
Abstract
Evidence suggests that interleukin-6 (IL-6) concentrations have an important role in suicide behavior (SB) as they are usually increased in these individuals, although no conclusive outcomes have been attained. The purpose of this study was to evaluate the IL-6 levels in plasma, serum, and cerebral spinal fluid (CSF) to determine through a meta-analysis if these levels are increased in individuals with SB in comparison to a group. We calculated the standardized mean difference and 95% confidence intervals (95% CIs). In the systematic review, 21 studies were included, while in the meta-analysis, we included nine studies. The results of our meta-analysis indicated that individuals with SB had reduced levels of IL-6 in plasma (d − 0.189, 95% CI: −0.274 to −0.103, Z, P (Q) = 0.339, I 2 = 7.478), but increased levels of IL-6 in serum (d − 1.14, 95% CI: 0.658 to 1.630, Z, P (Q) = 0.26, I 2 = 7.47) and CSF (d 0.64, 95% CI: 0.245 to 1.035, Z, P (Q) = 0.163, I 2 = 44.80). The meta-regression analysis showed an association between males and high IL-6 levels in plasma (P = 0.003) and serum (P = 0.010), but not the central nervous system (CNS), while age was not associated with IL-6 levels in any of the samples evaluated (plasma, serum, or CNS). The present meta-analysis indicates that serum and CNS IL-6 levels are increased in individuals with SB, while plasma IL-6 levels are decreased, highlighting the importance of the biological sample at the moment of selecting IL-6 as biomarker. However, we need more studies performed in different populations that measure IL-6 and also consider gender when these measures are performed.
Introduction
Suicide has become a serious global public health issue. Hence, different research approaches have emerged to better understand suicide behavior (SB) with the purpose to improve suicide prevention strategies worldwide (Fazel and Runeson 2020). An important step in developing more effective prevention and intervention programs is identifying robust indicators of risk, including biomarkers (Zhou and others 2020).
SB is a complex issue involving a number of psychological, social, cultural, and biological factors (Miller and Black 2020). One mechanism of interest linked with suicide is inflammation (Brundin and others 2017). In this sense, evidence supports that proinflammatory cytokines are a key factor in mediating behavior, neuroendocrine, and neurochemical features of psychiatric disorders (Suzuki and others 2019). Nonetheless, it is not clear whether inflammation is directly involved in the pathophysiology of suicidal behavior, or it arises as a secondary manifestation of these behaviors (Bergmans and others 2019). In addition, it is unknown if suicidal behavior represents a maladaptive version of the innate immune response activation, exacerbating the intensity and/or duration of the immune response or if it increases the vulnerability to suicide (Cáceda and others 2018). However, from the cascade inflammation, one of the most often implicated cytokines in suicide association studies are the interleukins (Keaton and others 2019).
To examine if the interleukins dysregulation is associated with suicide, several investigations have assessed interleukins levels in suicidal adult individuals (Kim and others 2014). The interleukin-6 (IL-6) is one of the interleukins most often implicated in association studies (Isung and others 2014). Some association studies have reported that levels of IL-6 were significantly higher in suicide individuals compared with nonsuicidal individuals (Conejero and others 2019). These studies suggest that IL-6 levels are abnormally high in suicidal individuals. Nevertheless, the IL-6 levels in individuals with SB are inconsistent; therefore, our aim was to measure whether the IL-6 levels differ between individuals with suicidal behavior and comparison groups through a meta-analysis and systematic review.
Methods
The present meta-analysis based on published studies was performed following the PRISMA statement. This study did not need the informed consent of patients nor ethical approval. The present work did not required IRB approval or waiver statment. All data is available on request to the correspondence author.
Search strategy
We systematically conducted a literature search using PubMed, Scopus, and Web of Science electronic databases. The relevant keywords used to identify publications of IL-6 levels and SB were “interleukin 6 AND suicide,” “IL-6 AND suicide,” “interleukin 6 AND suicidal behavior,” and “IL-6 AND suicidal behavior.” The reference lists of eligible studies were screened manually for any missing studies. In addition, all the eligible studies were checked carefully to prevent overlapping datasets.
