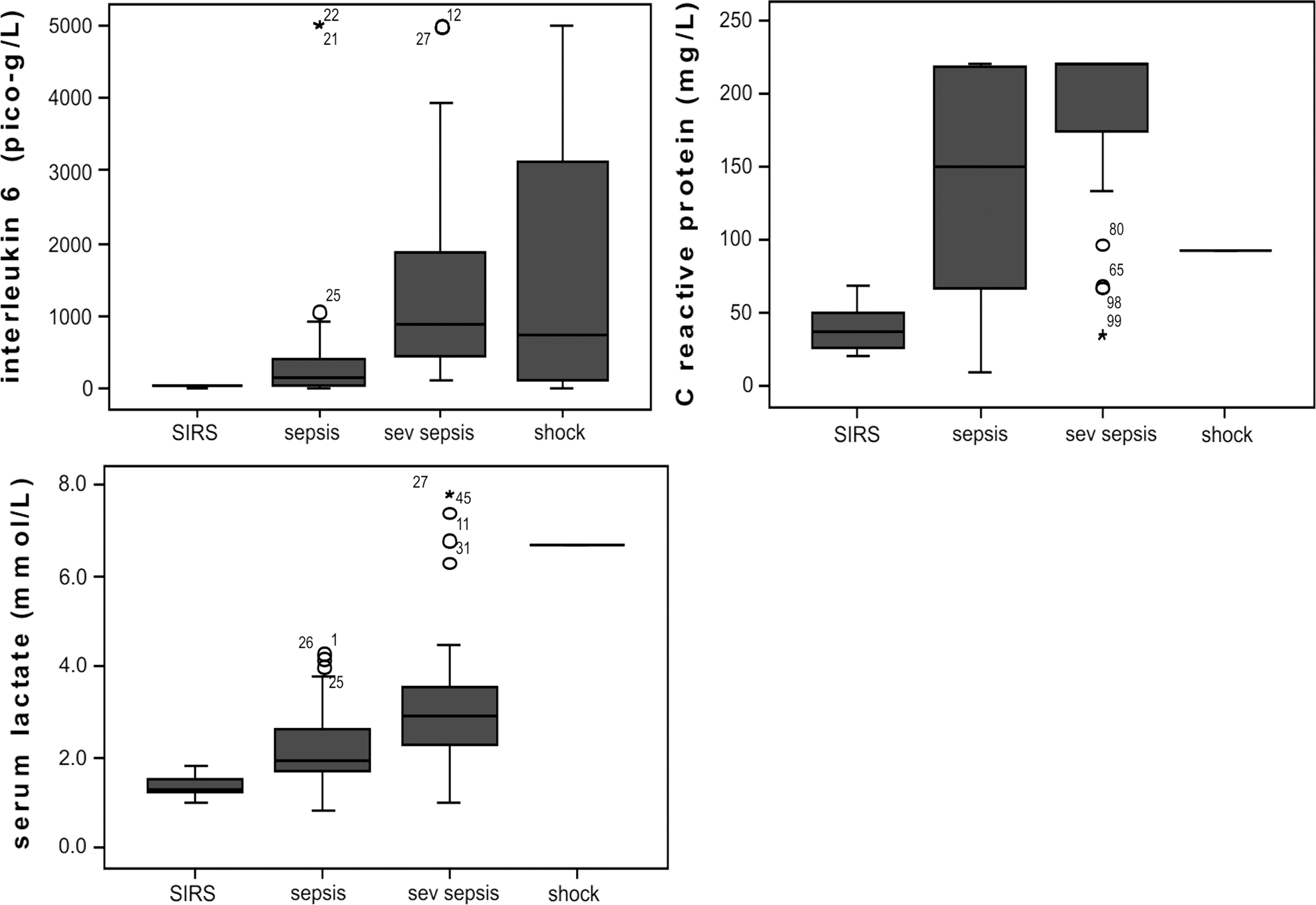
In 99 healthy volunteers, the levels of IL-6, serum lactate, and CRP remained within reference range, as shown in Table 2. These levels were shown to increase as the grade of sepsis increased and are depicted in the box and whisker plot Fig. 1.
Level of serum markers for the different grades of sepsis.
