
Abstract
Previously, we reported that a malleable protein matrix (MPM), composed of whey fermented by a proprietary Lactobacillus kefiranofaciens strain, has immunomodulatory and anti-inflammatory properties. MPM consumption leads to a considerable reduction in the cytokine and chemokine production (tumor necrosis factor-α, interleukin-1β, and interleukin-6), thus lowering chronic inflammation or metaflammation. Inhibition of metaflammation should provide positive impact, particularly in the context of dyslipidemia, insulin resistance, and hypertension. In this study, we investigated whether short-term MPM supplementation ameliorates those features of metabolic syndrome (MetS). The ability of MPM to potentially regulate triglyceride level, cholesterol level, blood glucose level, and hypertension was evaluated in different animal models. MPM lowers triglyceride level by 37% (P < .05) in a poloxamer 407 dyslipidemia-induced rat model. It also reduces total cholesterol by 18% (P < .05) and low-density lipoprotein-cholesterol level by 32% (P < .05) and raises high-density lipoprotein-cholesterol level by 17% (P < .01) in Syrian Golden hamsters fed a high fat/high cholesterol diet for 2 weeks. MPM reestablishes the fasting glucose insulin ratio index to normal levels (P = .07) in this latter model and lowers the plasma glucose level area under the curve (−10%, P = .09) in fructose-fed rats after 2 weeks of treatment. In spontaneously hypertensive rats, MPM-treated animals showed a reduction of SBP by at least 13% (P < .05) for 4 weeks. Results from this study suggest that MPM is a functional ingredient with beneficial effects on lipid metabolism, blood glucose control, and hypertension that might contribute to the management of MetS and thus reducing the risk of cardiovascular diseases.
Introduction
N
MetS is a group of metabolic disorders that are often found together in individuals at higher risk of CHD and T2DM. The set of criteria provided in the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) are widely used to diagnose people having MetS. Criteria considered in the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III are abdominal obesity, elevated triglycerides (TG), and low high-density lipoprotein cholesterol (HDL-C), elevated fasting plasma glucose, and elevated blood pressure. Three or more of these criteria are needed for MetS diagnosis. 3 Elevated levels of TG and low levels of HDL-C, as part of the atherogenic dyslipidemia, are highly associated in overweight/obese and/or T2DM individuals and apparently contribute the whole CHD risk, besides low-density lipoprotein cholesterol (LDL-C) alone. Elevated blood pressure is included in the MetS diagnosis because of its direct correlation with obesity and incidence in diabetic patients as well as its implication in atherosclerotic diseases. 4,5 Impaired fasting glucose, as an indicator of insulin resistance, is the root cause leading to the development of T2DM in people having MetS. 3 MetS is also characterized by prothrombic and pro-inflammatory states. It is argued that all those risk factors are closely linked and that the probable key features at the basis of MetS are being overweight and obesity.
Obesity can lead to a chronic inflammatory state within adipose tissue depots, which can cause adipocyte dysfunctions. 6 Metaflammation (chronic or low-grade inflammation) is characterized by abnormal cytokine production, increased acute-phase reactants and other mediators, and activation of a network of inflammatory signaling pathways. 7 Experimental, epidemiological, and clinical evidence links inflammation to the development of metabolic diseases and/or complications that emerge from these pathologies. Inhibition of metaflammation should provide positive impact, particularly in the context of MetS. This modulation can be also useful to control weight and body composition.
Recently, an innovative industrial process for whole whey fermentation has been developed that results in a malleable protein matrix (MPM) containing whey proteins, peptides, a proprietary Lactobacillus kefiranofaciens strain, exopolysaccharides, and calcium. 8,9 MPM stimulates the innate immune defense in healthy animals 10 and exhibits an anti-inflammatory effect comparable to that of hydrocortisone in an atopic dermatitis model. 11 MPM administration demonstrates a significant reduction of neutrophil infiltration associated with an inhibition of cytokine and chemokine production like interleukin (IL)-1β, IL-6, and tumor necrosis factor-α (TNF-α) in a murine air pouch model. 12 This latter result suggests that MPM could modulate chronic inflammation and exerts a synergetic beneficial impact on the key features of MetS.
Indeed, some milk whey-derived ingredients are known to have the potential to be used in multibeneficial foods as a supportive measure for people suffering from MetS. Many studies are reporting potential health benefits from various, especially proteinic, whey constituents. 10,13 For example, lipid-lowering and hypotensive properties have been associated with specific whey-derived proteins and peptides. 14,15 Studies also suggest the efficacy of some fermented milk products in such therapeutic application. 16 –18
These findings led us to investigate whether supplementation with MPM, a unique fermented whey product, is able to regulate dyslipidemia in a chemically induced rat model and in a diet-induced Syrian Golden hamster model. The present study focuses also on blood glucose management (hamsters and fructose-fed rats) and hypertension in spontaneously hypertensive (SHR) rats. A functional ingredient with such beneficial effects could help control Mets and complement current therapies such as lipid-lowering, hypoglycemic, and hypotensive drugs.
Materials and Methods
Products
MPM was supplied by Technologie Biolactis Inc. (Laval, QC, Canada) in a lyophilized form. 11 The MPM is obtained by a protein-specific recuperation procedure following the fermentation of sweet whey by a proprietary L. kefiranofaciens (R2C2) isolated from kefir grain and adapted to grow in whey. 8,9 The composition of MPM is shown in Table 1. Lyophilized MPM was reconstituted in water by adding 20 g of lyophilized MPM to 80 mL of water followed by 2 minutes of homogenization at 33,000 rpm with a Tissuemiser (Fisher Scientific, Ottawa, ON, Canada). The final reconstituted product is stable at 4°C for at least 1 month.
LAB, lactic acid bacteria.