Inclusion and exclusion criteria
The studies included in this meta-analysis had to meet the following inclusion criteria: (1) assessed the possible association between IL-6 levels and SB, (2) conducted under a case-control design, (3) had clearly reported the interleukin concentrations in both groups, (4) published in peer-reviewed indexed Journals or in Journal Citation Reports, and (5) data collection and analyses performed had to be valid from a statistical point of view.
The exclusion criteria for selection were as follows: (1) duplicates, (2) functional studies involving in vivo/in vitro analysis, (3) reviews, comments, or animal studies, and (4) reports in languages other than English.
Data extraction
Data were independently extracted by two investigators (González-Castro and López-Narvaez), contradictions between them were discussed until reaching agreement. The information obtained from each article consisted of first author's name, publication year, country, sample size, type of SB, criteria of diagnosis, interleukin levels, biological sample, mean age, gender, and main outcomes.
Literature quality evaluation
The eligible articles were carefully read and evaluated according to the Newcastle-Ottawa Scale (NOS). This scale evaluates each study based on three broad categories: selection of the study groups, the comparability of the groups, and the ascertainment of the outcome of interest. All the studies with less than six stars were considered low quality, only articles with at least six stars or more were included in this analysis. The same investigators (Gonzalez-Castro and López-Narvaez) worked independently in the quality assessment then cross-checked their findings; if consensus could not be reached a third investigator (C.A.T.-Z.) was involved.
Statistical analysis
We grouped studies according to the origin of the sample: (1) serum levels of IL-6 (In 2012, Karlović and others evaluated first a group of individuals with SB and with major depression disorder (MDD) and atypical features, and a second group of individuals with SB and with MDD and melancholic features), (2) plasma levels of IL-6 (In 2013, O'Donovan and others evaluated individuals with lower and higher suicide ideation, while Dolsen and others 2020 evaluated suicide attempters and suicide ideators), and (3) cerebral spinal fluid (CSF) IL-6 levels (Lindqvist and others 2009 compared IL-6 concentrations between violent suicide attempters and nonviolent suicide attempters). The units of measurement that were different among studies were transformed into unified units.
For estimate, the differences of IL-6 levels in serum, plasma, and cerebral spinal levels between individual with SB and controls by meta-analysis, we calculated the standardized mean differences (d) and 95% confidence intervals (95% CIs) of the three analyses. Furthermore, the effect size was converted to odds ratio and 95% CIs to get a better understanding of the implication of IL-6 levels in SB. The evaluation of heterogeneity of interstudy variations was performed with Q-test. In addition, I 2 was used as an indicator of heterogeneity to measure the level of inconsistency across studies. If there was significant heterogeneity (P-value Q test <0.05, I 2 > 50%), the random-effect model (by Dersimonian-Laird method) was used to pool the effect sizes; otherwise, the fixed effect model (by Mantel-Haenszel method) was applied. To assess the effect of each primary study on the total mean difference, a sensitivity analysis was conducted. In addition, suspected factors of heterogeneity were investigated using meta-regression models based on the mean age and the proportion of males. Funnel plots were constructed and Egger's test regression was used to establish possible publication bias. All tests were two-sided, with a significance threshold of P-value <0.05. The meta-analysis was conducted using the Comprehensive Meta-analysis software (CMA version 2 Biostat, Inc., Englewood). Meta-regression analyses were also performed with CMA v.2
Results
Study information
The search strategy retrieved 21 potential case-control studies from 2008 to 2020 (Fig. 1). From these, 17 studies were performed in Caucasian descendants; one study was performed in Asian individuals, one study in Middle-East individuals, and two studies evaluated Latin American subjects. The principal biological sample used to measure interleukins levels in cases and controls was plasma, followed by serum and finally CSF. With regard to the suicidal behaviors, 11 studies focused in suicide attempts, 1 article in suicide ideation, 5 articles used samples from individuals who died by suicide, and 4 reports used a combination of suicidal spectrum. More characteristics are shown in Table 1.