CRP, C-reactive protein; IL, interleukin.
IL-6 and sepsis
As shown in Table 3, patients with septic shock had significantly higher serum concentrations of IL-6 than patients with SIRS (P<0.001), sepsis (P<0.001), and healthy subjects (P<0.001), whereas no significant differences were found in comparison with patients having severe sepsis (P=0.067). Patients with severe sepsis had significantly higher serum concentrations of IL-6 (P<0.001) than those of healthy subjects but not significant (P=0.013) when compared with those of sepsis. Patients with sepsis had significantly higher serum concentrations of IL-6 (P>0.001) than those of healthy subjects but not significant (P=0.678) when compared with those with SIRS. Patients with SIRS had serum concentrations of this protein significantly higher (P<0.001) than those of healthy subjects.
Results are expressed as median and standard deviation. P values are from the Mann–Whitney U-test.
Serum lactate and sepsis
Regarding serum lactate, patients with septic shock had significantly higher serum concentrations of IL-6 than patients with severe sepsis, sepsis, SIRS, and healthy subjects (P<0.001). Patients with severe sepsis had significantly higher serum concentrations of IL-6 (P<0.001) than those of patients with sepsis and healthy subjects but not significant when compared with (P=0.061) than those of SIRS. Patients with sepsis had serum concentrations of this metabolite significantly higher (P<0.001) than those of patients with SIRS and healthy subjects.
CRP and sepsis
Regarding serum CRP, patients with septic shock had serum concentrations of this protein that were not significantly different from patients with sepsis (P=0.484) and severe sepsis (P=0.746) but significantly higher than patients with SIRS and healthy subjects (P<0.001). Both the patients with severe sepsis and those with sepsis had significantly higher serum concentrations of CRP (P=0.024 and P<0.001 respectively) than those of healthy subjects.