Niacin (Sigma-Aldrich Canada, Oakville, ON, Canada) was sonicated for 20 minutes and dissolved in sterile water in order for the animals to receive a dose of 100 mg/kg in a daily volume of 1 mL. Niacin served as a positive control in the chemically induced dyslipidemia study because of its potent lipid-altering capacities for raising the level of HDL-C and lowering the levels of TG and LDL-C and of its demonstrated beneficial effects in the poloxamer 407 (P-407)-induced hyperlipidemia animal model. 19
The P-407 (BASF Corp., Mississauga, ON, Canada) solution for intraperitoneal injection was prepared at a concentration of 300 mg/mL by combining the agent with sterile water and refrigerated overnight. All syringes were kept on ice prior to P-407 administration to maintain the polymer in a mobile viscous state, in order to facilitate injection. 20
Lovastatin (Sigma-Aldrich Canada) was dissolved in 0.5% methylcellulose and served as a positive control in the dyslipidemia study with hamsters because of its well-known cholesterol-lowering properties as an inhibitor of 3-hydroxy-3-methyl-glutaryl-coenzyme A (HMG-CoA) reductase. 21
Metformin (Sigma-Aldrich Canada) was dissolved in water and served as a positive control in the high-fructose diet model in rats because it is an antidiabetic agent that reduces blood glucose levels and improves insulin sensitivity. 22
Enalapril maleate (Sigma-Aldrich Canada) was dissolved in water and served as a positive control in the hypertension study because of its well-known antihypertensive properties and of its demonstrated beneficial effects on systolic blood pressure (SBP) in SHR rats. 23
Animals
Animals were housed under specific pathogen-free conditions and maintained in a 12-hour light/dark cycle. All animals received water and food ad libitum. All procedures using rats in this study were in accordance with the institution's guide for the care and use of laboratory animals and approved by the institutional animal care and user committee of the INRS-Institut Armand-Frappier (Laval, QC, Canada). The high fat/high cholesterol (HFHC) diet-induced hypercholesterolemia study using Syrian Golden hamsters was in accordance with the institution's guide for the care and use of laboratory animals and approved by the institutional animal care and user committee of Collège d'Enseignement Général et Professionnel de Lévis-Lauzon (Levis, QC, Canada).
P-407-induced hypertriglyceridemia study
Female Wistar rats (7 weeks old, weighing 125–150 g) were purchased from Charles River Canada (Montreal, QC, Canada). Six rats were randomly assigned to various treatment groups except for the untreated group, where 11 rats were assigned. Rats were pretreated orally, once daily for 7 days, with 1 mL of water (placebo group), 1 mL of reconstituted MPM (1 g/kg), or 1 mL of niacin (100 mg/kg). 19 Following the pre-treatment with the different products, all animals were made hypertriglyceridemic by an intrapeitoneal injection of 1 mL of P-407 (300 mg/mL). 19,24 Treatments continued once daily throughout the experiment. Blood collection was performed for analysis of TG levels at the beginning of the experiment (basal levels), after 7 days of pretreatment with the different products (comparison of post-treatment lipid levels), and at 72 hours post-induction of hypertriglyceridemia. Food was removed 16–18 hours before blood collection. One milliliter of blood was collected from the jugular vein and immediately transferred in lithium-heparinized plastic tubes. Tubes were lightly shaken and centrifuged to allow separation of the plasma. Plasma samples were collected in clean 1.5-mL microtubes and immediately frozen at −80°C until the time of analysis. For blood collection, each animal was anesthetized using isoflurane (AErrane®, Baxter Healthcare Corp., Thetford, UK). Animals were sacrificed after the last blood collection by CO2 asphyxia. TG level measurements were performed in an independent laboratory, ISO 9002 certified, offering a reliable plasma lipid quantification service (Laboratoire Biron, Brossard, QC, Canada).
HFHC diet-induced hypercholesterolemia study
Male Golden Syrian hamsters (26–29 days old) were purchased from Charles River Canada. Ten hamsters were randomly assigned to various treatment groups as a function of weight as well as plasma cholesterol. Hamsters were treated orally, once daily for a 8-week period, with 0.6 mL of water (placebo group), 0.6 mL of reconstituted MPM (1 g/kg), or 0.6 mL of lovastatin (12.5 mg/kg). These animals were given diet D12107 (Research Diets, Inc., New Brunswick, NJ, USA) providing 40% of calories from fat and containing 0.5% cholesterol during the entire experiment. The animals were given food and water ad libitum during the experimental period. Body weight was determined at the initiation of the experiment and was measured weekly thereafter along with the determination of food intake. Blood lipid parameters (total cholesterol, HDL-C, and LDL-C) were measured after 2 weeks of treatment. Plasma glucose and insulin levels were measured at the end of the experiment (8 weeks of treatment). Food was removed 16–18 hours before blood collection. From 300 to 500 μL of blood was collected from the jugular vein and immediately transferred to EDTA-containing plastic tubes (Sarstedt) for blood lipid measurement. For glucose and insulin measurement, 100 μL of blood was collected from the saphenous vein in nonanesthetized animals and immediately transferred in EDTA-containing plastic tubes. Tubes were lightly shaken and centrifuged to allow separation of the plasma. Plasma samples were collected in clean 1.5-mL microtubes and immediately frozen at −80°C until the time of analysis. For blood collection, each animal was anesthetized using isoflurane. Samples for all experimental groups were analyzed for total cholesterol and HDL-C. Plasma cholesterol (and HDL fraction) was assayed by an enzymatic method 25 adapted for measuring in 96-well plates, which requires a minimal volume. Plasma HDL-C was isolated from total cholesterol by precipitation of apolipoprotein B-containing lipoproteins (non-HDL fraction) with sodium phosphotungstate-magnesium chloride. 25 Plasma LDL-C was measured by difference between total cholesterol and HDL-C. Plasma glucose was measured with a portable glucometer (OneTouch®, LifeScan, Inc., Milpitas, CA, USA). The insulin level was determined by enzyme-linked immunosorbent assay according to direction from the manufacturer (EZRMI-13K, Linco Research, St. Charles, MO, USA).
