
Abstract
Color images are available online.
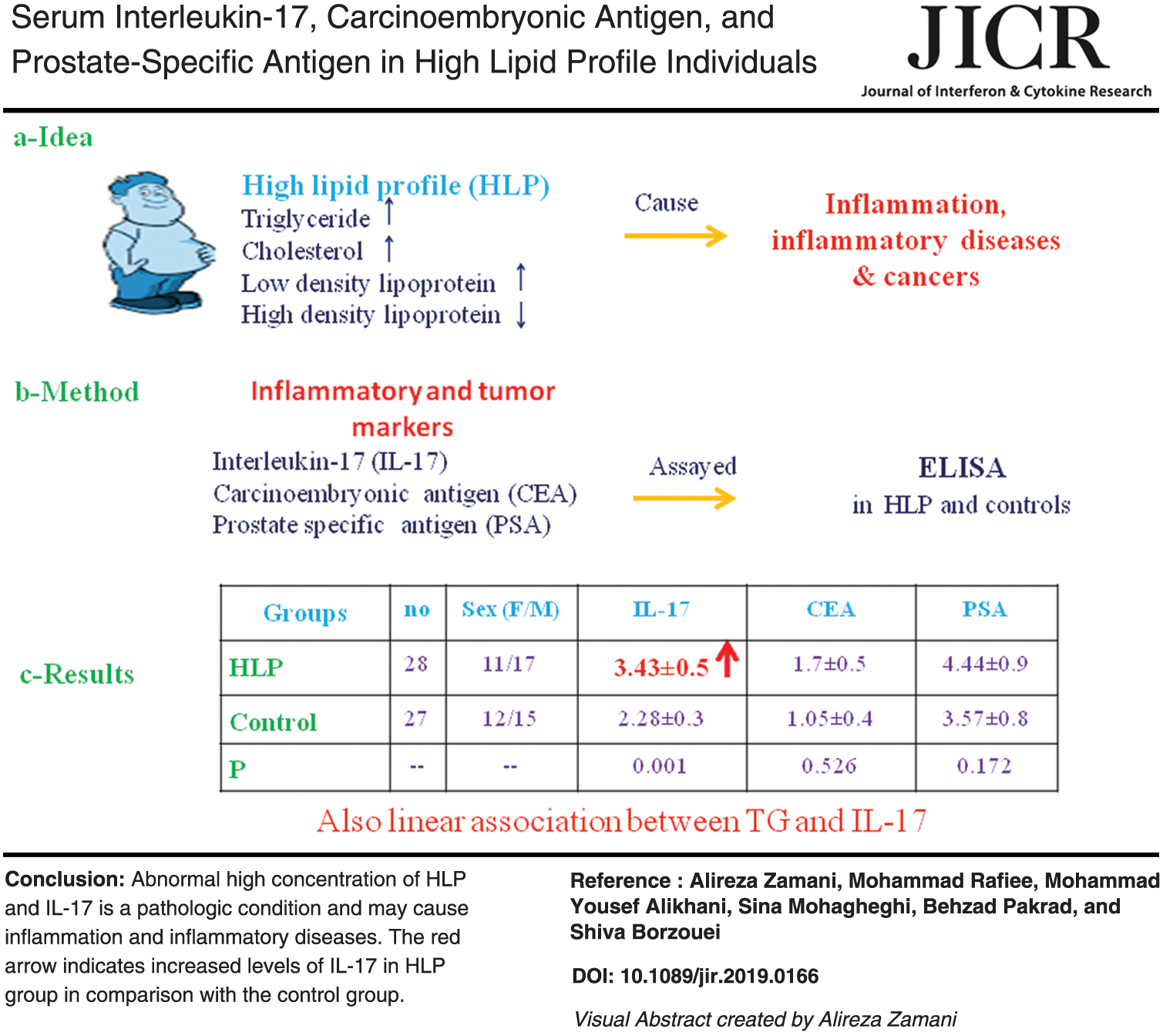
It is assumed that high lipid profile (HLP) causes chronic systemic inflammation, which ultimately leads to inflammatory diseases and cancers. The aim of the study was to investigate the serum concentration of proinflammatory/tumor markers of interleukin-17 (IL-17), carcinoembryonic antigen (CEA), and prostate-specific antigen (PSA) in HLP. HLP cases [F/M: 11/17 triglyceride (TG) >200 mg/dL, high-density lipoprotein (HDL) <50 mg/dL for females and HDL <40 mg/dL for males] and controls (F/M: 12/15, TG <200 mg/dL) were included. The volunteers with diabetes, high blood pressure, infection, cancer, inflammation, smoking addiction, drug consumption, and pregnancy were excluded. Serum TG, cholesterol, HDL and low-density lipoprotein were measured by routine biochemical procedures. The serum levels of IL-17, CEA, and PSA (only in men) were determined by enzyme-linked immunosorbent assay (ELISA). Independent samples t-test was used to compare the data in 2 groups and association between the variables tested by Pearson correlation. IL-17 in HLP group was statistically higher compared with the controls (3.43 ± 0.5 versus 2.28 ± 0.3 pg/mL, P < 0.001). The serum levels of CEA and PSA were not different in the HLP and controls. There was also a statistically positive linear association between TG and IL-17. In conclusion, abnormal high concentration of HLP and IL-17 could be a pathological condition and may cause to increase the chronic systemic inflammation and inflammatory diseases.