ROC analysis of serum markers
The ROC curves for serum lactate, IL-6 and CRP in differentiating between patients with severe sepsis and those with sepsis are shown in Fig. 2. The values of the areas under the ROC curves (95% CI) are 0.922(95% CI=0.834–1.009) for serum lactate, 0.912 for IL-6, and 0.719 for serum CRP. The area of serum CRP was significantly lower (P=0.009) than that of serum IL-6 and serum lactate (P<0.001).
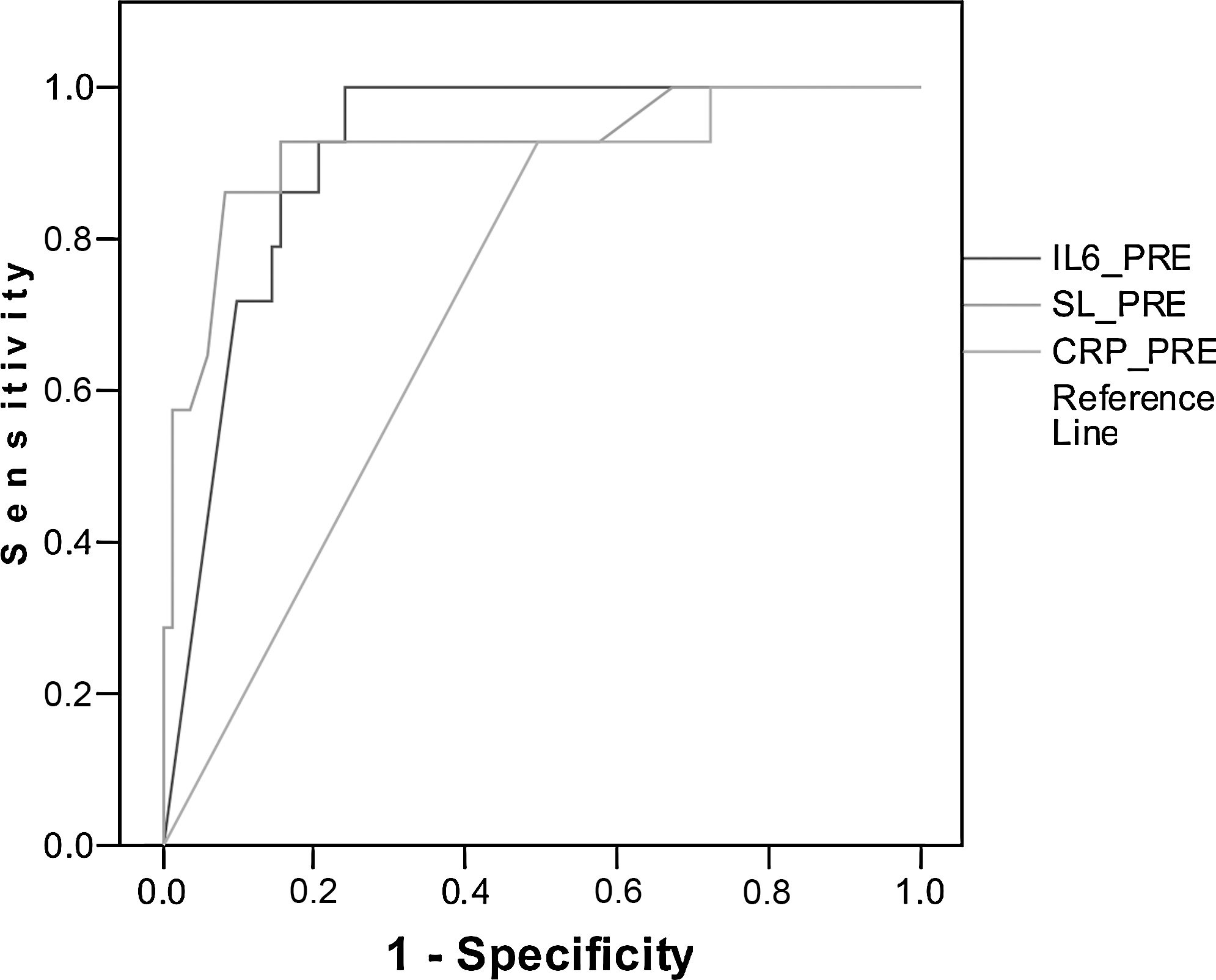
Receiver operating characteristic curves between those with severe sepsis and those with sepsis.
The best cutoff value of IL-6 to differentiate between patients with severe sepsis and those with sepsis ranged from 2,760 to 2,792 pg/mL. The best cutoff value to differentiate patients was 3.9 to 4.2 mM for serum lactate and ranged from 205.7 to 215.3 mg/L for CRP. In using serum lactate to discriminate between patients with severe sepsis and patients with sepsis, a cutoff value <3.9 mM had a sensitivity of 100% and a specificity of 83%. IL-6 (cutoff between 2,760 and 2,792 pg/mL) showed a lower prognostic efficiency than serum lactate: sensitivity of 87% and specificity of 81%. CRP (cutoff between 205.7 and 215.3 mg/L) showed a lower prognostic efficiency than IL-6: sensitivity of 57% and specificity of 46%.
Association between the serum markers
Serum IL-6 levels were positively correlated with serum lactate levels (r 2=0.368, P=0.008) as shown in Fig. 3. Serum lactate did not correlate with CRP levels (r 2=0.173, P=0.786). Similarly, IL-6 did not correlate with CRP levels (r 2=0.234, P=0.436).