High fructose diet-induced hyperglycemia study
Female Wistar rats (7 weeks old) were purchased from Charles River Canada. Six rats were randomly assigned to various treatment groups. Rats given a high fructose diet were treated orally, once daily with 1 mL of water (placebo group), 1 mL of reconstituted MPM (1 g/kg), or 1 mL of metformin (50 mg/kg) for 2 weeks, after which an oral glucose tolerance test (OGTT) was performed. Body weight was determined at the initiation of the experiment and was measured daily. Food was removed 16–18 hours before the OGTT. A glucose solution (2 g/kg) was given orally to each rat. Blood drops were withdrawn from the tail, and the glucose level was measured at 0, 20, 40, 60, 90, and 120 minutes post-glucose challenge using the FreeStyle Mini® blood glucose monitoring system (Abbott Diabetes Care, Inc., Alameda, CA, USA). The area under the curve (AUC) for plasma glucose concentration over a 120-minute period was calculated with a linear trapezoidal method. 26
Hypertension study
Female SHR rats rats (6 weeks old) were purchased from Charles River Canada. Ten rats were randomly assigned to various treatment groups. In order for blood pressure to spontaneously rise, rats were maintained on a regular diet for 2 weeks before starting the treatments. Hypertensive SHR rats were then treated daily with 1 mL of water (placebo group), 1 mL of reconstituted MPM, or 1 mL (1 g/kg) of enalapril maleate (10 mg/kg) (Sigma-Aldrich Canada). 23 Treatments continued once daily for 4 weeks and were stopped for the last week of the experiment. SBP was measured with the automated RTBP2000 Tail Blood Pressure system (Kent Scientific, Torrington, CT, USA). Data collections were made weekly, and the average of three measurements was taken as the initial mean SBP. Data were acquired and analyzed with Biopac Student Lab Pro® software version 3.6.1 (BIOPAC Systems, Inc., Goleta, CA, USA).
Statistical analysis
Statistical analyses were performed using a repeated measure one-way analysis of variance (ANOVA) test. Error bars represent ± SEM values. Statistical significance was considered at P < .05. Values between .05 and .1 were also mentioned and considered as a trend toward significance.
Results
P-407-induced hypertriglyceridemia study
The impact of MPM supplementation on plasma TG level was determined by the P-407-induced hypertriglyceridemia rat model. TG levels before and after P-407 treatment are shown in Figure 1. After 7 days of supplementation, the TG level (Fig. 1A) was lowered by 38% in the MPM-treated group (1.13 ± 0.11 mmol/L) compared to the placebo group (1.83 ± 0.15; P < .01). This reduction in TG level in MPM-treated animals is comparable to what we see with the niacin-treated animals (1.00 ± 0.08 mmol/L), which represents a 45% decrease. TG levels 72 hours after injection of P-407 (Fig. 1B) rose up to 83.49 ± 5.86 mmol/L for the placebo group compared to 54.63 ± 10.46 mmol/L for the MPM-treated animals and 57.14 ± 10.24 mmol/L for the niacin-treated animals, showing a reduction of 35% and 32% (P < .05), respectively, in plasmaTG levels.
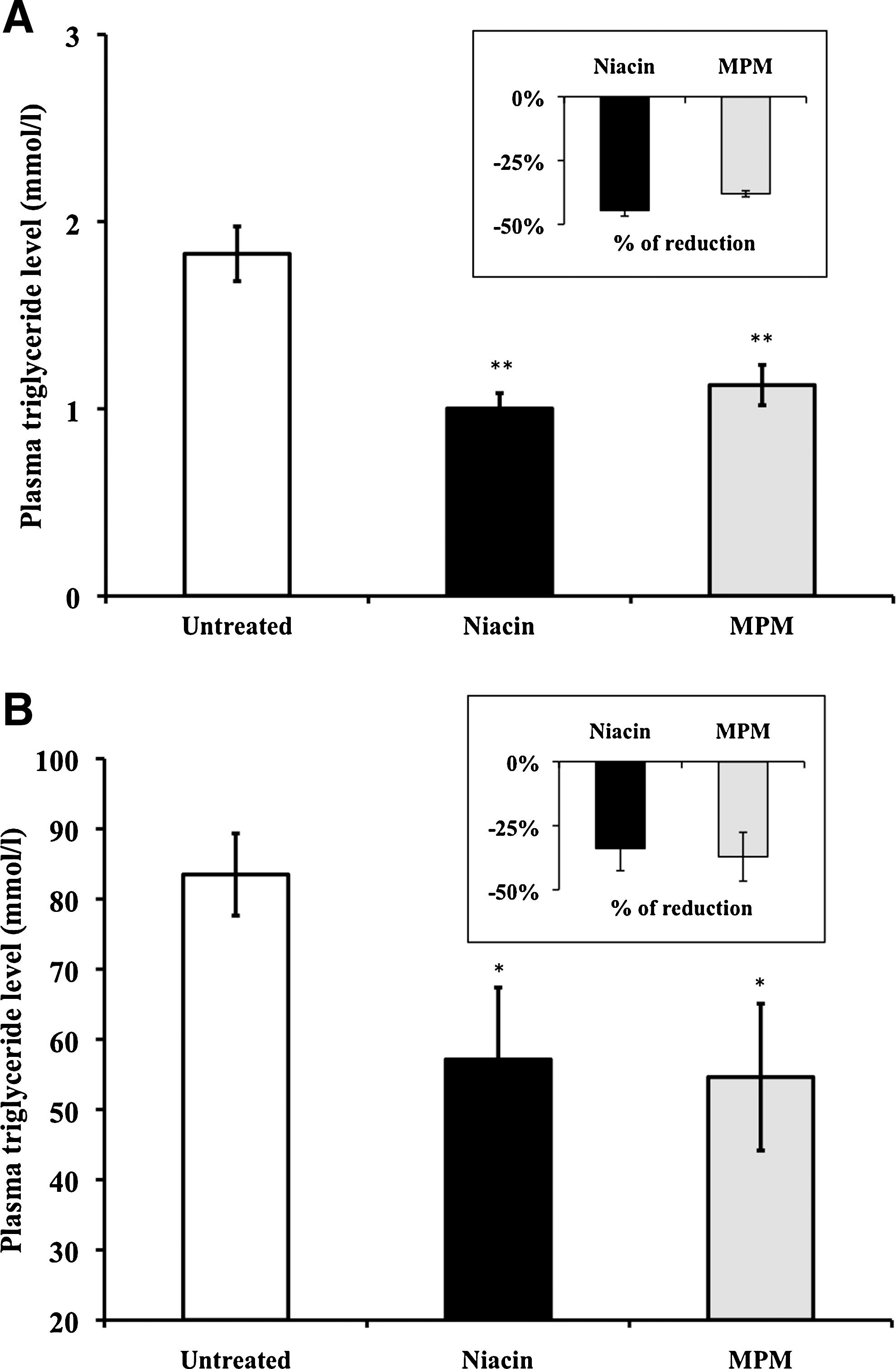
Effects of MPM compared to niacin on plasma TG level in Wistar rats (
HFHC diet-induced hypercholesterolemia study
The average body weights at baseline were similar among groups. The average for weight gain, food intake, and food efficiency in Syrian Golden hamsters during the 2 weeks of MPM supplementation are summarized in Table 2. Daily food consumption was less for lovastatin-treated hamsters (5.26 ± 0.18 g/day; P < .05) on the HFHC diet compared to the untreated animals on the same diet (7.26 ± 0.14 g/day). Weight gain and food efficiency were not significantly different between the two groups. However, food efficiency (28.45 ± 1.83%; P < .05) and weight gain (1.96 ± 0.13 g/day; P < .05) were higher with MPM-treated hamsters compared to untreated animals on the same HFHC diet.