Introduction
Today, due to unhealthy lifestyle and diet, the majority of the population has high lipid profile (HLP). Recent studies have revealed that HLP is related to release of some proinflammatory mediators. These mediators may involve in some diseases such as chronic systemic inflammation, cardiovascular diseases, and cancers. Although there are some studies about the relationship between HLP and these proinflammatory factors, they are not sufficient (Han and others 2008; Lee and others 2012; Welty 2013; Perez and others 2019). Therefore, this study aimed to investigate serum interleukin-17 (IL-17), carcinoembryonic antigen (CEA), and prostate-specific antigen (PSA) levels in HLP individuals.
IL-17 family includes six members of IL-17A, B, C, D, E, and F. IL-17A is the most important member of them and is one of the most inflammatory cytokine that is secreted by T helper 17 (Th17), natural killer, γδT cells, and neutrophils. IL-17 activates some transcription factors such as nuclear factor kappa-β (NF-κβ), activator protein 1 (AP1), and CCAAT/enhancer-binding protein (C/EBP) that upregulate the expression of some other proinflammatory cytokines genes. Therefore, overproduction of IL-17A may induce inflammation and plays a critical role in the inflammatory diseases. Also, it seems that high and pathological production of IL-17A in serum is associated with high levels of lipid profiles and may have possible roles in the pathogenesis of the diseases (Yu and others 2014; He and others 2017).
CEA is an inflammatory mediator and tumor marker that is elevated during inflammatory conditions and some malignant tumors, especially in colorectal cancers (Kerr and others 2018). Two in vitro studies have shown that CEA stimulated monocyte and macrophage cell lines and caused to increase the production of other proinflammatory cytokines such as tumor necrosis factor-α, IL-1β, and IL-6. These implicate the role of CEA in the inflammation and may relate to tumor development (Ganguly and others 2003; Aarons and others 2007). There is also some evidence that high level of CEA in serum may also be related to insulin resistance and metabolic syndrome in obesity (Kim and others 2011; Lee and others 2011). Serum high TG levels were positively related to serum CEA concentration too (Lee and others 2012; Esteghamati and others 2014). In contrast, a study on healthy Chinese males showed a negative correlation between serum CEA concentration and body mass index (BMI) (Li and others 2014).
Early detection of serum PSA is the most clinically useful tumor marker for the diagnosis and following of the treatment outcomes in prostate cancer (Mottet and others 2017). Serum PSA is also positively correlated with systemic inflammation (Kandirali and others 2007). A cohort study revealed that neutrophil count and neutrophil/lymphocyte ratio were positively correlated with PSA levels (Yun and others 2017). Some investigations showed a positive correlation between serum high level of TG and HLP with prostate cancer and high level of PSA test (Wuermli and others 2005; Adams and others 2019). However, there is scanty data about their relationship (Han and others 2008; Liu and others 2011).
Owing to scarce studies regarding HLP linkage with IL-17, CEA, and PSA concentrations in serum, the study was designed. In this study, individuals who underwent general health screening were selected and divided into HLP, and normal profile lipid groups and their sera were analyzed for IL-17, CEA, and PSA.
