
Abstract
Elevated levels of inflammatory and endothelial biomarkers are related to chronic diseases, cancers, and cardiovascular disease. This study aimed at evaluating the association of inflammatory cytokines and endothelial adhesion molecules with immunological, virological, and cardiometabolic disease in HIV-infected individuals. A cross-sectional study was initiated to evaluate the association of CD4 lymphocyte count, viral load, antiretroviral therapy, and metabolic and cardiovascular disease with inflammatory cytokines [interleukin (IL)-1β, IL-6, and tumor necrosis factor α (TNF-α)], adhesion molecules [soluble intercellular Adhesion Molecule 1 (sICAM) and soluble Vascular Adhesion Molecule 1 (sVCAM)], and highsensitive C-reactive protein (hs-CRP) levels in 125 HIV-infected patients. The associations between independent variables and biomarkers were analyzed by means of multivariate logistic regression. A viral load ≥100,000 copies/mL had a stronger association with high levels of sVCAM-1 (P=0.026; OR=2.54; CI=1.12–5.78) and TNF-α (P=0.048; OR=2.42; CI=1.01–5.85) than the current viral load using a multivariate analysis. Antiretroviral treatment was associated with lower levels of sVCAM-1 (P=0.20; OR=0.20; CI=0.05–0.78), TNF-α (P=0.060; OR=0.22; CI=0.05–1.07), and hs-CRP (P=0.093; OR=0.44; CI=0.17–1.15). CD4 counts <200 cells/mm3 were associated with high IL-6 levels (P=0.013; OR=3.17; CI=1.27–7.91); however, antiretroviral treatment was not associated with IL-6 levels. Metabolic syndrome was associated with high hs-CRP levels, systolic hypertension was associated with IL-6 levels, and family history of coronary disease was associated with TNF-α levels. High biomarker levels were associated not only with viral and immunological characteristics but also with cardiometabolic factors. The maximum viral load attained was an important risk factor for high levels of TNF-α and sVCAM-1. Treatment protected patients from high biomarker levels, except IL-6.
Introduction
E
In addition, although there are substantial data showing that HIV patients present with high biomarker levels, a few studies show the factors associated with abnormal levels of these different biomarkers in this population.
Therefore, we conducted the present study with the objective of determining the factors associated with elevated levels of inflammatory cytokines [IL-1β, IL-6, and tumor necrosis factor α (TNF-α)], adhesion molecules [soluble Intercellular Adhesion Molecule 1 (sICAM), and soluble Vascular Adhesion Molecule 1 (sVCAM)], and hs-CRP in patients with HIV infection with regard to HIV infection and its treatment, metabolic disorders, and cardiovascular disease.
Materials and Methods
Design and patient information
A cross-sectional study was conducted in which HIV-infected patients older than 18 years of age were approached during their outpatient consultation. The patients with infection or who had undergone hospitalization during the previous 3 months were excluded, as were pregnant women and individuals older than 65 years of age. A convenience sample consisting of 125 patients was used.
A questionnaire was administered to the patients to assess their medical history and habits. The patients also underwent physical examinations to evaluate their weight, height, abdominal circumference, and blood pressure levels. The data related to their HIV infection (CD4 count and HIV viral load) and antiretroviral treatment were extracted from their medical files.
This study is a part of the CSV 68/06 Cardiovascular Risk of Antiretroviral Therapy in Adults and Adolescents in Pernambuco/Brasil project and was approved by the research ethics committee of the HUOC/PROCAP (registration number 16/2009; CAAE-0018.0.106.000-09).