Data are mean ± SEM values (n = 10).
*P < .05 is significantly different from untreated group on the HFHC diet for each row.
Plasma cholesterol levels in Syrian Golden hamsters after 2 weeks of MPM supplementation are shown in Figure 2. The administration of MPM reduced the total plasma cholesterol level, increased the HDL-C level, and lowered the LDL-C level, leading to a better HDL-C/LDL-C ratio than the placebo group (Fig. 2). The total cholesterol level (Fig. 2A) was 8.48 ± 0.42 mmol/L for the MPM-treated animals in comparison to 10.33 ± 0.82 mmol/L for the untreated animals, resulting in a reduction of 18% (P < .05). Treatment with lovastatin slightly reduces cholesterol by 8%. Both lovastatin and MPM significantly increased the HDL-C level (Fig. 2B) by 35% (4.01 ± 1.36 mmol/L) and 17% (3.46 ± 1.17 mmol/L), respectively, in comparison to the placebo group (2.96 ± 0.13 mmol/L; P < .01). Also, both lowered the LDL-C level (Fig. 2C): by 32% for MPM-treated animals (5.02 ± 0.68 mmol/L; P < .05) and by 26% for lovastatin (5.47 ± 0.74 mmol/L) compared to the placebo group (7.36 ± 0.91 mmol/L). The HDL-C/LDL-C ratio (Fig. 2D) was improved significantly for both lovastatin (0.78 ± 0.11 [65% increase]) and MPM-treated animals (0.76 ± 0.10 [61% increase]) compared to the untreated animals (0.47 ± 0.007; P < .05).
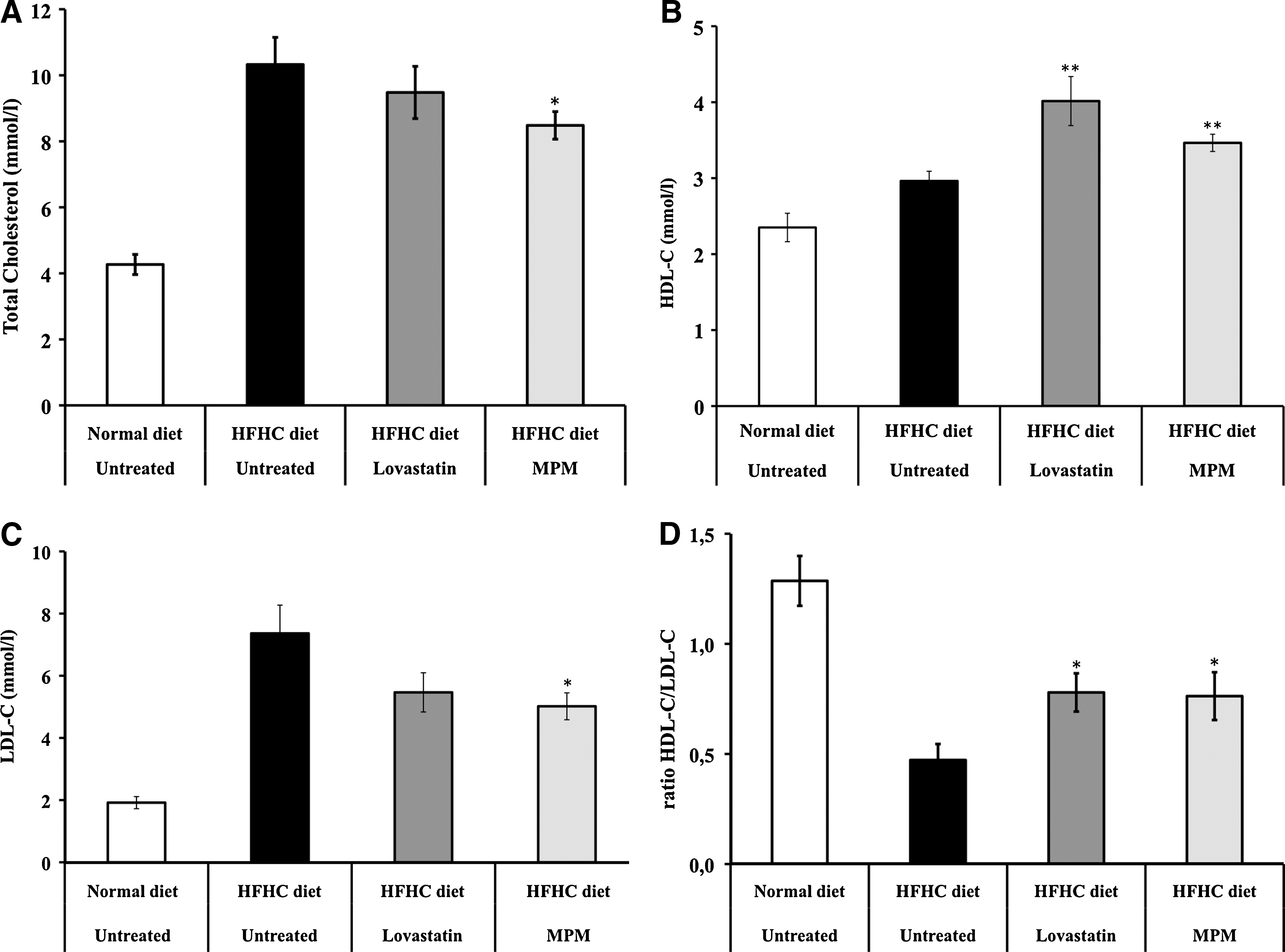
Effect of MPM compared to lovastatin on (
The treatment lasted 8 weeks, when the combination of the HFHC diet and lovastatin became toxic for all the animals in this group. MPM-treated animals showed severe signs of dyslipidemia in which plasma lipid levels were comparable to those of the untreated control group on the same diet (data not shown). The administration of MPM did not reduce significantly the fasting glucose level and the insulin level (Fig. 3). However, MPM supplementation led to a better fasting glucose to insulin ratio (FGIR) compared to the untreated group on the same HFHC diet (Fig. 3). The fasting glucose