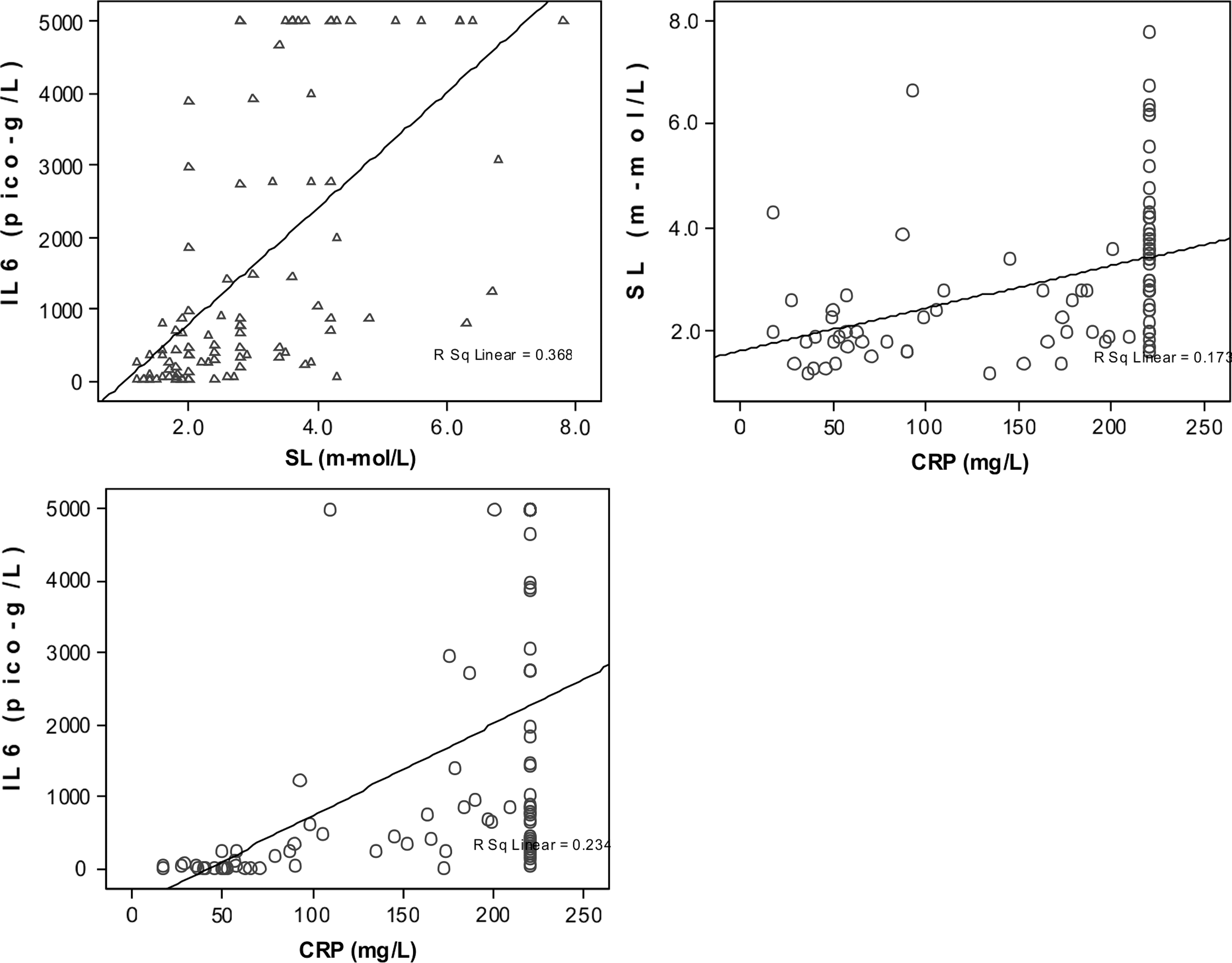
Correlation between the serum markers in acute abdomen.
Discussion
At present, many systems are used in determining the prognosis of acute abdomen. These systems require clinical, laboratory, and radiological assessment of the disease, and none of them are useful for a rapid evaluation of high-risk patients in emergency situations, because they are expensive or time consuming. It has been established that increasing lactate levels signal both developing septic shock and multiple organ failure. Decreasing levels correlate with improvement of the septic state (Boldt and others 2001). It has been reported that serum concentrations of IL-6 increase in patients with inflammatory disorders and in patients with acute abdomen; however, there are no studies that used this molecule to establish the prognosis of acute abdomen at the first initial visit when the patient was in the Emergency Room (Hamilton and others 1992; Berger and others 1997; Goodwin and others 1997; Labib and others 1997). It has also been reported that CRP by itself cannot be used as a marker for acute abdomen (Salem and others 2007). It has been known that the initial sepsis level correlates with the final prognosis of the patient. Thus, by finding an association between the serum markers and the initial septic level of the patient, we may be able to indirectly correlate between the serum markers and the prognosis of the patient. In the present study, we evaluated whether the combined use of serum lactate and IL-6 assays, ie, 2 tests that are quick and easy to perform, is able to serve this purpose. We also compared the sensitivity and the specificity of this combination with that of CRP.