Blood sample processing
A blood sample (15 mL) was collected to measure the levels of inflammatory cytokines (IL-1β, IL-6, and TNF-α), adhesion molecules (sICAM-1 and sVCAM-1), and hs-CRP as well as lipid and glucose levels. The frozen samples were sent for multiplex bead array assays (MBAAs) to be performed at the Institute Genesis, São Paulo, Brazil. Before sample aliquots were added to a sample plate for testing, the samples were gently shaken and then centrifuged at 13,200 rotations/min for 10 min at 48°C. Dilutions of the plasma samples and standards were prepared in accordance with the manufacturer's instructions. Two different sets of MBAAs were used: (1) the Lincoplex 3-plex Human Cardiovascular Disease Panel 3 Immunoassay Kit (Millipore, Billerica, MA; HCVD3-67CK) to measure IL-1ß, IL-6, and TNF-α; and (2) the Lincoplex 2-plex Human Cardiovascular Disease Panel 1 Kit (Millipore; HCVD1-67AK) to measure sVCAM-1 and sICAM-1. An instrument based on fluorescent granules (Luminex-100; Luminex Corporation, Austin, TX) was used to read each multiplex plate. The data on the Luminex plates were analyzed using the Milliplex Analyst software v3.4 (Millipore; Vigene Tech, Inc., Boston, MA) and 5 adjustment parameters for the logistic curve. MBAA was used, because it enables multiple cytokine assays to be analyzed from a single serum sample. hs-CRP was measured by means of nephelometry using kits from Beckman Coulter Image Immunochemistry Systems (Brea, CA). Cut-off values were established in accordance with the literature: IL-6 assay ≥0.11 pg/mL (Mochizuki and others 2011); IL-1 β assay >0.08 pg/mL (Mochizuki and others 2011); TNF-α assay >1.2 pg/mL (Bennet and others 2006); sICAM-1 assay ≥502 pg/mL (Luc and others 2003); sVCAM-1 assay ≥710 pg/mL (Luc and others 2003); and hs-CRP assay ≥3.0 mg/L (Zakynthinos and Pappa 2009).
Carotid ultrasound
Measurements were performed on the medial-intimal layer of the anterior and posterior walls of the extracranial segments of the carotids using General Electric Vivid 5 high-resolution equipment (Horten, Norway) and a linear transducer (7.5 MHz) with specific software for studying the left and right carotid arteries. Images of the common carotid arteries, carotid bifurcation, and internal carotids were obtained by means of transversal and longitudinal sweeps. The carotid intima-media thickness CIMT measurement was described as a common-carotid measurement (mean of 3 measurements of the posterior wall of the common carotid). The presence of subclinical atherosclerosis was defined as a CIMT ≥0.8 mm.
Statistical analysis
A case-control analysis was conducted to assess associations between the biological, HIV-related, metabolic, and coronary artery disease risk factors with regard to high biomarker levels. A univariate analysis was performed to determine the association of high levels of each biomarker (sVCAM-1, sICAM-1, TNF-α, IL-6, IL-1β, and hs-CRP) with the variables divided into biological characteristics, laboratory and anthropometric data, HIV-related factors, coronary disease risk factors, and carotid atherosclerosis. The cut-off values cited earlier were used to dichotomize the continuous variables (sVCAM-1, sICAM-1, TNF-α, IL-6, IL-1β, and hs-CRP).
We performed a multivariate analysis in 2 steps. (1) A multivariate analysis of each group was performed to determine the variables that are closely associated with outcome. The variables associated with outcome with P value<0.25 in the univariate analysis were successively included in a multivariate logistic regression model, and those showing an association with a P value≤0.05 remained in the model. (2) The variables selected in the previous step were introduced in the final multivariate model (including variables of all groups), and those with a P value≤0.05 remained in the final model.
We examined the colinearity for those variables, which, in theory, were expected to be associated with each other. The variables that remained in the final multivariate model were examined for interactions.
The data entry and double entry validation were performed in parallel with data collection, and the database was managed by the SQL Server 2000 (Microsoft), using GeneXus software (version 7.5) and STATA version 8.2 for data analysis.
