
Abstract
We describe a rare case of a 58-year-old female with ocular surface squamous neoplasia (OSSN) in her left eye. She was treated for 12 months with topical interferon alpha-2b (IFNα-2b) eye drops and OSSN resolved completely. She presented with a whitish elevated lesion involving the cornea, limbus, and conjunctival surface after discontinuation of topical IFNα-2b. Excision biopsy along with amniotic membrane grafting was done to stabilize the ocular surface. Histopathological evaluation of the excised tissue revealed ocular surface inflammation with no evidence of malignancy.
Case Report
A 58-year-old female presented to us with complaints of a white patch on her left eye for 8 months, demonstrating an increase in whiteness for 2 weeks. She was a known case of hypothyroidism, hypertension, and diabetes mellitus under treatment. On examination, her best-corrected visual acuity (BCVA) was 6/6, N6 in the right eye, and 6/12p, N6 in the left eye. Intraocular pressure was 15 and 12 mmHg in the right and the left eye, respectively. Slit-lamp evaluation revealed a normal anterior segment in the right eye and a large grayish avascular lesion with fimbriated edges on the corneal epithelium involving almost two-thirds of the corneal epithelial surface. A white elevated avascular patch measuring 2 mm × 5 mm adjoining the inferior limbus extending from 6 o'clock to 8 o'clock meridians, suggestive of keratin, was also noted (Fig. 1A). The rest of the ocular examination, including indirect ophthalmoscopy, was within normal limits in both eyes. Anterior segment OCT (AS-OCT) (Topcon Maestro, Japan) of the left eye revealed thickened hyperreflective epithelium with an abrupt transition from normal to an abnormal epithelium (Fig. 1B). There was associated localized shadowing of underlying tissues corresponding to the area with keratin. Based on clinical and AS-OCT findings, she was diagnosed with ocular surface squamous neoplasia (OSSN) involving the left eye (Tis).
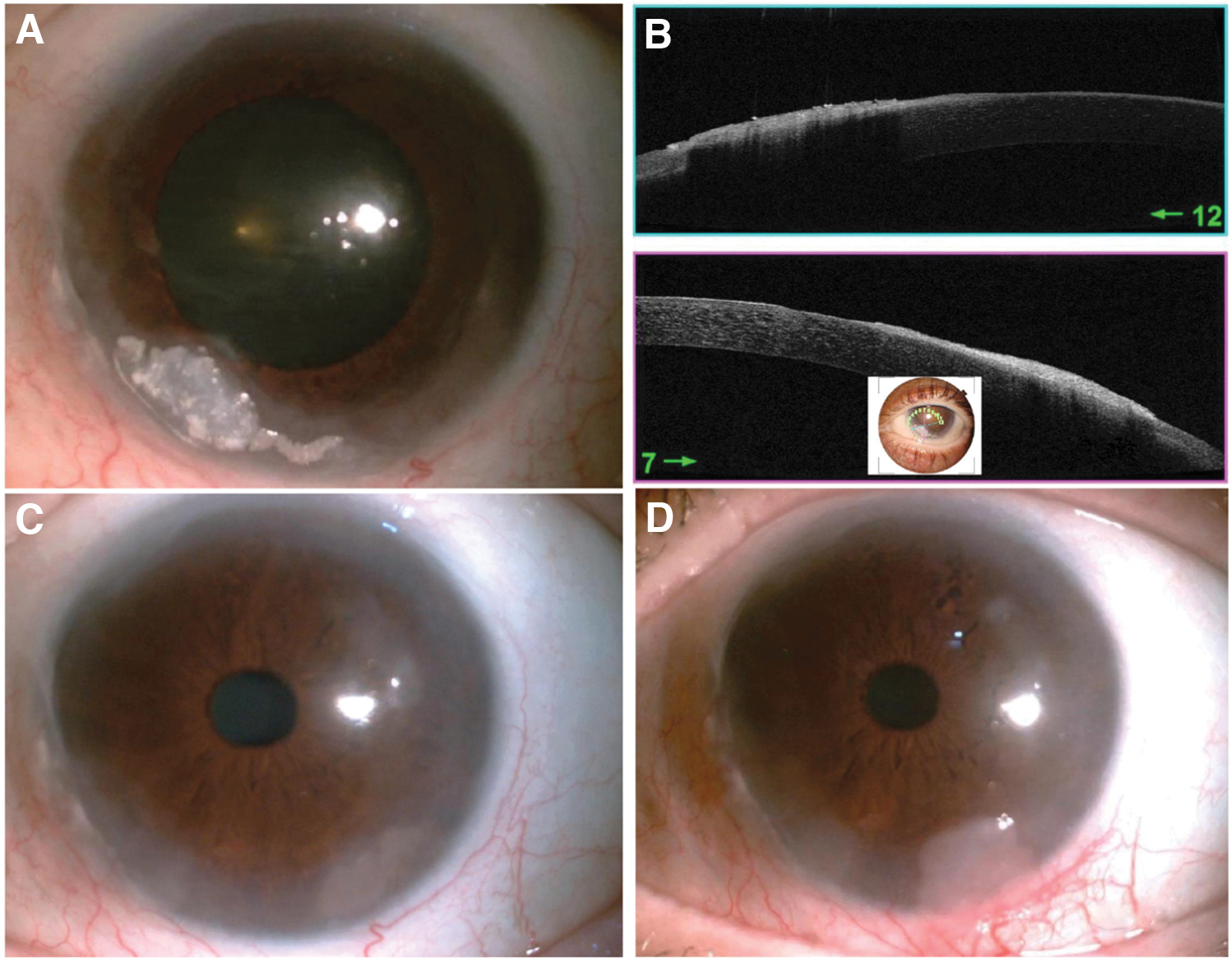
Slit-lamp photograph of the right eye under diffuse illumination on the day of presentation showing grayish epithelial lesion with keratin deposition on the cornea suggestive of OSSN