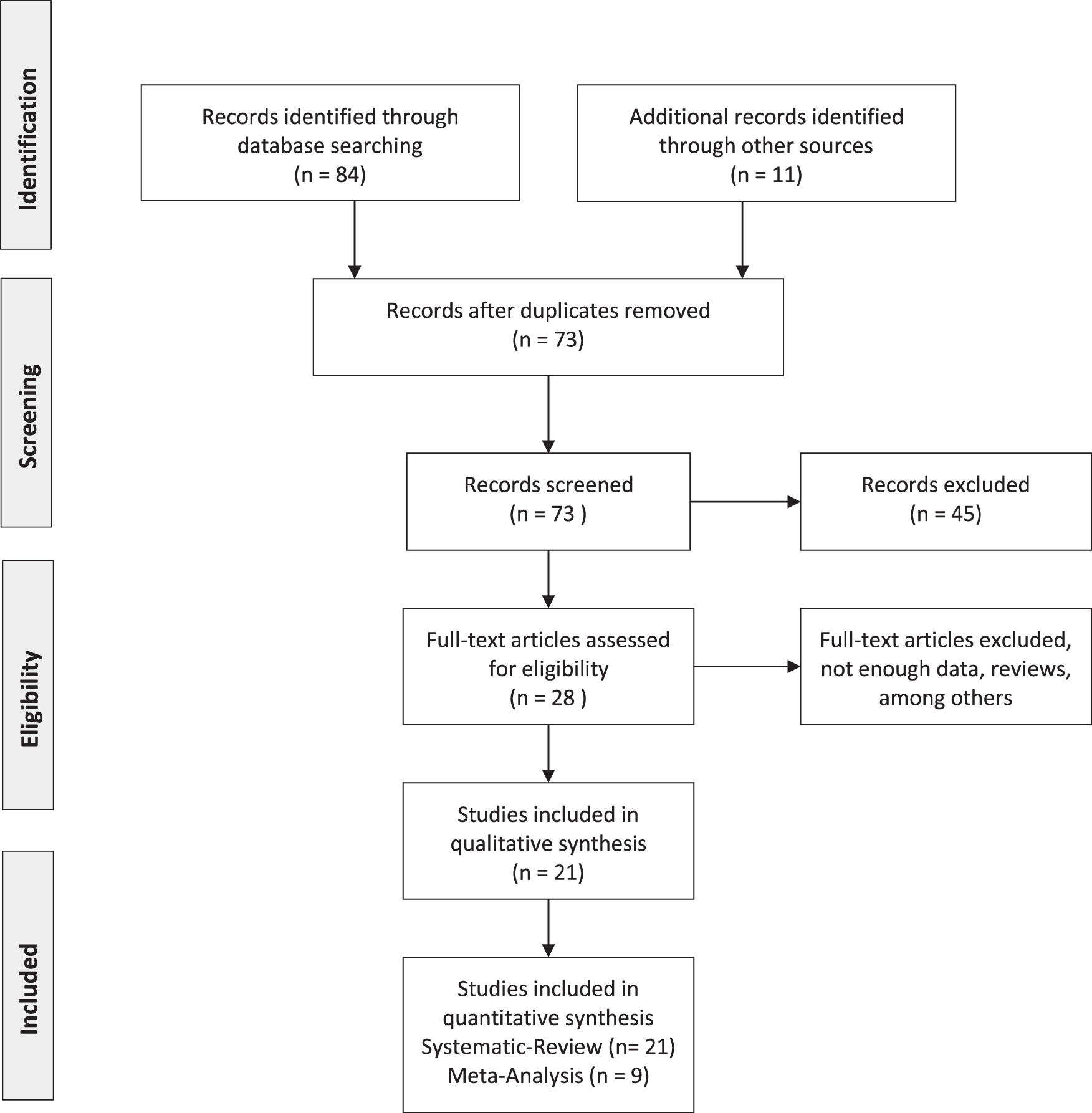
Flowchart of the literature search and studies selection.