Results
Blood samples were collected from 125 patients, the majority of which were men (60.8%) with a mean age of 42.1±9.5 years. Antiretroviral treatment was being utilized by 102 patients, while 23 had not received treatment. From the 125 patients, 71 (56.8%) presented with an undetectable viral load. High biomarker levels were found in 71 patients (56.8%) for VCAM-1, 4 (3.2%) for ICAM-1, 86 (68.8%) for TNF-α, 92 (73.6%) for IL-6, and 14 (11.2%) for IL-1β. hs-CRP values greater than 3.0 mg/dL were found in 38.4% of the patients.
Univariate analysis on factors associated with increased quantitative and categorized sVCAM-1 levels showed that male sex and a maximum viral load >100,000 copies were associated with high levels of sVCAM-1, while the use of antiretroviral therapy protected from high levels of this cytokine (Table 1). Only 4 samples (3.2%) were found to have above-normal values (≥502 pg/mL) for sICAM-1, and no associations were found between elevated levels of this biomarker and any variable.
Low HDL cholesterol: <40 mg/dL in men and <45 in women; bMen: waist >102 cm; women: waist >88 cm.
Bold numbers indicate a significant P value.
CAD, coronary artery disease; sVCAM-1, soluble Vascular Adhesion Molecule 1.
Elevated TNF-α levels were associated with a maximal viral load >100,000 copies, while an undetectable viral load was protective against high levels of this cytokine. Family history of coronary artery disease was also associated with high TNF-α levels (Table 2). The IL-6 measurements were above the cut-off value (≥0.11 pg/mL) in 92 cases (73.6%). The only factor involved in high IL-6 levels was CD4 count <200 cells/mm3 (nadir and current; Table 3). Elevated IL-1β levels (≥0.08 pg/mL) were found in 14 samples (11.2%), and no factor was found to have a significant association with elevated levels of this cytokine in the univariate analysis. Due to the lack of significant associations in the univariate analysis, no multivariate analysis was performed for this biomarker.
Low HDL cholesterol: <40 mg/dL in men and <45 in women; bMen: waist >102 cm; women: waist >88 cm.
Bold numbers indicate a significant P value.
TNF-α, tumor necrosis factor α.
Low HDL cholesterol: <40 mg/dL in men and <45 in women; bMen: waist >102 cm; women: waist >88 cm.
Bold numbers indicate a significant P value.
hs-CRP levels greater than 1.0 mg/dL were found in 70% of the patients, although 60% of patients presented with undetectable viral loads. The median hs-CRP was 2.2 mg/dL, and the 75th percentile reached a value of 4.5 mg/dL (the cut-off value for inflammatory processes was ≥0.5 mg/dL). In total, 38.4% of patients presented with hs-CRP levels greater than 3.0 mg/dL, which was the cut-off value for a risk of cardiovascular disease. The factors associated with or close to significance for an hs-CRP value greater than 3.0 mg/dL were metabolic syndrome, systolic hypertension, body mass index ≥25, and abnormal abdominal circumference. The length of time of antiretroviral therapy (>5 years) showed a tendency toward hs-CRP values <3.0 mg/dL (OR=0.38; 95% CI=0.12–1.23; P=0.113; Table 4).
Low HDL cholesterol: <40 mg/dL in men and <45 in women; bMen: waist >102 cm; women: waist >88 cm.
Bold numbers indicate a significant P value.
hs-CRP, highsensitive C-reactive protein.
