
Abstract
In this study, preoperative serum levels of insulin-like growth factor 1 (IGF-1) were determined in 216 hepatocellular carcinoma (HCC) patients who underwent hepatic resection to investigate a possible contribution of IGF-1 to the increased risk for HCC recurrence and mortality. During January 2010 and December 2013, 216 HCC patients receiving hepatectomy were recruited. The primary endpoint was the HCC recurrences within the 3-year follow-up. The secondary endpoint was all-cause mortality. The multivariate analyses with Cox regression model were applied to explore the clinical significance of IGF-1 serum levels and associated parameters on death and recurrence of HCC patients. The IGF-1 levels of included patients were determined, with a median value of 75.5 ng/mL (IQR, 40.3–93.0 ng/mL). The preoperative serum level of IGF-1 was negatively correlated with tumor size, Child–Pugh class, or tumor stage (P < 0.001 for all). In multivariate models comparing the first, second, and third quartiles with the fourth quartile of IGF-1, the levels of IGF-1 in Q1 and Q2 were associated with HCC recurrence, with an increased risk of 216% [hazard ratios (HR) = 3.16 (95% CI: 1.79–4.28)] and 106% [3.02 (1.36–3.11)]. Similarly, concentrations of IGF-1 in Q1 and Q2 were also related to all-cause mortality, with an increased recurrence risk of 238% [HR = 3.38 (95% CI: 1.85–4.36)] and 117% [3.02 (1.40–3.21)], respectively. Poor prognosis in HCC patients receiving hepatectomy could be indicated by low preoperative serum levels of IGF-1, which would be applied as a predictor.
Introduction
B
Insulin-like growth factor (IGF)-1, was mainly secreted by the liver, which made critical effects on promoting and regulating cell growth (Hung and others 2014). IGF axis has been proved to play significant roles in tumorigenesis with both experimental and epidemiologic evidence (Sandhu and others 2002). Previous studies (Stuver and others 2000; Rehem and El-Shikh 2011) reported a decreased serum level of IGF-1 in HCC, which was different from the increased tendency reported in other cancers (Renehan and others 2004). Mazziotti and others (2002) suggested a significantly decreased serum level of IGF-1 in HCC development, for those patients with hepatitis C virus (HCV)-related cirrhosis.
Interestingly, previous studies had presented that serum level of IGF-1 was a predictor for prognosis after surgical removal in HCC patients (Liu and others 2016; Yao and others 2017). Furthermore, in a retrospective study on HCC patients, a significant relationship was observed between expression level of IGF-1 and liver cirrhosis or survival after surgery. In addition, this relationship was independent of underlying liver diseases of patients (Chun and others 2014). Thus, we assumed that the preoperative IGF-1 level in serum may be related to prognosis of HCC in Chinese Han population. In this study, preoperative serum levels of IGF-1 were determined in 216 patients with HCC, who received hepatic resection to investigate a possible contribution of IGF-1 to the increased risk for HCC recurrence and mortality.
Patients and Methods
Patients
During January 2010 and December 2013, 308 patients with HCC were recruited, who received hepatectomy without any previous anti-cancer treatment in our hospital. HCC was confirmed by histological diagnosis. Exclusion criteria included the following: (1) had other malignancies (n = 8); (2) died within 30 days after surgery (n = 18); (3) lost during the 3-year follow-up (n = 28); (4) had neurological disorders (Parkinson's disease, stroke, and Alzheimer's disease; n = 22); and (5) failed to provide the informed consent or lost blood samples (n = 16). This prospective cross-sectional study involving human subjects was reviewed by the Institutional Review Board of our hospital. The written informed consent, including background and procedures of this study, was obtained from all the patients.
Clinical information and surgical treatment
Age, sex, general conditions (HBsAg-positive status, HCV Ab-positive status, and first-degree history of LCC), pathological parameters, as well as clinical biomarkers [number of tumors, tumor size, present cirrhosis, vascular invasion, distant metastasis, presence of portal vein thrombosis (PVT), and lymph node involvement] were all collected. Each patient was classified based on the 3 Child–Pugh's grades (Hashimoto and others 2005). Besides, according to the modified tumor node metastasis (TNM) staging criteria, tumor staging was established (Pugh and others 1973). Vascular invasion was determined by pathological examination toward the removed samples, which was defined as portal vein or hepatic vein invasion. Indications for hepatectomy were determined with multiple approaches, including preoperative diagnostic imaging, intraoperative ultrasonography, and liver function assessment. The removal of 3 or more liver segments was considered to be major hepatic resection.