Materials and Methods
Participants
Twenty-eight adult volunteers who attended to Arad Clinical Diagnostic Laboratory (Hamadan, Iran) for general health screening (F/M: 11/17) with high triglyceride (TG >200 mg/dL) and low level of high-density lipoprotein (HDL <50 mg/dL for females and HDL <40 mg/dL for males) were included in the study as HLP group. Twenty-seven adult volunteers (F/M: 12/15) with normal TG (<200 mg/dL) were also recruited as control. The participants were healthy, and there was no statistical difference in gender and age between the 2 groups. The participant had no diseases such as diabetes, high blood pressure, infections, cancer, and inflammation. They were not also addicted to smoking, drug consumers, and pregnant. All the protocols of the study were approved by the Committee of Ethics for Hamadan University of Medical Sciences, Hamadan, Iran (Code:
Blood collection
Five milliliters of peripheral blood of each fasting participant was collected to prepare the serum. The samples were centrifuged at 2000 g for 20 min, and the sera were isolated. The lipid profile parameters were measured by routine biochemical procedures in Arad Clinical Diagnostic Laboratory (Hamadan, Iran) by Roche Hitachi 912 autoanalyzer (Hitachi, Japan).
IL-17, CEA, and PSA assay
The serum levels of IL-17, CEA, and total PSA (only in men) were determined by enzyme-linked immunosorbent assay (ELISA) according to the manuals of the kits. The kit's sensitivity for IL-17A was 0.5 pg/mL (eBioscience, Norway). The sensitivities of CEA and PSA kits were 1 and 0.013 ng/mL, respectively (Monobind, Inc.). All the assays were carried out in duplicate (Shahriari and others 2011; Zamani and others 2017).
Statistical analysis
The mean of the data in the 2 groups was analyzed by independent samples t-test. Pearson correlation, curve estimation, and linear regression tests were also performed among the measured parameters. The P values <0.05 were considered to be significant. Statistical analysis was performed by SPSS 16 package (SPSS, Inc., IL). Data were expressed as means ± standard deviation.