The final multivariate logistic regression model is described in Table 5. The factors associated with increased sVCAM-1 were male sex (OR=2.31; CI 95%=1.01–5.30; P=0.048) and a maximum viral load >100,000 RNA copies/mL (OR=2.54; CI=1.12–5.78; P=0.026). The use of antiretroviral therapy was protective against high levels of sVCAM-1 (OR=0.20; CI=0.05–0.78; P=0.020). The presence of CIMT thickening was not associated with increased sVCAM-1 levels in this analysis. However, when assessed continuously by means of a correlation analysis, the CIMT thickening was shown to be positively associated with sVCAM-1 (β=0.00008; P=0.048). In the final model, it was demonstrated that high TNF-α levels were associated with having attained a viral load ≥100,000 RNA copies/mL (OR=2.42; CI=1.01–5.85; P=0.048) and having a family history of cardiovascular disease (OR=3.12; CI=0.95–10.3; P=0.061). Conversely, the use of antiretroviral therapy was protective against elevated TNF-α levels (OR=0.22; CI=0.05–1.07; P=0.060). It is notable that current viral load and having attained a viral load >100,000 RNA copies/mL were associated with high levels of sVCAM-1 and TNF-α. However, in the multivariate analysis, the association was strongest for the latter; therefore, the current viral load was excluded from the final model for these 2 biomarkers. IL-6 was independently associated with a current CD4 level <200 cells/mm3 (OR=3.17; CI=1.27–7.91; P=0.013) and a systolic arterial pressure ≥140 mmHg (OR=3.35; CI=0.82–13.7; P=0.091); however, there was no association with current viral load, a viral load >100,000 RNA copies/mL, or having used an antiretroviral treatment. The use of antiretroviral therapy for more than 5 years was associated with protection against high hs-CRP levels, while the presence of metabolic syndrome increased the risk of high hs-CRP levels almost 2-fold (OR=1.89).
A model diagram showing HIV-related factors that result in high or diminished levels of IL-6, TNF-α, sVCAM, and CRP and their role in cardiovascular complications is presented in Fig. 1.
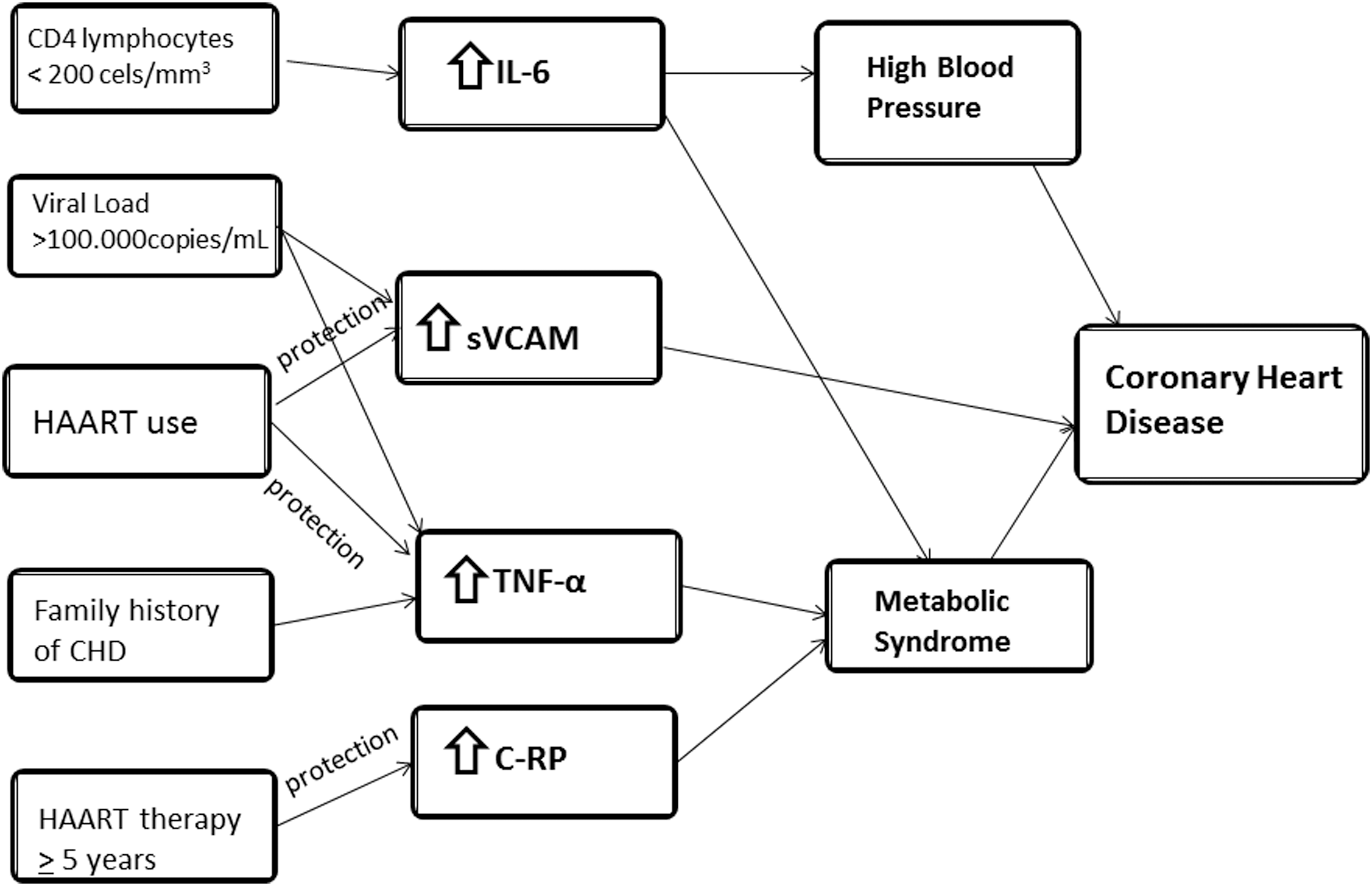
Model diagram of factors associated with risk or protection for high levels of IL-6, sVCAM, TNF-α, and CRP; high blood pressure; metabolic syndrome; and coronary heart disease in patients with HIV infection. IL-6, interleukin-6; sVCAM, soluble Vascular Adhesion Molecule 1; TNF-α, tumor necrosis factor α; CRP, C-reactive protein.
Discussion