Laboratory testing
Following an overnight fast, venous blood samples of each subject were taken early morning. Blood samples in the tubes were stored at 20°C for 15 min and centrifuged at 1,200 g, thereafter, the serum samples were stored frozen in plastic vials at −80°C for further consecutive analyses. The IGF-I and α-fetoprotein (AFP) levels of patients were determined with standard methods generally applied in our hospital (Immulite 2000, CA). In this method for IGF-I, the detection range was 15–1600 ng/mL, with intra-and inter-assay variation coefficients of 1.0%–2.4% and 1.6%–2.8%, respectively. The IGF-I level was also determined in 100 normal healthy populations with a median of 160 ng/mL. Other physical markers were also analyzed per standard method (Roche Cobas Integra 800 analyzer), including serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), and high-sensitivity C-reactive protein (Hs-CRP). For all measurements, undetectable levels were preset to the lower limit in the experiment.
Patient follow-up in the following 3 years
The physical examination was performed on all included patients. The follow-up after surgery lasted for 3 years, with an interval of 3 months in the first 2 years and 6 months in the third year. The biochemical analysis of several markers was determined, as well as dynamic computed tomography (CT) or magnetic resonance imaging (MRI). If a lesion was observed with typical radiological features of HCC, which was also confirmed with CT or MRI, it was considered recurrence. Angiographic examination was done in case of strong suspicion of disease recurrence. Once the recurrence was confirmed, further treatment should be performed, such as hepatic resection, radiofrequency ablation, or transarterial chemoembolization. The primary endpoint was the HCC recurrence within the follow-up. The secondary endpoint was all-cause mortality. The overall survival (OS) was recorded in all included patients, defined as from surgery to death, or for surviving patients; the data were censored on the data of the final follow-up.
Statistical analysis
The categorical variables were expressed as percentages and continuous variables were expressed as medians [interquartile ranges (IQR)]. According to whether the data were normal or non-normal distribution, chi-square test was applied for the comparison. Besides, Spearman's rank-correlation coefficient assessment was applied for analyzing correlations among continuous variables. For the not normally distributed data, the comparison between groups was performed with Mann–Whitney U test.
The overall prognostic accuracy of detected biomarkers was summarized by the receiver operating characteristic (ROC) curves, with the area under the curve (AUC) calculated. The cutoff of IGF-1 levels for predicting HCC recurrence and mortality was also determined by ROC. The clinical significance evaluation of adding IGF-1 to existing biomarker panels was performed with integrated discrimination improvement (IDI) and net reclassification improvement (NRI) indices, mainly for improving recurrence and mortality prediction of HCC patients (Pencina and others 2008). Multivariate analyses were applied for evaluating the relative clinical significance of serum levels of IGF-1 and other clinical variables on prognosis. The Cox regression analysis was applied to calculate crude and multivariate hazard ratios (HR) after adjusting for all significant predictors (included age, sex, HBsAg-positive status, HCV Ab-positive status, first-degree history of LCC, number of tumors, tumor size, present cirrhosis, vascular invasion, distant metastasis, presence of PVT, lymph node metastasis, Child–Pugh class, TNM stage, and blood levels of ALT, AST, total bilirubin, AFP, and Hs-CRP). For further investigating the effects of IGF-1 on 2 endpoints, adjusted HR and 95% CIs for IGF-1 quartiles were evaluated and compared (with highest IGF-1 quartile as reference). The Kaplan–Meier curve was applied for calculating the cumulative OS, which was further compared with a log-rank test. All statistical analysis in this study was performed with SPSS (SPSS, Inc.). The P < 0.05 was considered to be significant.
Results
Patient characteristics at the baseline
In our study, among the 308 screened eligible HCC patients receiving hepatectomy, 216 patients were finally included and completed 3 years of follow-up. As shown in Table 1, overall median of age was 54 years (IQR, 46–63) and 51.9% were men. The median of IGF-1 levels was 75.5 ng/mL (IQR, 40.3–93.0 ng/mL) for these patients. The information of patients at baseline was provided (Table 1).
Serum IGF-1 levels in Quartile 1 (<40.3 ng/mL), Quartile 2 (40.3–75.5 ng/mL), Quartile 3 (75.6–93.0 ng/mL), and Quartile 4 (>93.0 ng/mL).
p-value was assessed using Mann–Whitney U test or Chi-square test.
Tumor was staged according to the American Liver Tumor Study Group modified TNM staging classification.