Results
Results of the independent samples t-test analysis of TG, cholesterol (Chol), low-density lipoprotein (LDL), and HDL data did not reveal any statistically significant differences between the 2 genders of female and male (data are not shown). Also, the ages of the participants in 2 groups of HLP and controls were not statistically different. Although the amounts of TG, Chol, and LDL were higher, HDL was lower in HLP group compared with the controls (Table 1).
Lipid Components in High Lipid Profile and Control Groups

Results are presented as mean ± standard deviation.
The independent sample t-test was performed to compare the 2 groups.
Chol, cholesterol; F/M, female/male; HDL, high density lipoprotein; HLP, high lipid profile; LDL, low-density lipoprotein; No., number; TG, triglyceride.
The mean serum level of IL-17 in the HLP group was 3.43 ± 0.5 pg/mL and in controls was 2.28 ± 0.3 pg/mL. The results of the independent samples t-test showed that the level of IL-17 was statistically higher in the HLP group compared with its level in the controls (P < 0.001). The serum levels of CEA (HLP = 1.17 ± 0.4 versus controls = 1.05 ± 0.3 ng/mL, P = 0.526) and PSA (HLP = 4.44 ± 0.9 versus controls = 3.57 ± 0.8 ng/mL, P = 0.373) were not significantly different between the 2 groups (Fig. 1).
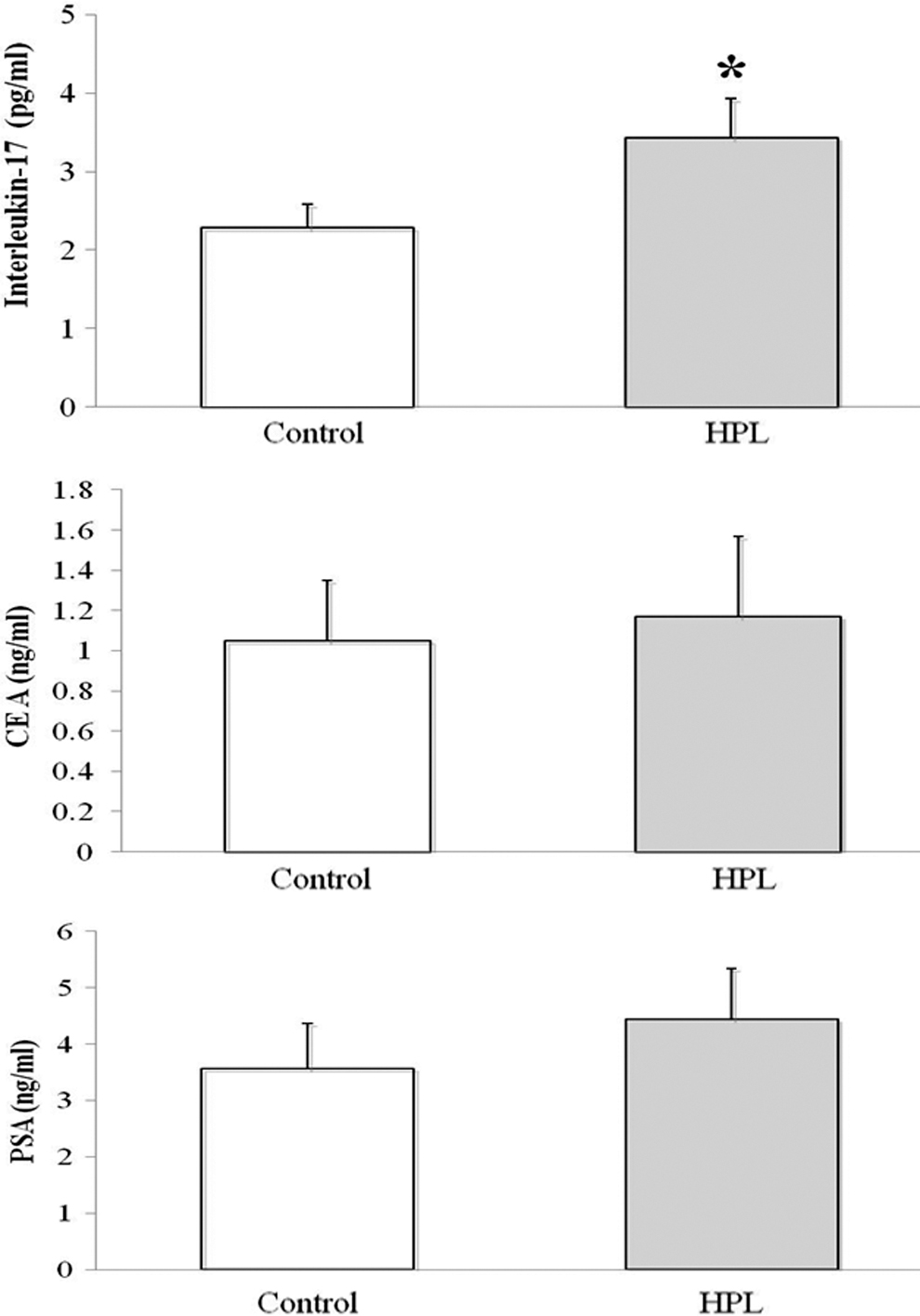
Serum levels of IL-17, CEA, and PSA in HLP and control groups. The independent samples t-test was performed to compare the 2 groups. The PSA levels were only detected in male cases. *P < 0.001. CEA, carcinoembryonic antigen; HLP, high lipid profile; IL-17, interleukin-17; PSA, prostate-specific antigen.
Owing to an increase in serum IL-17 level in HLP group, curve estimation model between IL-17 and HLP components were illustrated. Figure 2 shows a positive correlation between increase of TG, Chol, and LDL in serum with IL-17 concentration. In contrast, this correlation for IL-17 and HDL was negative.