General Characteristics of the Case-Control Association Studies with Suicidal Behavior Included in the Systematic Review
ANX, anxiety; BD, bipolar disorder; BDI, Beck Depression Inventory; BSS, Beck Scale for Suicidal Ideation; CGAS, Children's Global Assessment Scale; CIDI, Composite International Diagnostic Interview; CSF, cerebral spinal fluid; C-SSRS, Columbia Suicide Severity Rating Scale; DSM-IV, Diagnostic and Statistical Manual of Mental Disorder edition IV; ECL, high-sensitivity electrochemiluminescence; ELISA, enzyme-linked immunosorbent assay; HARS, Hamilton's Rating Scale for Anxiety; HDRS, Hamilton's Depression Rating Scale; K-SADS-PL, Schedule for Affective Disorders and Schizophrenia–Present and Lifetime Version for Children; MADRS, Montgomery-Asberg Depression Rating Scale; MDD, major depression disorder; MINI, Mini International Neuropsychiatric Interview; NA, not available; PCR, polymerase chain reaction; PTSD, post-traumatic stress disorder; SA, suicide attempters; SB, suicide behavior; SCHZ, schizophrenia; SI, suicide ideators; SUAS, Suicide Assessment Scale; SUD, substance use disorder; SV, suicide victims.
Based on the inclusion and exclusion criteria as well as the NOS scale measurement in this meta-analysis, we only analyzed nine studies, which clearly stated the IL-6 levels for cases and controls. Subsequently, we analyzed the IL-6 levels in 878 cases and 4,274 controls. The average age of the sample analyzed was 38.66 years for cases and 34.93 years for controls. The mean body mass index was 25.69 kg/m2 for cases and 24.64 kg/m2 for controls.
Meta-analysis of IL-6 levels in plasma samples
In this meta-analysis, we included five case-control association articles of IL-6 and SB (Kim and others 2008; Gabbay and others 2009; O'Donovan and others 2013; Eidan and others 2019; and Dolsen and others 2020) (Table 2). In a first view with the presence of heterogeneity, we found that individuals with SB did not show statistical differences of IL-6 concentrations in comparison with the comparison group (d: 0.204, 95% CI: −0.084 to 0.492, Z P-value 0.164, Q P-value <0.0001, I 2 = 87.83, Z P-value = 0.165). However, when the studies that gave heterogeneity were discarded (Q P-value 0.339, I 2 = 7.478), we observed that individuals with SB presented reduced levels of IL-6 in comparison with the control group (d: −0.189, 95% CI: −0.274 to −0.103, Z P-value <0.0001). Eggers test was performed to assess potential publication bias; no statistical significance was found; Table 3. Furthermore, we convert d in odds ratio. We found the reduced levels of IL-6 in the SB group remain [odds ratio (OR) 0.710, 95% CI: 0.609 to 0.829, Z P-value <0.0001] (Fig. 2).