AFP, α-fetoprotein; ALT, alanine aminotransferase; AST, aspartate transaminase; HCC, Hepatocellular carcinoma; HCV, hepatitis C virus; Hs-CRP, high-sensitivity C-reactive protein; IGF-1, insulin-like growth factor 1; IQR, interquartile ranges; PVT, portal vein thrombosis; TNM, tumor node metastasis.
Associations between baseline serum IGF-1 and patient characteristics
A negative association was observed between IGF-1 and Child–Pugh class (r = −0.286, P < 0.001), as well as between IGF-1 and tumor stage (r = −0.326, P < 0.001). Furthermore, as shown in Table 1, patients with lower levels of IGF-1 (in the Q1 range) were older and more likely with HCV Ab-positive status, multiple lesions, vascular invasion, distant metastasis, presence of PVT, and lymph node metastasis. However, other factors, such as sex, infection time, HBsAg-positive status, tumor size, cirrhosis state, total bilirubin, and AFP, were all detected to have no apparent influence regarding serum IGF-1 level (all P > 0.05).
IGF-1 and recurrence risk after surgery
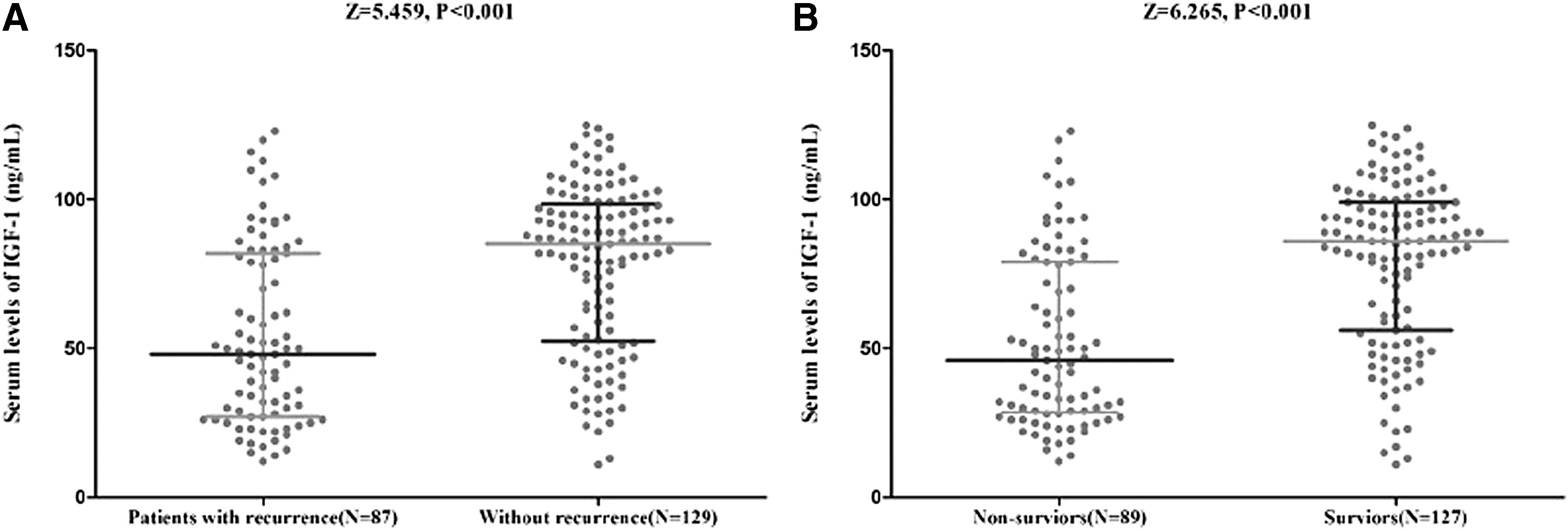
In the follow-up that lasted for 3 years, HCC recurrence and all-cause mortality were analyzed for all patients. There were 87 patients (40.3%, 95% CI: 33.7%–46.8%) who had HCC recurrence. Referred to the IGF-1 quartiles, the recurrence distribution was ranged from 66.7% (Q1) to 18.5% (Q4), Fig 1. Patients with HCC recurrence had significantly lower serum IGF-1 levels than those without [48.0 (IQR, 27.0–82.0) ng/mL versus 85.0 (IQR, 52.5–98.5) ng/mL; P < 0.001; Fig. 2A].