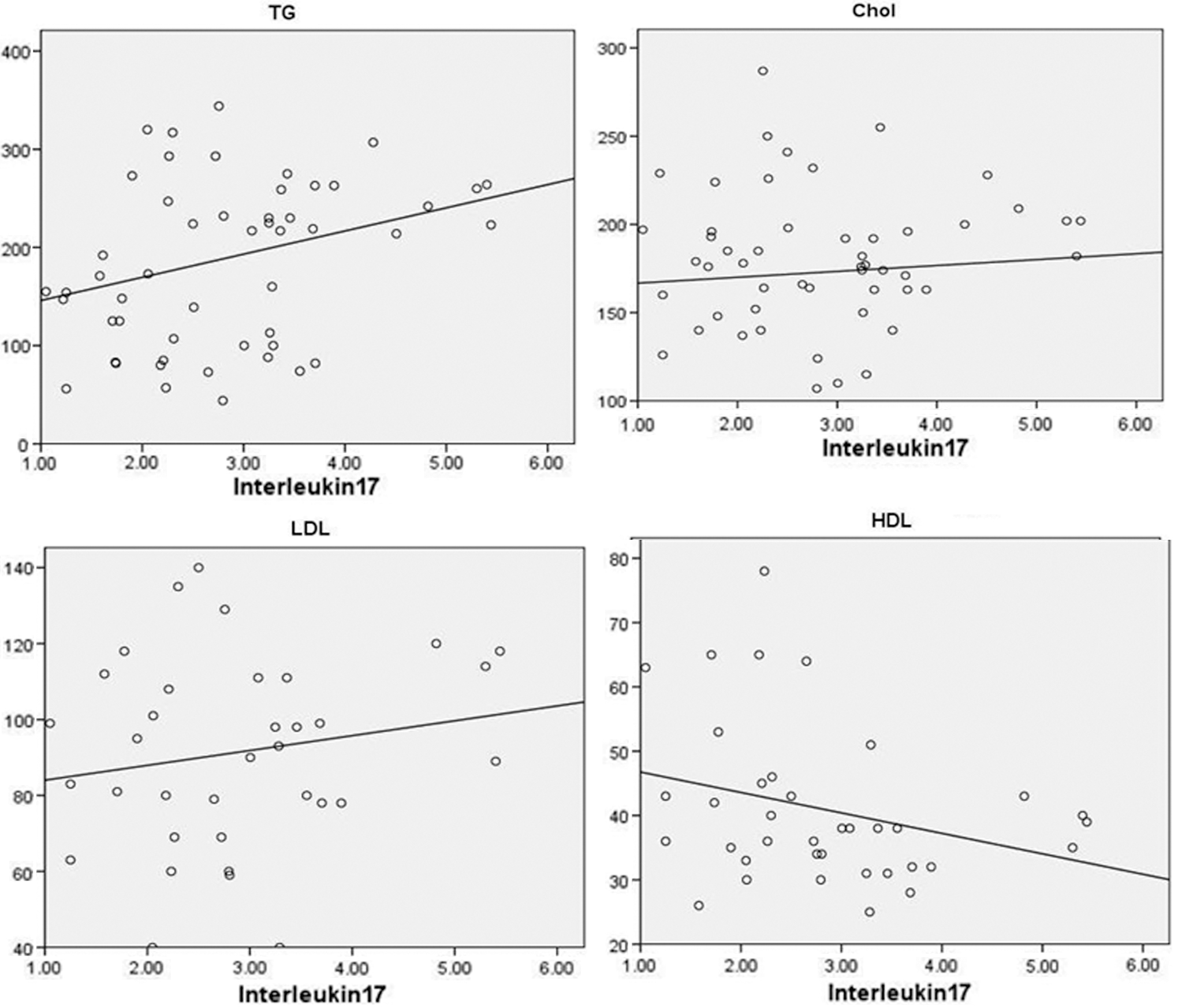
Curve estimation between IL-17 and HLP components. Curve estimation test was performed between IL-17 and TG, Chol, LDL, and HDL data. The results showed a positive linear correlation between IL-17 and TG, Chol, and LDL levels. However, correlation between IL-17 and HDL was negative. Chol, cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglyceride.
Pearson correlation test was performed between IL-17, CEA, and PSA with TG, Chol, LDL, and HDL data. The results of the correlation analysis showed a positive linear association between the TG, Chol, and LDL and IL-17 levels. Correlation between HDL and IL-17 was a negative linear association. The correlation between TG and IL-17 was only supported by statistical test. The results of correlation test for CEA and PSA were not statistically significant (Table 2).
Correlation Between Interleukin-17, Carcinoembryonic Antigen, and Prostate-Specific Antigen with High Lipid Profile Components
Pearson correlation test was performed between IL-17, CEA, PSA, TG, Chol, LDL, and HDL data. The results showed a positive linear correlation between IL-17 and CEA with TG and HDL, respectively.
Statistically significant.
CEA, carcinoembryonic antigen; IL-17, interleukin-17; PSA, prostate-specific antigen.
In addition, the results of linear regression analysis test revealed a positive correlation between HLP and IL-17 (R = 0.633, P = 0.005).
Discussion
This study measured the serum levels of IL-17, CEA, and PSA in 2 groups of HLP and normal lipid profile controls. The associations of lipid components with serum IL-17 were also evaluated. The results showed that the level of IL-17 was higher in HLP group compared with the controls. There was also a positive statistically significant association between serum levels of TG and IL-17.