level (Fig. 3A) was 82.00 ± 6.97 mg/dL for the MPM-treated animals in comparison to 96.77 ±11.95 mg/dL for the untreated animals on the HFHC diet, resulting in a reduction of 15% (P = .289). Animals on the HFHC diet showed a 43% increase (P = .102) in fasting glucose level compared with animals on a normal diet (67.64 ± 3.06 mg/dL), but only a 21% increase (P = .185) occurred when MPM was added to the diet. The insulin level (Fig. 3B) was 12.55 ± 1.44 μU/mL for the MPM-treated animals in comparison to 11.66 ± 1.10 μU/mL for the untreated animals on the HFHC diet, resulting in an increase of 8% (P = .638). Animals on the HFHC diet showed a 15% increase (P = .416) in insulin level compared with animals on a normal diet (10.18 ± 1.27 μU/mL), but a 23% increase (P = .185) when MPM is added to the diet. The FGIR (Fig. 3C) is improved in MPM-treated animals on the HFHC diet (6.77 ± 0.97), representing a reduction of 22% compared to the untreated group on the same diet (8.64 ± 0.92; P = .07). Remarkably, the FGIR of MPM-treated animals (6.77 ± 0.97) on the HFHC diet is comparable to the FGIR in untreated animals on a normal diet (7.00 ± 0.80; P = .779).
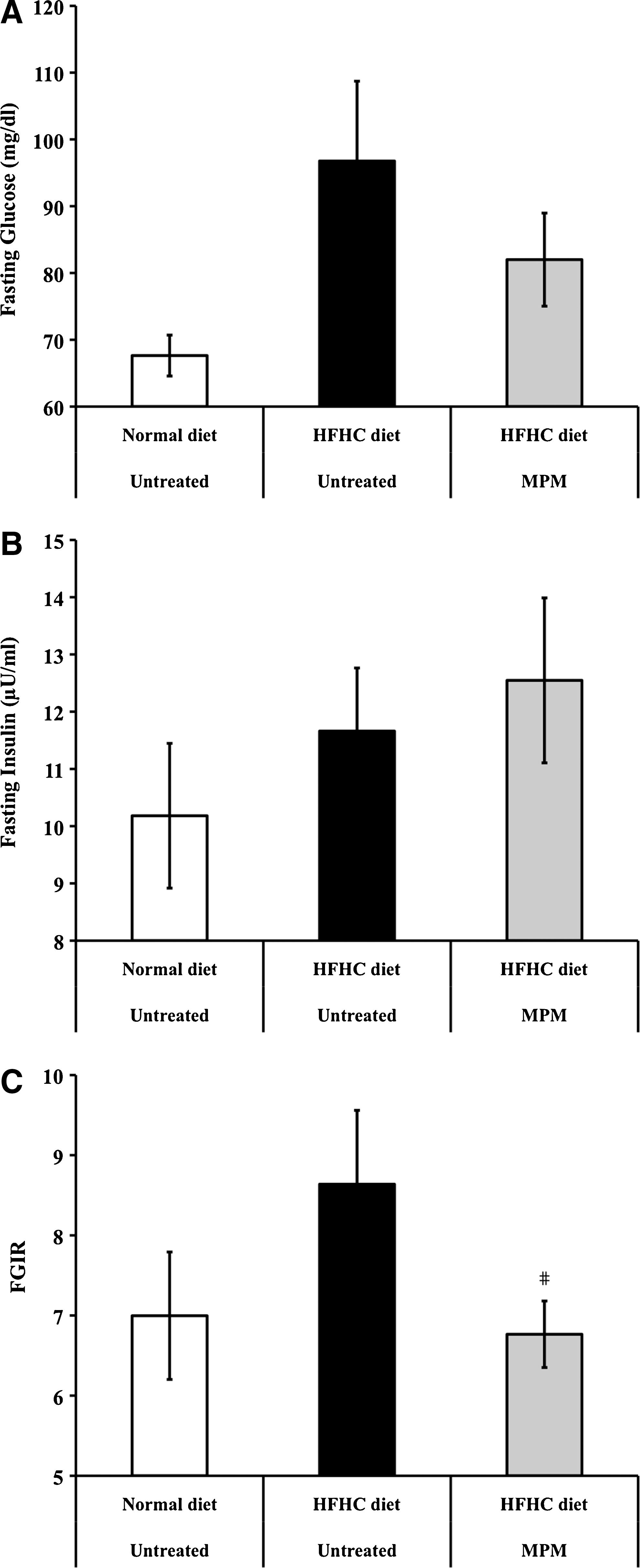
Effects of MPM on (
High fructose diet-induced hyperglycemia study
Growth rate and plasma glucose levels for Wistar rats after 2 weeks of MPM supplementation or metformin are shown in Figure 4. No significant growth rate differences were observed between the groups (Fig. 4A). OGTTs were performed on those animals (Fig 4B). MPM-treated animals on the high fructose diet showed a reduction in plasma glucose level (756.58 ± 17.40 mmol/L/120 min) compared to the placebo group (842.83 ± 55.72 mmol/L/120 min; P = .09) and compared to the metformin-treated animals (864.00 ± 8.41 mmol/L/120 min; P < .01). Also, the OGTT result of MPM-treated animals (756.58 ± 17.40 mmol/L/120 min) on the high-fructose diet is comparable to that of untreated animals on a normal diet (761.83 ± 15.85 mmol/L/120 min).