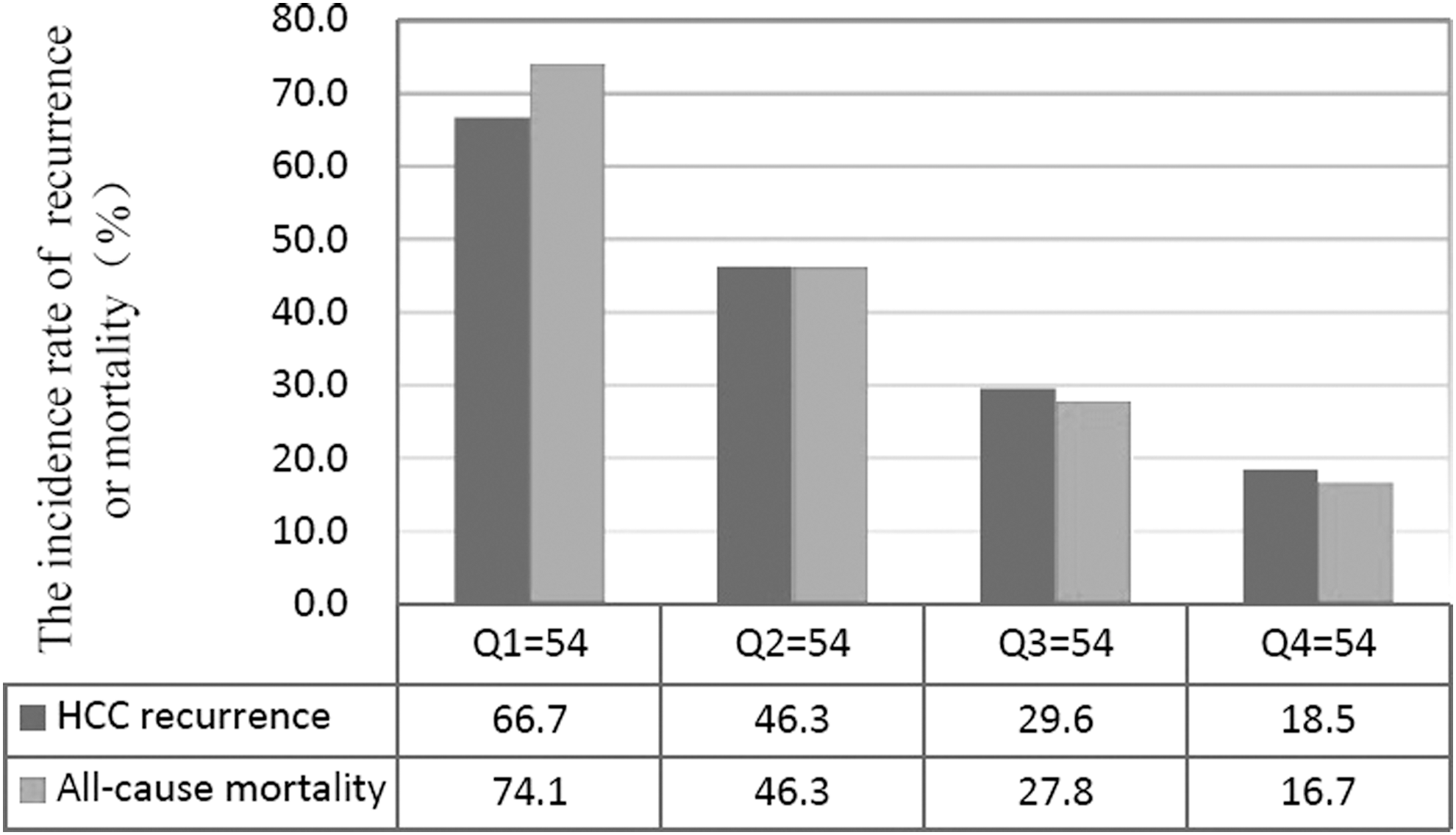
The incidence for HCC recurrence and all-cause mortality according to the baseline IGF-1 quartiles. Serum IGF-1 levels in Quartile 1 (<40.3 ng/mL), Quartile 2 (40.3–75.5 ng/mL), Quartile 3 (75.6–93.0 ng/mL), and Quartile 4 (>93.0 ng/mL). HCC, hepatocellular carcinoma; IGF-1, insulin-like growth factor 1.
Serum IGF-1 levels in different groups.