According to the literature, there is no direct study about the association of serum HLP and IL-17 in normal cases. The most studies are about the relationship between obesity/metabolic syndrome and IL-17 (Surendar and others 2011; Owczarczyk-Saczonek and Placek 2017; Perez and others 2019). In metabolic syndrome there is a cluster of disorders such as hypertension, high blood sugar, excess body fat, and abnormal lipid levels that occur together. It is obvious that each of these conditions may individually affect the production of IL-17 or other proinflammatory cytokines. In an experimental murine model by obesity-induced metabolic syndrome, the data have demonstrated that the mice lacking for IL-17 receptor were protected against obesity (Perez and others 2019). Another experiment dealing with the use of an anti-IL-17 monoclonal antibody to inhibit IL-17 function in nonalcoholic fatty liver disease (NAFLD) revealed significant improvement in the liver function, attenuated hepatic lipid accumulation, and decreased proinflammatory cytokines levels that are associated with NF-κβ signaling pathway (Xu and others 2013).
Furthermore, it has been reported that the metabolism of hepatic lipids, TG, and production of IL-17 in the liver is associated with microRNA 26a (Mir-26a). In an in vivo and in vitro study by He and others, they found lower expression of IL-17 in the nonalcoholic fatty liver tissue induced by Mir-26a expression. In addition, total liver weight, infiltration of immune cells, and hepatic TG deposition were also decreased by expression of Mir-26a (He and others 2017). In association between TG and IL-17, it was reported that TG-rich lipoproteins and IL-17 cause to activation of NF-κβ, vascular cell adhesion molecule-1 and other inflammatory mediators (Welty 2013; Yu and others 2014). NF-κβ is a key regulatory transcription factor in the inflammatory response of the immune system (Goldminz and others 2013). A study by Cimato and others (2013) has also shown a positive correlation between LDL Chol and serum IL-17 level. In an in vitro experiment, the human peripheral mononuclear cells were exposed to mycobacterial surface lipids and produced a large amount of IL-17 (Jonsson and others 2012).
In contrast, there are some contrast results about the effect of IL-17 on obesity/metabolic syndrome and contributes to the development of atherosclerosis by induction of inflammation. IL-17 inhibits interferon-γ and some adhesion molecules on the cells and may protect atherogenesis and decreased adipose tissue accumulation (Owczarczyk-Saczonek and Placek 2017). Another epidemiological study refers to a reduction in serum IL-17 level in metabolic syndrome compared with controls (Surendar and others 2011).
In this study, although CEA concentration in HLP group showed a little higher than its level in the controls, this variation is not statistically significant. It seems that the change in level of CEA could be statistically significant provided that the sample size increased. There is also some controversial report about the association between CEA and HLP. Esteghamati and others (2014) study reported higher levels of TG in combination with other components of metabolic syndrome were directly associated with CEA levels. It could be mentioned that Esteghamati and others determined CEA levels in metabolic syndrome patients who had a conglomeration of many metabolic disorders, but our cases were only healthy volunteers with HLP. Another study showed a positive correlation between CEA and TG level in female Korean nonsmokers (Lee and others 2012). A study on 200 healthy Korean nonsmokers reported a direct association between CEA and NAFLD and its grade of hepatic steatosis. They explained that CEA might enroll in the pathophysiology of fatty liver disease (Lee and others 2013). In contrast, a study on 1,915 healthy Chinese males revealed a significantly reverse linear correlation of CEA concentration with BMI. Although they mentioned the effect of larger plasma, volume might be a critical factor in this reduction (Li and others 2014).
There was also no statistical difference between the serum level of PSA in HLP and controls. Although similar to the CEA level, PSA level was also a little higher in the HLP cases. Similar to our results, Han and others (2008) reported no correlation between TG and Chol with PSA. However, they found a negative correlation between HDL and PSA. An investigation evaluated the association between serum lipid profile with a serum PSA level in healthy men. They found a negative correlation between BMI and TG levels with serum PSA level. However, there was no correlation between serum Chol and HDL (Liu and others 2011).
According to the results of this study, it can be concluded that the serum IL-17 concentration in the HLP individuals is higher compared with normal lipid profile. This abnormal condition may cause to increase the systemic chronic inflammation and other inflammatory diseases.
Footnotes
Acknowledgments
The authors express their gratitude to the staff of the Arad Clinical Diagnostic Laboratory (Hamadan, Iran) for their supportive assistance.
Compliance with Ethical Standards
All the protocols of the study were approved by the Committee of Ethics for Hamadan University of Medical Sciences, Hamadan, Iran (Code:
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was funded (no. 9404091983) by vice-chancellor for research and technology, Hamadan University of Medical Sciences.