Treatment was initiated 4 times daily with topical interferon alpha-2b (IFNα-2b) eye drops (1 mIU/mL). One month after initiation of therapy, her BCVA improved to 6/6, N6 in the left eye. The keratin patch appeared to have reduced to size 1.4 mm × 5 mm. Nine weeks after initiation of treatment, minimal keratin remained. The lesion was also noted to be smaller in size. She was reviewed every 2 weeks and the same treatment was continued. Ten months after initiation of therapy, the entire lesion resolved. Treatment was continued for another 8 weeks to avoid recurrence of the lesion and stopped (Fig. 1C).
When reviewed at 10 weeks after cessation of treatment, a whitish elevated patch with superficial vascularization was noted at the 5 o'clock meridian. Eight weeks after this, the patchy lesion was noted to be thickened and increased in size measuring 3 mm × 3.2 mm. It was extending to the adjoining limbus and conjunctiva (Fig. 1D). AS-OCT showed a localized hyper-reflective lesion over a normal-looking epithelium with partial shadowing on the horizontal scan. The same lesion appeared as thickened hyper-reflective epithelium with an abrupt transition from normal to abnormal epithelium on the vertical scan. She was advised to undergo excision biopsy with alcohol epitheliectomy and amniotic membrane grafting.
Under peribulbar anesthesia, a 3 mm clear margin was marked using a marking pen, all around the lesion. The conjunctiva was dissected using the “no-touch” technique. Absolute alcohol was applied on the corneal surface, and the lesion and the adjoining epithelium were excised using a crescent blade. The sample was placed on a filter paper, marked, and sent for histopathological evaluation. Three cycles of cryopexy were done to the conjunctival edge along the excised margin. Amniotic membrane was secured over the bare corneal and conjunctival surface using fibrin glue (Tisseel, Baxter AG, Vienna, Austria). A bandage contact lens was placed. The postoperative period was uneventful.
Histopathological evaluation of the excised tissue revealed hyperplastic epithelium with no evidence of dysplastic/neoplastic cells. Inflammatory infiltrate was noted in the stromal layer of the excised conjunctival tissue (Fig. 2A–C). At the final follow-up, 6 months after surgical excision, the ocular surface was stable with normal looking epithelium (Fig. 2D).
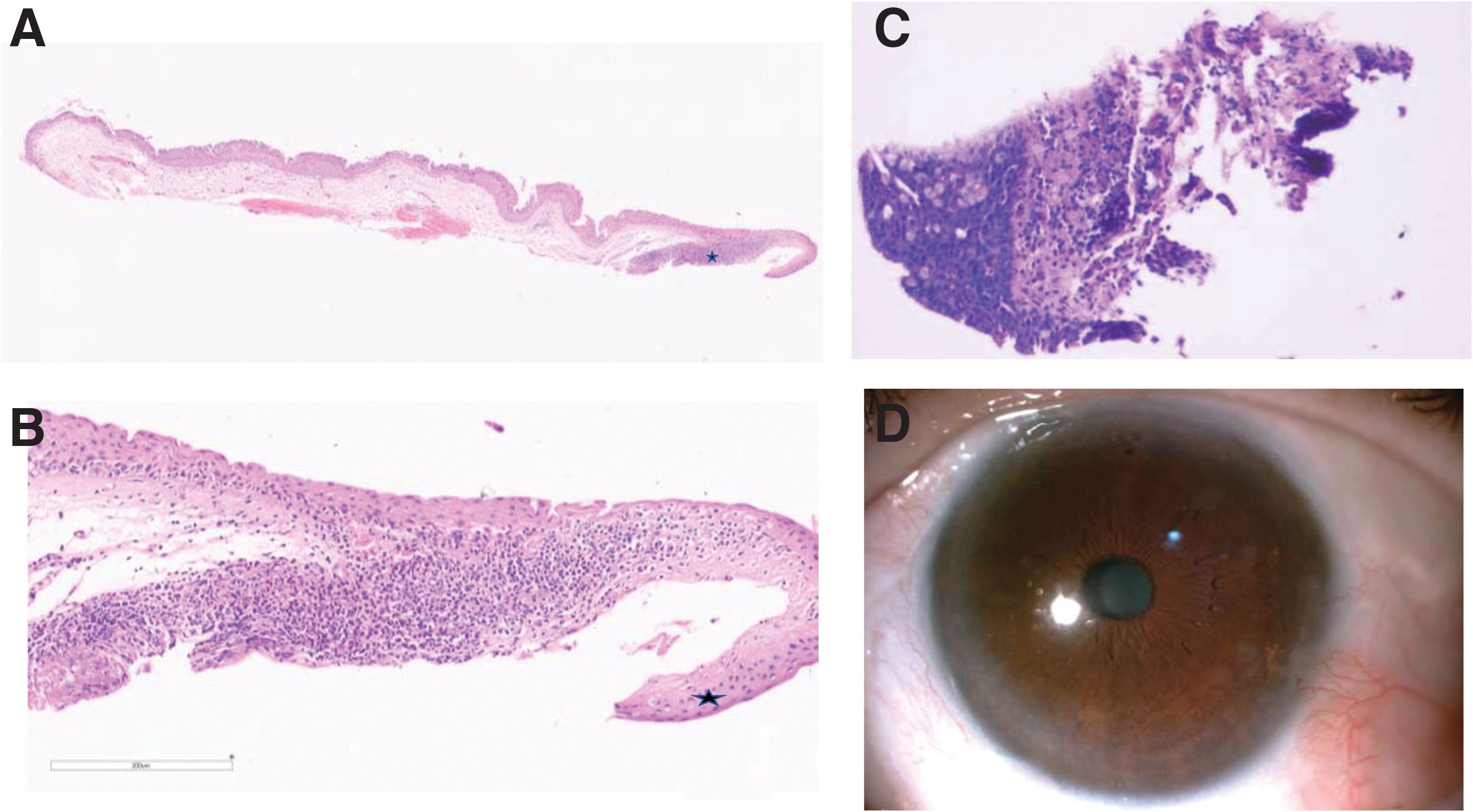
Photomicrograph showing stratified squamous epithelium and stroma with congested blood vessels with a band of lymphoplasmacytic cell infiltrates (black asterisk); hematoxylin and eosin stain, 4.2 × digital scanner magnification
Discussion