The odds ratio (OR) of IGF-1 level was compared with the AFP and other risk predictors with univariate Cox regression analysis. The unadjusted OR between IGF-1 and HCC recurrence was 0.95 (95% CI: 0.93–0.97; P < 0.001), indicating a strong association. The adjusted HR was 0.97 after adjusting for all other significant risk factors (95% CI: 0.96–0.98), Table 2. The result indicated that IGF-1 remained to be an independent biomarker for outcome prediction. In addition, age, Child–Pugh status, TNM stage, AFP, and Hs-CRP remained significant outcome predictors, unlike all others assessed (Table 2). In multivariate models comparing the Q1, Q2, and Q3 against the Q4 of IGF-1 (Table 3), concentrations of IGF-1 in Q1 and Q2 were associated with HCC recurrence, and risk of recurrence was increased by 216% [HR = 3.16 (95% CI: 1.79–4.28)] and 106% [3.02 (1.36–3.11)]. The result of likelihood ratio test confirmed independent association of IGF-1 with HCC recurrence (P < 0.001). Furthermore, in a multivariate model analyzing the IGF-1 (Q1) versus Q2–4 together with the clinical variables, the result indicated the prognostic significance of IGF-1 (HR = 4.35; 95% CI: 2.26–8.39).
Adjustment by age, sex, HBsAg-positive status, HCV Ab-positive status, first-degree history of LCC, number of tumors, tumor size, present cirrhosis, vascular invasion, distant metastasis, presence of PVT, lymph node involvement, Child–Pugh class, TNM stage, blood levels of ALT, AST, total bilirubin, AFP, Hs-CRP, and IGF-1.
CI, confidence interval; HBV, hepatitis B virus; HR, hazard ratios.
Adjustment by age, sex, HBsAg-positive status, HCV Ab-positive status, first-degree history of LCC, number of tumors, tumor size, present cirrhosis, vascular invasion, distant metastasis, presence of PVT, lymph node involvement, Child–Pugh class, TNM stage, blood levels of ALT, AST, total bilirubin, AFP, Hs-CRP, and IGF-1.
Serum IGF-1 levels in Quartile 1 (<40.3 ng/mL), Quartile 2 (40.3–75.5 ng/mL), Quartile 3 (75.6–93.0 ng/mL), and Quartile 4 (>93.0 ng/mL).
P tread <0.001.
OR, odds ratio.
In an ROC analysis of HCC recurrence during the follow-up (3 years), based on the ROC curve, the optimal cutoff value of serum IGF-1 levels as an indicator for screening of recurrence was estimated to be 117.5 ng/mL, which yielded a sensitivity of 48.4% and a specificity of 95.4%, with the AUC at 0.66 (95% CI: 0.57–0.74), Fig. 3A. Interestingly, the AUC was improved from 0.76 to 0.82 (95% CI: 0.78–0.86) after adding IGF-1 serum level to clinical examination variables. This AUC difference between the clinical variables without or with IGF-1 was significant [difference, 0.06 (95% CI: 0.04–0.08); P = 0.01]. The NRI statistic results indicated that, after adding IGF-1 to established risk factors, the rate was significantly increased for classifying HCC recurrence and non-HCC recurrence patients (P = 0.006). The IDI statistic results suggested that the discrimination between HCC recurrence patients and non-HCC recurrence patients could be significantly improved with the IGF-1 level (P = 0.01).