Effects of MPM and metformin on (
P < .01, significantly different for the MPM-treated group on a fructose diet compared with the metformin-treated group on a fructose diet in the one-way ANOVA statistical analysis.
Hypertension study
The impact of MPM supplementation on SBP was determined using SHR rats. SBP of each animal was periodically measured, and a period of 2 weeks was necessary to achieve high SBP (Fig. 5). At baseline (week 0), SBP was similar for the three groups. Blood pressure did not change over a 4-week period for the placebo group (181.06 ±5.25 mm Hg) but was reduced by 25% to a normal blood pressure level in the enalapril-treated animals (143.46 ±5.89 mm Hg; P < .01). The MPM-treated animals showed a 13% reduction in SBP (164.01 ± 7.10 mm Hg; P < .05) after 4 weeks compared to the placebo group.
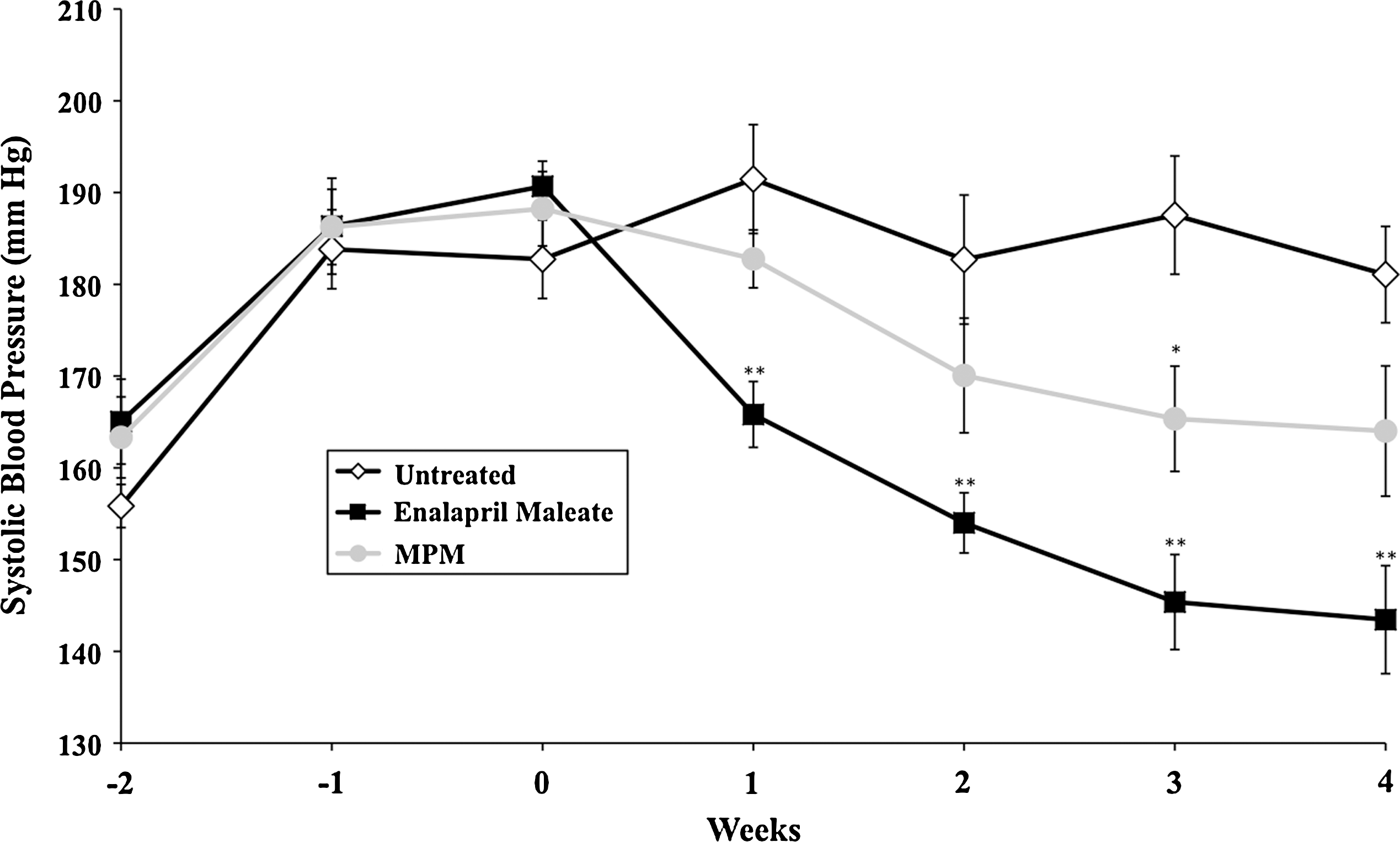
Effects of MPM compared to enalapril maleate on SBP in SHR rats treated for 4 weeks. Data are mean ± SEM values (n = 12). *P < .05, **P < .01, significantly different from the untreated group in the one-way ANOVA statistical analysis.