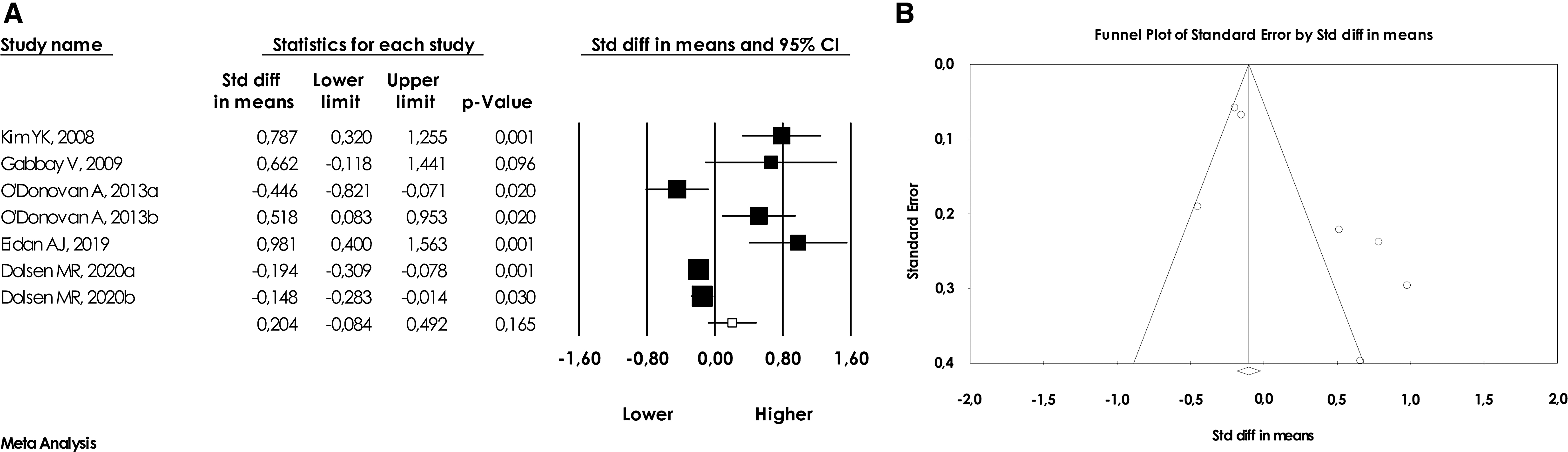
Meta-analysis of the association of IL-6 plasma levels and suicidal behavior describing
Description of Interleukin-6 Levels and Sample Features of Suicide Behavior Association Studies Included in the Meta-Analysis
Mean, standard deviation.
Mean, standard error.
BMI, body mass index; HC, healthy controls; IL-6, interleukin-6; MDD-AS, major depressive disorder with atypical features with suicidal behavior; MDD-MS, major depressive disorder with melancholic features with suicidal behavior; WSB, without suicidal behavior.
Meta-Analysis of the Case-Control Association Studies Between Interleukin-6 Levels and Suicidal Behavior with Standardized Mean Differences Effect Size
N, number of studies included; d, standardized mean differences.
95% CI, 95% confidence interval; SE, standard error.
Meta-analysis of IL-6 levels in serum samples
Second, when we evaluated IL-6 in serum (Karlović and others 2012; Vargas and others 2013), we found statistical differences between cases and controls. We observed increased levels of IL-6 in serum of individuals with SB (d: 1.144, 95% CI: 0.658 to 1.630, Z P-value <0.0001) in the absence of heterogeneity (Q P-value 0.269 and I 2 = 23.76). No significant evidence of publication bias was found (P-Value 0.431). In addition, we evaluated IL-6 serum based on odds ratio effect size. As the same of the other analysis, a statistical relationship (OR 7.963, 95% CI: 3.296 to 19.243, Z P-value <0.0001) was founded after discarding heterogeneity (Fig. 3).