The results from the present study demonstrated that the biomarkers studied were elevated in a large proportion of the patients, even though 60% presented with undetectable viral loads at the time of sample collection. Furthermore, the results showed that the maximum viral load attained by the patient had a great bearing on their “inflammatory status”; that is, the maximum viral load reached was more important than the presence of undetectable viral load at the time of the examination, particularly with regard to the elevation of the levels of TNF-α and the endothelial activation marker sVCAM-1. On the other hand, the results also showed that antiretroviral treatment was associated with lower biomarker levels (TNF, sVCAM, IL-1β, and hs-CRP), and this reduction was even more evident after 5 years of antiretroviral treatment. However, the use of antiretrovirals did not protect against elevated IL-6 and hs-CRP levels. CD4 levels lower than 200 cells/mm3 were associated with elevated IL-6 levels. Conversely, metabolic syndrome was associated with elevated levels of hs-CRP, systolic hypertension with IL-6, and family antecedents of coronary artery disease with elevated TNF-α levels.
Cozzi-Lepri and others (2011) described the biomarker behavior in a group of patients from the Strategies for Management of Antiretroviral Therapy (SMART) study, which compared the maintenance of antiretroviral therapy with a structured interruption of therapy. Their study showed that treatment interruption led to a reduction in the numbers of CD4 lymphocytes and significant increases in TNF-α, CXCL10, IL-10, and IL-6 levels, thus simulating acute HIV infection (Cozzi-Lepri and others 2011). Others observed that even under virological control (either through antiretroviral treatment or through the organism's own mechanisms, as occurs in chronic controlled patients who have an undetectable viral load without treatment), the cytokine, endothelial activation, and CRP levels (ie, inflammation) are higher in individuals with HIV infection than in noninfected individuals (Neuhaus and others 2010; Armah and others 2012). These findings agree with our results that show high levels of biomarkers in a large proportion of patients, even those under treatment. Studies have also shown that chronic inflammation is associated with significant consequences with regard to morbidity among infected individuals such as cardiovascular events, bone disease and central nervous system events, and mortality (Kuller and others 2008; Deeks 2011; Mangili and others 2011).