Discussion
In this study, we examined the effect of MPM supplementation to potentially regulate TG level, cholesterol level, blood glucose, and hypertension in different animal models. MPM lowers the TG level in a P-407-induced dyslipidemia rat model, comparable to niacin treatment. It also reduces total cholesterol and LDL-C levels and raises the HDL-C level in Syrian Golden hamsters fed on a HFHC diet for 2 weeks. MPM reestablishes the FGIR index to normal levels in this latter model and lowers the plasma glucose level AUC in fructose-fed rats after 2 weeks of treatment. In SHR rats, MPM-treated animals showed a reduction of SBP for 4 weeks. Results from this study suggest that MPM is a functional ingredient with beneficial effects on lipid metabolism, blood glucose control, and hypertension that might contribute to the management of MetS and thus reducing the risk of CVDs.
As a new target for lifestyle change and drug therapies, prevention and control of MetS are believed to reduce CHD and T2DM-related mortality and would therefore have a positive impact on health-related costs and quality of life. The preferred way to reduce the prevalence of MetS is by implementation of healthy nutritional and lifestyle habits. Besides major nutrients (saturated and unsaturated fats, cholesterol, carbohydrates, etc.), many new dietary factors used in so-called functional foods or as nutraceuticals are now recognized to impact on some of the individual features of MetS. However, because MetS is a cluster of many metabolic disorders, a food or nutraceutical able to deliver multiple benefits at a time could be view as highly desirable as part of a therapeutic lifestyle change intervention. 27
In the P-407-induced dyslipidemia animal model, a regulation of TG levels was observed for the group treated with MPM as seen by the prevention of the increase of plasma TG levels compared to the control group. The efficacy of MPM to regulate induced hyperlipidemia was compared to that of niacin throughout the studies. Niacin is a well-documented drug for its lipid-lowering properties, 28,29 and its efficacy has been demonstrated with the P-407 animal model of hyperlipidemia. 19 Interestingly, in the hyperlipidemia study, treatment with MPM had a similar impact to that of niacin. A reduction of plasma TG was observed in both these groups: levels were 35% lower 72 hours after the injection of P-407. A single P-407 injection causes a dose-dependent hyperlipidemia in rats, increasing plasma TG more than 60-fold with a dose of 300 mg. 30 This increase in plasma TG has been reported to be largely due to the inhibition of lipoprotein lipase, the major enzyme responsible for the hydrolysis of plasma lipoprotein TG, 30 suggesting that MPM could regulate the activity of lipoprotein lipase.
The induction of hyperlipidemia in rats with injection of P-407 is an interesting model to rapidly evaluate the effect of a product on lipid disorders, particularly on TG. This model allows to obtain indications on the effect of the product on hyperlipidemia, but does not represent the lipid disorders observed in humans. The hamster fed with an HFHC diet is a more representative model of the lipid metabolism and conditions observed in humans. 31,32 In this model, MPM reduced total cholesterol and LDL-C levels and increased the HDL-C level in hamsters, which is comparable to a lovastatin treatment. The statins, like lovastatin, are inhibitors of HMG-CoA reductase. The HMG-CoA reductase is an enzyme that converts HMG-CoA into mevalonic acid. The inhibition of this enzyme activity results in the decrease in biosynthesis of cholesterol, which leads to an increase in HMG-CoA reductase and number of hepatic receptors for LDL-C. This increase in LDL receptors consequently leads to a decrease in blood LDL-C. 33 The benefits obtained by MPM supplementation are not the results of a possible toxic adverse event. Animals receiving MPM gained weight, and food efficiency was better compared to the placebo group on the same diet. This could be explained by the extra caloric intake of 0.42 kcal/day associated with MPM consumption.
In this latter model, MPM treatment did not reduce the fasting glucose level and did not increase significantly the insulin level. However, it led to a better FGIR compared to the untreated group and reached a level comparable to animals on a normal diet. The relationship between MPM supplementation and glucose management in this model did not reach the level of statistical significance, although a trend was present. Indeed, the insulin level seemed higher after MPM treatment. The large SEM observed indicate wide variations in individual responses. Studies showing that diets rich in monounsaturated fatty acids, such as oleic acid, or certain proteins, such as whey protein, improve glycemic control and result in a greater insulin release compared with a control meal with the same glucose content in Zucker rats 34 and in humans. 35 Whey proteins have insulinotropic effects and can reduce postprandial glycemia. This effect may involve the incretin hormones glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1. 36 One of the main components of MPM is sweet whey, suggesting that the insulinotropic effect observed here could be whey-dependent.
MPM-treated animals on the high fructose diet showed a reduction in plasma glucose level compared to the placebo group and to the metformin-treated group, reaching a level comparable to untreated animals on a normal diet. It has been suggested that administration of whey proteins produces a significant reduction in dipeptidyl peptidase IV (DPP-IV) activity in the proximal small bowel that leads to an increase in levels of incretin, which inhibits glucagon release (which increases the blood glucose) but more importantly increases insulin secretion and decreases gastric emptying. 36 Whey digestion generates di- and tripeptides that could act as DPP-IV competitive inhibitors like the well-known diprotin A (Ile-Pro-Ile) and diprotin B (Val-Pro-Leu). 37 MPM is the result of fermentation of whey proteins by L. kefiranofaciens R2C2, potentially producing bioactive peptides that will inhibit DPP-IV activity before the luminal digestion and thus regulating blood glucose and insulin levels.