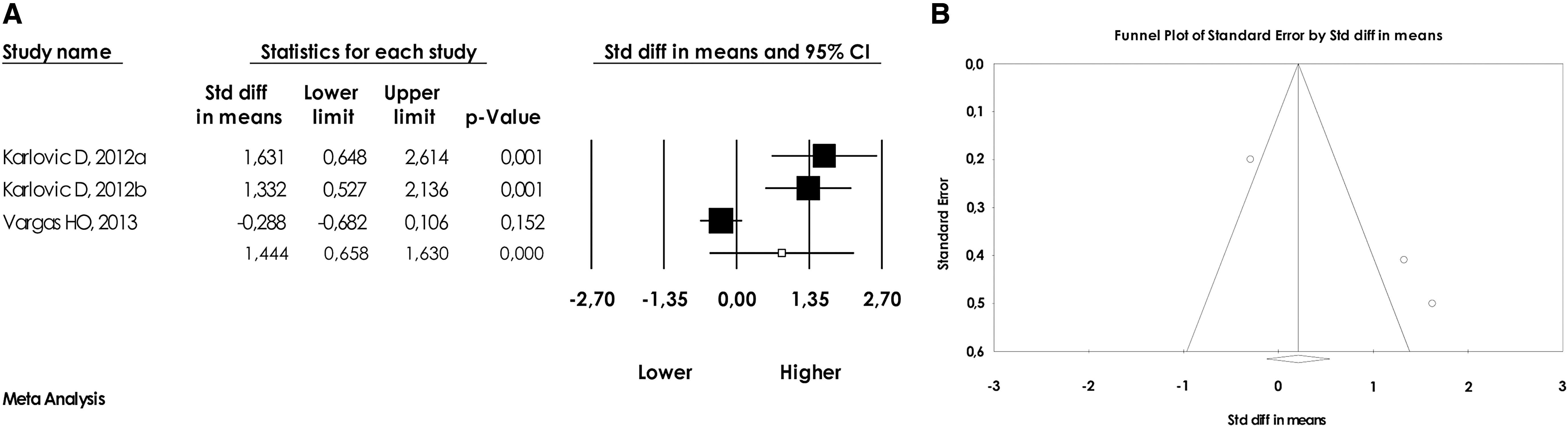
Meta-analysis of the association of IL-6 serum levels and suicidal behavior describing
Meta-analysis of IL-6 levels in CSF samples
This last analysis revealed increased levels of IL-6 in CSF of individuals with SB (Q P-value 0.163, I 2 = 44.80; d: 0.640, 95% CI: 0.245 to 1.035, Z P-value 0.002) (Lindqvist and others 2009; Isung and others 2012). Our results suggest that the IL-6 levels are increased in CSF of individuals with SB when compared with the control group. The forest plot is shown in Fig. 2B. Publication bias was measured according to Egger test, no significant P-value was reported (P-value 0.946). Moreover, with ORs effect size analysis, we observed an association (OR 3.182, lower limit 1.891, upper limit 5.358, Z P-value <0.0001) with suicidal behavior and CSF levels (Fig. 4).
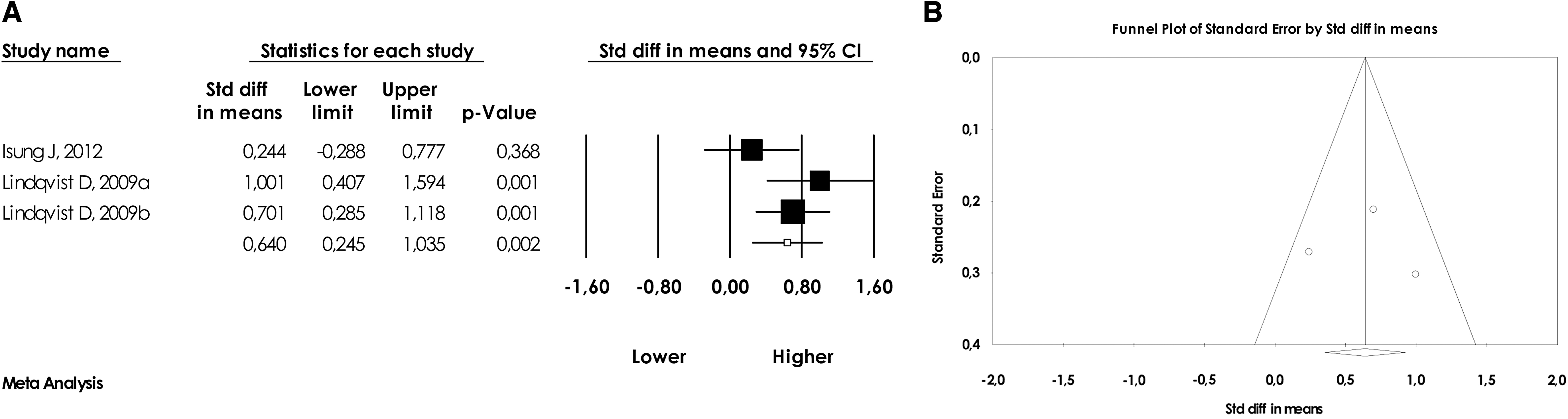
Meta-analysis of the association of IL-6 CSF levels and suicidal behavior describing
Sensitivity analysis
To assess the stability of our results, we performed a sensitivity analysis by sequentially excluding individual studies for each meta-analysis. For the association between plasma, serum, and CSF IL-6 levels and SB, no single study qualitatively changed the pooled D’ when removed, indicating that the results of this meta-analysis are stable.