Although some studies have been performed, it remains unclear whether each of the inflammatory cytokines and endothelial cells have similar behaviors and what the determining factors are for each, particularly considering the factors related to HIV and its treatment. Moreover, there is no consensus regarding whether cardiovascular and metabolic disorders are associated with increased cytokine levels in HIV patients as observed in the general population, considering that HIV patients present with many other factors which stimulate inflammation. The individual analysis of each of these markers is one of the advantages of the present study.
Our findings suggest that high levels of sVCAM-1 and TNF-α were clearly linked to having attained a viral load >100,000 copies of RNA/mL at any time over the course of infection. A currently undetectable viral load also appeared to protect patients from high cytokine levels. Indeed, a maximum viral load >100,000 copies of RNA/mL showed a stronger association with sVCAM-1 and TNF-α levels than an undetectable viral load, and this association persisted in the final multivariate model. This original finding reinforces the importance of an early HIV diagnosis. It also shows, from the biomarker viewpoint, the importance of preventing high levels of viremia, as the consequences appear not to be completely reversible with the current antiretroviral therapy.
IL-6 is a pro-inflammatory cytokine with pleomorphic biological effects and is a powerful stimulator of B cells with regulatory action related to the immune system, hematopoiesis, inflammation, and oncogenesis (Kishimoto 2010). In the present study, elevated IL-6 levels were associated with CD4 lymphocyte counts lower than 200 cells, either as the lowest level ever reached or as the current level. This was the only biomarker studied here that was independently associated with CD4 lymphocyte levels. A study by Eastburn showed that elevated viral RNA levels were associated with elevated levels of IL-6 and fibrinogen. However, the association between IL-6 levels and viremia levels was reduced by 50% after adjustment for the CD4 lymphocyte count, thus showing the importance of CD4 lymphocyte levels for this cytokine in that study (Eastburn and others 2011).
The results of an elegant study performed by Regidor and others (2011) agree with our results, indicating that IL-6 levels were not affected by antiretroviral therapy. In that study, which included 290 patients, the serum levels of certain markers normalized after 3 years of therapy use; however, similar to our findings, the serum IL-6 levels did not appear to be affected by the antiretroviral therapy. The authors concluded that there was a state of continuous chronic hyperactivation of B cells that persisted after at least 2 or 3 years after the initiation of antiretroviral therapy (the period analyzed in their study). These findings may partially explain the excess incidence of lymphomas that occur in HIV-positive individuals in the postantiretroviral therapy time (Regidor and others 2011).
Kuller and others (2008) analyzed the cytokine profile of a group of patients in the SMART study (El-Sadr and others 2006), and their results agree with our findings. In the group of patients whose antiretroviral therapy was maintained, the levels of IL-6 were stable; that is, there was no increase or only a small increase in the cytokine levels. However, they discussed another aspect that deserves attention: In the group of patients in whom antiretroviral therapy was interrupted, the levels of IL-6 increased progressively. All of these findings suggest that antiretroviral therapy does not reduce the levels of IL-6 after its elevation but can prevent its increase over time, confirming the importance of the early use of antiretroviral therapy while we await other strategies to reduce chronic immune activation.
A large epidemiological study on elderly people measured the levels of IL-6, CRP, TNF-α, and other biomarkers. Of all the markers evaluated, IL-6 was the most intensely associated with incident diseases, incapacity, and mortality (Singh and Newman 2011). Among HIV-positive individuals, the situation did not appear to differ: The baseline assessment of HIV-positive individuals included in the SMART study, in a case-control study, and after randomization showed that there was a strong association between elevated IL-6 levels and mortality (Kuller and others 2008). This phenomenon was also described by Boulware and others (2011).