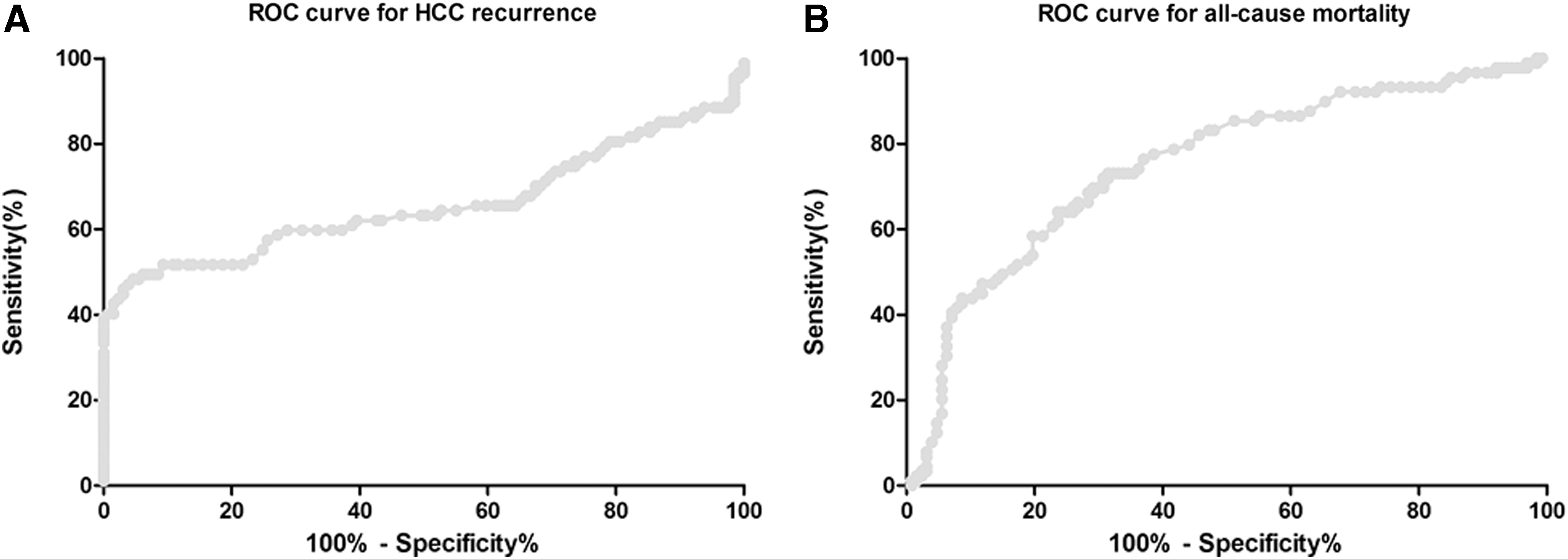
ROC curves were utilized to evaluate the accuracy of serum IGF-1 levels to predict outcomes.
Associations of baseline serum IGF-1 levels with all-cause mortality
In the follow-up that lasted for 3 years, 89 patients (41.2%, 95% CI: 34.6%–47.8%) died. The all-cause mortality across the IGF-1 quartiles ranged from 74.1% (Q1) to 16.7% (Q4), Fig. 1. IGF-1 serum levels in patients who died were significantly lower as compared with patients who survived (46.0 [IQR, 28.5−79.0] versus 86.0 [IQR, 56.0−99.0] ng/mL; P < 0.001; Fig. 2B).
The OR of IGF-1 level compared with the AFP and other predictors was calculated with univariate Cox regression analysis. The unadjusted OR between IGF-1 and all-cause mortality was 0.94 (95% CI: 0.92–0.96; P < 0.001), indicating a strong association. The adjusted HR was 0.96 (95% CI: 0.95–0.97) after adjusting for all other significant predictors. The result suggested IGF-1 as an independent all-cause mortality biomarker, Table 2. In addition, age, Child–Pugh status, TNM stage, AFP, and Hs-CRP were still significant biomarkers for mortality prediction, unlike all others assessed (Table 2). The Q1, Q2, and Q3 of IGF-1 was compared with Q4 in multivariate models (Table 2); concentrations of IGF-1 in Q1 and Q2 were related to all-cause mortality, and the recurrence risk was increased by 238% [HR = 3.38 (95% CI: 1.85–4.36)] and 117% [3.02 (1.40–3.21)]. The results of likelihood ratio test confirmed an independent association between IGF-1 and mortality (P < 0.001). Furthermore, in a multivariate model analyzing the IGF-1 (Q1) versus Q2–4 together with the clinical variables, the result indicated the prognostic significance of IGF-1 (HR = 6.59; 95% CI: 3.29–13.20).
In an ROC analysis of mortality during the follow-up (3 years), based on the ROC curve, the optimal cutoff value of serum IGF-1 levels as an indicator for screening of all-cause mortality was estimated to be 72.5 ng/mL, which yielded a sensitivity of 73.1% and a specificity of 68.5%, with the AUC at 0.75 (95% CI: 0.68–0.83), Fig. 3B. Interestingly, the AUC was increased from 0.78 to 0.85 (95% CI: 0.81–0.89), after adding IGF-1 serum level to clinical examination variables. This AUC difference between the clinical variables without or with IGF-1 was significant [difference, 0.07 (95% CI: 0.05–0.09); P = 0.008]. The NRI statistic results indicated that, after adding IGF-1 to established risk factors, the rate was significantly increased for classifying all-cause mortality patients and survivors (P = 0.003). The IDI statistic results suggested that the discrimination between all-cause mortality patients and survivors could be significantly improved with the IGF-1 level (P = 0.007).
The Kaplan–Meier estimates of all-cause mortality stratified by baseline serum IGF-1 quartile are shown in Fig. 4. The OS was significantly longer in patients with higher serum IGF-1 level compared with lower IGF-1 (P < 0.001; log-rank test).