Animals receiving MPM showed a reduction in SBP after 7 days of feedings. Reduction of SBP in the MPM group was observed throughout the study and was still significant at week 4. Enalapril was used as a positive control in the hypertension study because of its demonstrated hypotensive properties on SHR rats, 38 allowing comparison to the effects of MPM. After 4 weeks of feedings, SBP of enalapril-treated rats had returned to normal values. The SBP values of MPM-treated animals were considerably decreased compared to the control group. These results demonstrated that MPM possesses a significant antihypertensive effect. Fermentation of milk with Lactobacillus was shown to produce bioactive peptides inhibiting angiotensin-converting enzyme and therefore had a positive impact on hypertension. 39,40 Hypertensive female SHR rats force-fed with MPM, a fermented whey product, showed reduced SBP in comparison to the group force-fed water. A reduction of SBP was observed upon daily administration of MPM and was maintained for 4 weeks. In comparison with other studies using either fermented dairy products and/or peptides isolated from these fermented products, this level of SBP reduction compares well to previous reports. 39 –45
Few fermented products containing whey are currently available. Kawase et al. 18 studied the impact of a fermented milk containing whey on lipid levels of rats and healthy men. Treatment with the fermented milk reduced total cholesterol in rats and had positive effects on HDL and TG in men. 18 Such fermented products are desirable functional ingredients for the management of lipid-related health problems. MPM is a novel, complex fermented whey product containing whey proteins, calcium, and L. kefiranofaciens R2C2. Many components found in MPM could be responsible for the effects observed on hyperlipidemia, hyperglycemia, and hypertension. Whey proteins are recognized to have a positive impact on lipid and glucose levels. 13,36 MPM contains also important quantities of calcium, which plays a role in the regulation of energy metabolism and obesity risk. 46 A possible synergistic effect of whey and calcium in controlling obesity was also suggested. 46 Furthermore, the exopolysaccharide kefiran, which is produced by L. kefiranofaciens R2C2, was recently shown by others to have a beneficial impact on lipid metabolism in laboratory animals. 47 Another interesting compound found in whey is nicotinamide riboside, a molecule part of the niacin (vitamin B3) family. This molecule has recently been identified as a new vitamin that could be an alternative to niacin as a useful lipid-lowering supplement. To date, the only product in which this molecule has been found is whey. 48 The bacteria themselves could even have probiotic properties and influence lipid metabolism. Many Lactobacillus strains have been suspected to have cholesterol-lowering effects by producing short-chain fatty acids in the intestine that can then inhibit hepatic cholesterol synthesis or redistribution of plasma cholesterol to the liver, by interfering with cholesterol absorption from the intestine or by directly assimilating cholesterol. 49,50 However, the effect of short-chain fatty acids on lipid metabolism remains controversial. 51
We have previously showed that MPM administration inhibits the production of inflammation markers such as IL-1β, IL-6, and TNF-α in a murine air pouch model. 12 This latter result suggested that MPM could modulate chronic inflammation and exert a beneficial impact on metabolic disorders. Most adipose tissue in mammals is white adipose tissue. It contains adipocytes, preadipocytes, endothelial cells, fibroblasts, leukocytes, and macrophages. These macrophages are derived from the bone marrow, and their number correlates with the appearance of obesity and homeostatic or metabolic cascade imbalance. 6 Various mediators (IL-1β, IL-6, and TNF-α) are synthesized by macrophages and adipocytes, contributing to local and systemic inflammation, perturbation in glucose management and lipid profile, vascular endothelial dysfunction, hypertension, and vascular inflammation. 7 In that context, MPM administration should prevent hyperlipidemia, hyperglycemia, and hypertension by negatively regulating the granulocyte-dependent response and thus preventing recruitment of immune cells from the bone marrow like macrophages in adipose tissue. This will downregulate the production of pro-inflammatory cytokines like IL-6 and TNF-α and impair the crosstalk between adipocyte and macrophages to restore homeostasis.
Patients with MetS typically have a mixed dyslipidemia, high blood pressure, and high fasting plasma glucose. 52 Lipid metabolism of patients with MetS is often less efficient, which is comparable to what is happening in animals following injection of poloxamer. Angiotensin-converting enzyme inhibitors and statins were shown useful in the treatment of MetS. 52 Niacin has also been recognized to effectively treat dyslipidemia found in MetS, 53 but adverse effects such as flushing and hepatic toxicity have minimized its use. MPM is a natural functional ingredient that showed the capacity to regulate dyslipidemia, in two different animal models, to control blood glucose, and to reduce SBP in SHR rats. The effects observed after MPM consumption on dyslipidemia, blood glucose, and hypertension, three major symptoms of MetS, demonstrate that it could be used as an adjunct therapy for prevention of MetS and related CVDs. Also, we have previously demonstrated that MPM treatment led to a reduction in pro-inflammatory inducers like IL-6 and TNF-α, 12 thus lowering low-grade inflammation often seen in MetS patients.
In conclusion, the results suggested a beneficial impact on MetS associated with consumption of the fermented whey product MPM. Statins are undisputedly the gold standard in the treatment of dyslipidemia, and more effective monotherapies are unlikely to be identified and developed in the near future. Niacin has also been used in men with efficacy, but its side effects do not allow a high patient compliance. Therefore, MPM is being positioned as a natural bioactive ingredient that could be used as an adjunct to statin or niacin therapy or as a functional ingredient complementing those current therapies. A product such as MPM has many advantages compared to other products or drugs on the market because of its multifunctional properties, making it a key nutraceutical ingredient for individuals suffering from MetS, CVD, atherosclerosis, and possibly diabetes. Such roles and applications of MPM will, however, need to be investigated in a well-designed, placebo-controlled human study. The fact that the fermented product looks like regular yogurt is very interesting, making it easy to introduce in the everyday diet of consumers. A nutraceutical ingredient regulating dyslipidemia, controlling blood glucose elimination, and having hypotensive and immunoregulating properties should be considered a product with a high potential on prevention or control of lipid-associated diseases and MetS and will be most likely a good candidate for functional food formulation.
Footnotes
Acknowledgments
The project was supported by a strategic grant (STP 246405-01) from the Natural Sciences and Engineering Research Council of Canada in collaboration with Technologie Biolactis Inc. The authors wish to thank M. Roger Dubuc and Mme. Dalie St-Georges for their technical assistance. J.B. holds a Ph.D. scholarship from the Fonds de Recherché en Santé du Québec.
Author Disclosure Statement
J.B., E.T., and P.L. are scientists and employees for Technologie Biolactis Inc. C.D. has served as a co-investigator for and received research funding from Technologie Biolactis Inc. and from the Natural Sciences and Engineering Research Council of Canada. E.M. is a scientist for TransBiotech and has received funding from Technologie Biolactis Inc. and from a PART subsidy. L.-P.P. received a Natural Sciences and Engineering Research Council of Canada industrial grant in collaboration with Technologie Biolactis Inc. No other competing financial interests exist.