Meta-regression models
We also performed meta-regressions to identify factors influencing the mean rates of plasma, serum, and CSF analyses. Specifically, we based these analyses on the mean age and proportion of males associating IL-6 levels and suicidal behavior.
The meta-regression analyses based on mean age revealed no statistical relationship of IL-6 levels in plasma (point estimate 1.116; Lower limit −0.071; Upper limit 2.304; P-value 0.065), serum (Serum point estimate 0.888; Lower limit −0.293; Upper limit 2.069; P-value 0.140), or CSF (point estimate −22.46; Lower limit −2.366; Upper limit 47.304; P-value 0.076).
The meta-regression based on the proportion of males suggested a statistical association of IL-6 levels in plasma (point estimate −0.745; Lower limit −1.244; Upper limit −2.926; P-value 0.003) and serum (point estimate −0.628; Lower limit −1.112; Upper limit −0.144; P-value 0.010), while IL-6 levels in CSF (CSF point estimate −0.805; Lower limit −2.471; Upper limit 0.861; P-value 0.343) showed no association.
Discussion
The aim of this systematic review and meta-analysis was to investigate if IL-6 levels in plasma, serum, and CSF are increased in individuals with SB in comparison with a control group. The effect of a particular cytokine on a given cell depends on the cytokine, its extra cellular abundance, the presence (or absence) of the complementary receptor on the cell surface, and downstream signals activated by receptor binding (Rincon 2012; Pandey and others 2018a, 2018b). Specifically, there are two signaling pathways to IL-6: the anti-inflammatory pathway also known as the classical way and the proinflammatory pathway also known as the trans-signaling way (Su and others 2017). In the proinflammatory pathway, IL-6 attaches to a soluble IL-6R (not membrane-bound) and it is used by various cell types within the brain (Rincon 2012; Rossi and others 2015; Ohlsson and others 2019). Therefore, this pathway is very often selected as a candidate to study several diseases (Rincon 2012; Bay-Richter and others 2015; Schiavone and others 2016; Nowak and others 2019) such as the psychiatric diseases (Rincon 2012; Rossi and others 2015; Eidan and others 2019; Coryell and others 2020; Dolsen and others 2020).
Our meta-analysis revealed that IL-6 levels in plasma are decreased in individuals with suicidal behavior, while in serum and CSF individuals with SB, the IL-6 levels are increased. These findings have clinical importance evidencing the role of interleukin levels in SB and the possible use of IL-6 levels as a biomarker of SB.
Our first analyses revealed lower IL-6 plasma levels in individual with suicidal behavior, which is in agreement with previous works. For example, in a group of 36 individuals with MDD who had recently attempted suicide and 33 nonsuicidal MDD individuals, the IL-6 plasma levels were significantly lower in the suicidal group when compared with the nonsuicidal group (Kim and others 2008). To explain this lower IL-6 plasma levels, we hypothesized that IL-6 is directly involved in developing SB. For example, in a group of 12 individuals with depression in a remission state, normal IL-6 levels were observed, indicating that already in remission state these individuals had similar IL-6 levels to healthy controls (Frommberger and others 1997). In this subanalysis, the majority of articles showed a considerable interval of time between the suicidal attempt and the evaluation of IL-6 in each individual (Kim and others 2008; Dolsen and others 2020). This implicates that it is necessary to take into consideration the time of SB and sampling, as well as if the individual is in pharmacological treatment or not.