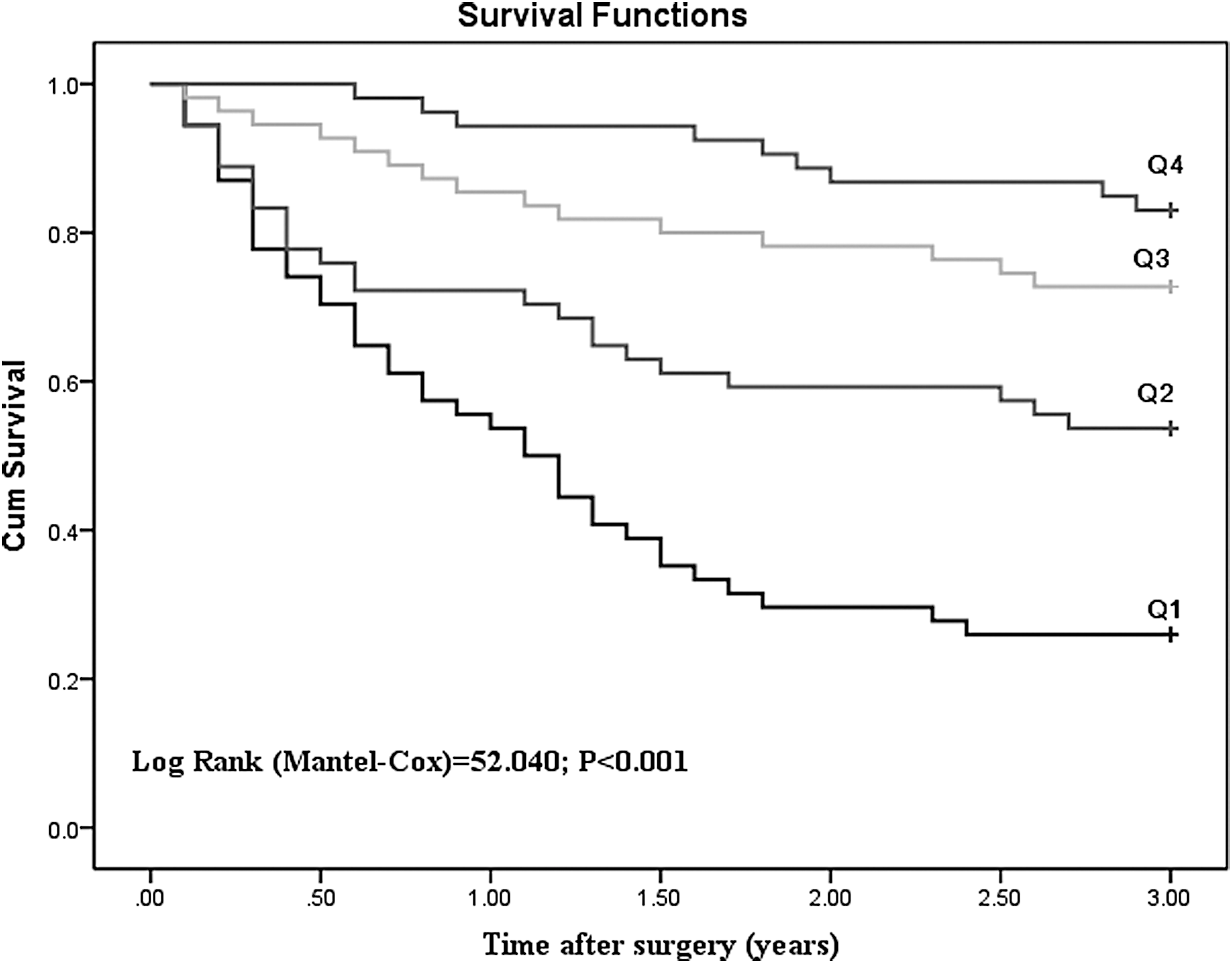
Kaplan–Meier survival of HCC based on IGF-1 quartiles. Serum IGF-1 levels in Quartile 1 (<40.3 ng/mL), Quartile 2 (40.3–75.5 ng/mL), Quartile 3 (75.6–93.0 ng/mL), and Quartile 4 (>93.0 ng/mL).
Discussion
The IGF axis made significant roles in HCC, which have been confirmed in both cell lines and animal xenograft models. In this study, high risk of recurrence events and all-cause mortality of HCC patients after hepatectomy could be independently predicted by low serum IGF-1 levels before operation (defined as less than Q1). These results suggested that serum level of IGF-1 was readily clinically significant and valuable in prognosis prediction.