Patients with severe sepsis and sepsis had serum concentrations of all 3 markers significantly higher than those of the healthy subjects. These findings confirm previous studies showing that in patients with acute abdomen there is early involvement of the immune system (Viedma and others 1992; Berger and others 1997; Goodwin and others 1997). We found that serum lactate determination, using the cutoff value (3.9 mM), had a high sensitivity (100%) and specificity (83%) in differentiating between patients with severe sepsis and those with sepsis. IL-6 came next with a sensitivity of 87% and a specificity of 81%. The AUC for serum lactate (0.922), IL-6, (0.912) and CRP (0.719) in differentiating between patients with severe sepsis and those with sepsis also proves the superiority of serum lactate and IL-6.
The combined use of serum lactate and IL-6 would allow us to simultaneously establish the prognosis of patients with acute abdomen (r 2=0.368, P=0.008), whereas the combined use of IL-6 and CRP had a lower performance. These results may be because of the fact that, in patients with acute abdomen, there is an activation of the acute phase response which is more pronounced in the severe form of the disease and involves proinflammatory cytokines such as IL-6 at an early stage (Norman 1998). On the contrary, CRP only indicates the severity of acute abdomen at a later stage, because it requires the activation of cytokines for its synthesis by the liver (Le and Vilcek 1989; Sholmerich 1998).
Serum lactate levels at a given time represent the speed with which lactate is produced by hypoxic tissue minus the speed with which it is taken up and metabolized by unaffected tissues. Lactate is an early indicator of inadequate perfusion and oxygenation and a semiquantitative estimate of tissue oxygen deficiency. It is a very useful tool for admitting and triaging patients, a marker for monitoring resuscitation therapies, and an important prognostic indicator for patient outcome. Hemodynamically stable septic patients have normal lactate levels (ie, sepsis per se is not the cause of hyperlactatemia). However, obstruction/closure of capillary units, as a consequence of septic agents, may lead to increased lactate levels. Of the patients who die of sepsis, 35% succumb to hypotension not responsive to vasopressor agents (septic shock) in the first week, and 55% die of multiple organ failure in the second week. Increasing lactate levels signals both developing septic shock and multiple organ failure. Our study clearly demonstrates the relationship between serum lactate and the septic status of the patient and proves to be a good prognostic indicator for patients with acute abdomen.
IL-6 is a glycoprotein produced by a variety of cells including T- and B-cells and endothelial cells. Production of IL-6 is induced by viruses LPS, IL-1 and TNF. It induces a proliferation of B-lymphocytes with increased synthesis of immune globulins and a proliferation of T-lymphocytes. Further, its main effect is to induce hepatic synthesis of acute-phase proteins such as CRP, fibrinogen, α1-antitrypsin, or complement factors. IL-6 is less transient and, therefore, more readily measurable than either IL-1 or TNF-α. It appears to be one of the best prognostic markers regarding the outcome of patients with SIRS, sepsis, or multiple organ dysfunction syndrome (MODS). Hack and others (1989) reported a direct correlation between IL-6, and levels of lactate in septic shock and IL-6 appeared to have prognostic significance in the differentiation of survivors from those who died (P=0.0003). This study reinforces the usefulness of IL-6 in segregating patients with different levels of sepsis. The combination of IL-6 and serum lactate in prognosticating the patient may prove to be helpful in serving the patient better in an emergency setting.
Limitations
(1) A larger subject group is under study, and the results will be reviewed soon.
(2) The cost of measuring serum markers is at present prohibitive. However, since the effectiveness of the serum markers have been proved, the cost tends to decrease once these measurements are made a routine in laboratory practices.
Conclusion
In conclusion, the results of this study show that in emergency situations, it is now possible to simultaneously establish both the septic status and the prognosis of acute abdomen, thereby immediately aiding in the initiation of intensive treatment. We hope that an IL-6 assay for routine use in emergency situations will be developed in the near future. Additional clinical studies involving a more consistent population of patients with acute pancreatitis are needed to confirm these initial and promising results.
Footnotes
Acknowledgment
The authors wish to acknowledge the help rendered by Dr. Raja Sabapathy, Ganga Hospital, in helping them prepare this article.
Author Disclosure Statement
No competing financial interests exist.