With regard to IL-6 serum concentrations, we observed higher levels of IL-6 in individuals with suicidal behavior; however, there are mixed outcomes. For example, Karlović and others, did not observe statistical differences in IL-6 serum levels in suicidal and nonsuicidal subjects with MDD (Karlović and others 2012); nevertheless, they found a positive correlation between the severity of depression in melancholic subjects. Furthermore, in 4,500 individuals from a cohort, higher levels of the systemic inflammatory marker IL-6 in childhood were associated with an increased risk of developing depression and psychosis in young adulthood (Khandaker and others 2014), highlighting the possibility that IL-6 serum concentration is a suitable biomarker of psychiatric diseases. Concerning the discrepancies we observed between plasma and serum IL-6 levels, this has been observed before in a meta-analysis that compared IL-6 in plasma and serum between individuals (children and adults) with obstructive sleep apnea syndrome (OSAS) and healthy controls, in which the pooled analysis of serum and plasma IL-6 levels in children with OSAS compared with controls revealed that only the MD of plasma IL-6 levels was significant (Imani and others 2020).
Finally, regarding the IL-6 CSF levels in suicidal individuals, we found a relationship between increased levels of IL-6 and SB. This is in agreement with previous studies as Lindqvist and others (2009) reported that IL-6 in CSF was significantly higher in suicide attempters than in healthy controls. In addition, they observed that individuals who performed violent suicide attempts displayed higher IL-6 levels than other suicide attempters (Lindqvist and others 2009). In a different meta-analysis, it was observed that IL-6 concentrations in CSF were increased in individuals with schizophrenia, but not significantly increased in affective disorders when compared with healthy controls (Orlovska-Waast and others 2019), which indicates that IL-6 CSF levels differ depending on the psychiatric diagnostic (Coccaro and others 2015).
Our findings clearly correlate IL-6 levels suicidal behavior; nevertheless, we should take notice of circumstances that could affect directly or indirectly the interleukins levels. For instance, the research of suicide biomarkers, including IL-6, should take into consideration the physical and psychosocial stress that individuals with suicide risk might be having (Tanaka and others 2016). Some evidence indicates that the negative effect of the IL-6 inflammatory role could be derived of an impairment of the regulation process of inflammation (Kiecolt-Glaser and others 2003; Del Giudice and Gangestad 2018). Furthermore, it has been seen that under physiologic conditions, there is a feed forward loop, which is likely to result in IL-6 driven induction of IL-10 release for example, which would, in turn, have the potential to dampen or resolve inflammatory processes through its immunoregulatory/anti-inflammatory effects (Ahmed and Ivashkiv 2000; de Oliveira and others 2018). When this regulation is altered, IL-6 levels modification might contribute to suicidal behavior. Therefore, psychiatric research is important to take into consideration these factors that could play as moderators of IL-6 levels.
It is important to note some limitations in our study. First, we did not evaluate the participation of confounding factors (gender, age, caffeine or alcohol use, exercise, quality of the sleep, and others) that could have affected and challenged the measures of IL-6 levels (Brøndum and others 2016). Another fact is that cytokines are reactive to diverse methodological factors such as storage conditions, repetitive cycles of freezing-thawing among others that could decrease or increase IL-6 levels (de Jonge and others 2003). In addition, we did not evaluate genotypic (polymorphisms) and phenotypic (attempt, ideation or consummation) differences that may have influenced individual reactivity to inflammatory responses in individuals with suicidal behavior (Vargas and others 2013; Grudet and others 2014).
To sum up, our findings indicate that individuals with SB in comparison with a control group have reduced peripheral levels of IL-6 in plasma, but increased in serum; while in CSF, the levels of IL-6 are increased. Based on the present outcomes, the IL-6 levels seem to be a potential biomarker candidate for SB. However, to take a definite conclusion, it is necessary to replicate this type of studies through different populations.
Footnotes
Acknowledgments
We thank everyone who participated in the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.