Previous studies had suggested the relationship between serum IGF-1 levels and HCC risk and prognosis. Compared to Child-Turcotte-Pugh (CTP) score, IGF-CTP score was reported to be facile, blood based, and cost-effective, with better performance on HCC classification (Kaseb and others 2014). Another study reported that IGF-1 in serum could be a simple, low cost, and noninvasive marker for HCC patients with cirrhosis (Ibrahim and others 2013). In this study, we found that concentrations of IGF-1 in Q1 and Q2 were associated with HCC recurrence, against the fourth quartile of IGF-1. Consistent with our results, a low preoperative circulating IGF-1 level had been suggested significantly related to an improved risk of early recurrence in HCC patients (Yao and others 2017). Furthermore, Cho and others (2014) described that low baseline IGF-1 levels were an independent biomarker for poor survival (P = 0.045). Similarly, in this study, the data illustrated that level of IGF-1 in Q1 and Q2 was associated with all-cause mortality against the Q4 of IGF-1 (Table 2). In addition, another study was focused on the patients experiencing curative therapy for early-stage HCC. The result indicated that lower serum levels of IGF-1 at baseline were independently related to a shorter recurrence time and poorer OS (Cho and others 2013). However, Karabulut and others (2014) obtained a different conclusion that neither serum IGF-1 protein nor serum IGF-1 mRNA made significantly adverse effects on survival (P = 0.53 and 0.42, respectively) in HCC.
The low level of IGF-1 in HCC could be resulted from reduced synthetic capacity of hepatic mass or reduced growth hormone stimulation (Su and others 1989). In this study, we also found that IGF-1 level in the HCC was lower than in healthy cases (75.5 ng/mL versus 160 ng/mL). Hepatic damage may contribute to the reduced circulating IGF-1 in patients with cirrhosis or HCC, because hepatocytes were the main producers of IGF-1 (Liu and others 2015). Some studies suggested that hepatic damage could only partially contribute to the reduced IGF-1 level (Hung and others 2014). Stuver and others (2000) observed that, after managing the degree of hepatic damage, reduction of serum IGF-1 levels in HCC patients was not largely affected by this issue.
Furthermore, tissue hypoxia would be enhanced with IGF-1, and tumor growth and metastasis may be promoted (Catrina and others 2006). However, the association between IGF-1 axis and HCC has been different from that with other tumors, since the circulating IGF-1 has been largely originated from liver. Therefore, liver function was directly reflected by IGF-1 levels, which were negatively related to the severity of chronic liver diseases (Assy and others 2008). However, the levels of IGF-1 were still significant biomarkers for indicating progression and death, independent of remaining liver function and traditional stepwise parameters. Low IGF-1 level may also result in the development of cirrhotic features by promoting proinflammatory and profibrogenic responses (Conchillo and others 2005; Sobrevals and others 2010). Inflammatory microenvironment, advanced hepatic fibrosis and cirrhosis would be essential in carcinogenesis and development of HCC (Hoshida and others 2008; Yang and others 2011), and those factors could contribute to the higher recurrence and mortality rates in patients with low IGF-1 levels.
There were some limitations in this study. First, this was a single-center study with a small sample size (N = 216). Second, the follow-up was short and event number was small; thus, the effects of IGF-1 on OS were not fully explored. Third, this was an observational study, and therefore causality cannot be inferred. Last, other circulating factors on IGF axis was not evaluated, including IGF-2 and IGF binding protein 3 (IGFBP-3), which was the main IGF-1 binding protein plasma carrier. Interestingly, a previous study suggested that IGFBP-3 functions like a tumor suppressor gene; it may be used as a therapeutic target for HCC (Hanafusa and others 2002).
Conclusion
Poor prognosis could be predicted with low preoperative serum IGF-1 levels in HCC patients receiving hepatic resection, and serum IGF-1 levels may be applied as a biomarker in the future. Further studies would be required to confirm this relationship based on the existence of limitations. These biomarkers may also be applied as available targets for designing individual strategies to treat these patients.
Compliance with Ethical Standards
Research involving human participants and/or animals
This prospective cross-sectional study involving human subjects was approved by the Institutional Review Board of the First Affiliated Hospital of Jiaxing University.
Informed consent
All patients received written information concerning the background and procedures of the study, and the patients or their relatives gave written informed consent before entering the study.
Footnotes
Acknowledgment
This study was supported by General Surgery of Jiaxing Medical Key Discipline (04-F-15). We are grateful to the nurses, physicians, and patients who participated in our study, and the staff of the central laboratory of the Hospital. All authors have contributed significantly, and all authors are in agreement with the content of the article.
Author Disclosure Statement
No competing financial interests exist.