A large proportion of the patients in the present study had elevated hs-CRP levels, including levels greater than 3.0 mg/L, which is indicative of a risk for cardiovascular disease (Pearson and others 2003). This finding agreed with the studies by Neunhaus and others (2010), Cozzi-Lepri and others (2011), and Eastburn and others (2011). However, there was disagreement with regard to the associations between high levels of this marker and viral load levels. In the present study, we did not find any association between elevated hs-CRP levels and the viral load. There also appears to be disagreement regarding this topic in the literature. Eastburn conducted an interesting study in which the viral load was stratified into several levels of viremia; this author did not find any direct association between hs-CRP and increasing viral load extracts except for very high viremia extracts (greater than 100,000 copies). Eastburn also drew attention to the extreme variability of hs-CRP values, which was also observed in our study, and hypothesized that other factors could influence the CRP levels in these patients. Another question that remains is the effect of treatment with regard to reducing and normalizing hs-CRP values. In our study, we observed that the levels of hs-CRP were associated with treatment and were reduced in patients who had been receiving treatment for more than 5 years.
Metabolic and cardiovascular factors also modified biomarker behavior: Elevated TNF-α levels were associated with family coronary artery disease; elevated IL-6 levels were associated with systolic hypertension; and hs-CRP was associated with the presence of metabolic syndrome. These findings indicate that, similar to uninfected individuals (Duvnjak and Duvnjak 2009; Scarpellini and Tack 2012), the risk factors for cardiovascular disease among HIV patients are associated with higher levels of inflammation.
The present study has limitations: The study design was cross-sectional, and, therefore, the exposure time coincided with outcome time; the small sample size may have resulted in the failure to show certain associations, particularly in relation to IL-1β; and the variability in cytokine measurements, a phenomenon that has previously been cited in the literature. We believe that these limitations do not compromise the final conclusions.
The main strengths of the study relate to the inclusion of patients with and without the use of antiretroviral therapy, the patients with and without controlled viremia, and the analysis of many factors that could influence outcomes such as risk factors for cardiovascular diseases, which have been associated with elevated cytokine levels (Duvnjak and Duvnjak 2009; Cheung and others 2012; Tete and others 2012). In addition, a separate analysis for each marker made it possible to demonstrate differences in behavioral patterns.
The present study raises certain questions, because other studies with a large number of patients have shown better evolution and lower mortality among patients with early antiretroviral therapy initiation (with higher CD4 levels) (Kitahata and others 2009; Sterne and others 2009). An individual who initiates antiretroviral therapy with a high CD4 count would most likely never achieve CD4 levels lower than 200 cells/mm3, which were associated with high IL-6 levels in our results. Similarly, the patient would not experience high viral loads, possibly never reaching levels above 100,000 copies of RNA/mL, which were associated with high sVCAM and TNF-α levels in our study. The findings from this study support starting antiretroviral therapy early after the detection of HIV infection.
In conclusion, it was demonstrated that cell activation and inflammation continue to occur in individuals with HIV, even when the viral load was suppressed. This occurred particularly when a viral load greater than 100,000 copies was reached at any point during the course of the disease. Antiretroviral therapy was protective against high levels of the biomarkers, and this protection appeared to increase with the length of use, particularly in relation to hs-CRP. In particular, IL-6 correlated with low CD4 levels independently of viral load levels. Emphasis should also be placed on controlling and preventing systolic arterial hypertension and metabolic syndrome, given that these increase the risk of immune activation, which is already present in chronic HIV infection. New strategies to control inflammation are urgently needed to reduce long-term morbidity in patients with HIV.
Footnotes
Acknowledgments
The authors are grateful for the financial support rendered by Ministerio da Saude do Brasil/Programa DST/AIDS/UNESCO (CSV 68/06–Projeto “Risco cardiovascular da terapia anti-retroviral em adultos, adolescentes e crianças em Pernambuco”). The authors are partially supported by CNPq (Scholarship 310911/2009-5 to HRL and Scholarship 301779/2009-0 to MFPMA and Scholarship 308311/2009-4 to RAAX).
Authors' Participation
HRL conceived the study, participated in the design, and co-ordinated and drafted the article. VMGA carried out the carotid ultrasounds. JCZ, MCF, and DBMF recruited, selected, and followed the patients. MFPMA and VMGA prepared the questionnaire. RAAX participated in the design, co-ordinated, and supervised the statistical analysis. UM performed the statistical analysis. All authors read and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.