The characteristic description of OSSN includes grayish avascular epithelial lesion with fimbriated edges. Classical AS-OCT features diagnostic of OSSN include thickened hyper-reflective epithelium with an abrupt transition from normal to an abnormal epithelium (Singh and others 2018). Presence of keratin and melanin can lead to the shadowing of underlying structures. The lesion our patient first presented with was typical of OSSN both on slit-lamp evaluation and AS-OCT.
However, the lesion noted after the discontinuation of topical IFNα-2b appeared as a whitish elevated lesion with well-demarcated edges that crossed the limbus and involved the adjacent conjunctiva. The AS-OCT scans along the vertical axis were suggestive of OSSN, whereas the scans along the horizontal axis showed a relatively normal-looking epithelium with a thickened hyper-reflective lesion overlying it. Thus, the clinical appearance was not suggestive of OSSN and the AS-OCT was also inconclusive. The patient underwent excision and biopsy to elucidate a histopathological diagnosis.
Interferons are cytokines with antiviral, antineoplastic, and immunomodulatory activity and are currently being used in their recombinant form for various ocular and systemic pathologies (Lewczuk and others 2019; Butler and others 2012) The exact mechanism of action of IFNα-2b in OSSN is not known. It is hypothesized to work by inducing chemotaxis of natural killer cells and cytotoxic T cells into the tumor tissue leading to the destruction of neoplastic cells and resolution of OSSN (Butler and others 2012). Adverse effects after topical IFNα-2b therapy include ocular discomfort, punctate epithelial keratitis, follicular conjunctivitis, and corneal melt (Warren and others 2020).
IFNα-2b has anti-inflammatory, antiangiogenic, and antiproliferative activity and acts against various biological targets including vascular endothelial growth factor, interleukin-8 (IL-8), IL-10, transforming growth factor beta, and tumor necrosis factor alpha (Maleki and others 2018). Our case highlights the possibility of epithelial inflammation leading to hyperplasia after the discontinuation of topical IFNα-2b after prolonged use. We hypothesize this to have occurred due to alterations in the inflammatory pathways by some unknown mechanism leading to rebound inflammation after discontinuation of topical therapy. Excision followed by amniotic membrane grafting helped in restoring a normal ocular surface. Physicians need to be aware of such complications after IFNα-2b therapy.
Footnotes
Authorship Confirmation Statement
ICMJE criteria for authorship followed.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.