
Abstract
Palm oil is a common cooking ingredient used in the commercial food industry as the second largest consumed vegetable oil in the world. Because of its lower cost and highly saturated nature, it usually maintains a solid form at room temperature and is used as a cheap substitute for butter. However, there has been a growing health concern about palm oil because of the link between dietary fats and coronary heart disease. Palm oil contains ∼49% saturated fat, a relatively high concentration compared with other vegetable oils. Consequently, high intakes of saturated fat from palm oil induce a larger increase in plasma concentrations of total cholesterol and low-density lipoproteins. In the present study, we examined the hyperlipidemia of palm oil and the risk of cardiovascular disease (CVD) using a rat model in comparison with sunflower oil with a relatively low level of saturated fat. On in vivo examination using Sprague-Dawley (SD) rats for 22 days, there were no significant differences in serum lipid levels, suggesting that palm oil may not cause hyperlipidemia and elevate CVD risk. However, liver samples obtained from SD rats fed with palm oil showed a lot of large lipid inclusions stained with the Oil Red O working solution, but not much lipid accumulation was observed in rats treated with sunflower oil. In addition, lipid accumulation in the mixed oil group fed the combination of palm and sunflower (1:1) oil was shown to be at an intermediary level between the palm oil group and sunflower oil group. Taken together, these results indicate that palm oil, a highly saturated form of vegetable oil, may induce dysfunction of the liver lipid metabolism before affecting serum lipid levels. On the other hand, sunflower oil, a highly unsaturated vegetable oil, was shown to be well metabolized in liver.
Introduction
E
Palm oil is regarded as an alternative to partially hydrogenated oils containing trans fats, although controversial issues remain. 5 However, as much as its huge consumption, there has been a growing health concern about palm oil because of the link of dietary saturated fats to coronary heart disease. 6 Although palm oil does not contain cholesterol like other vegetable oils, the high saturated fat concentration of palm oil is associated with hyperlipidemia, which is a leading contributor to cardiovascular disease (CVD). 7,8 Particularly, the palmitic acid in palm oil has been associated with the increased risk of coronary heart disease. 9 In addition, the usage of repeated heated palm oil was reported to be the predisposing factor to atherosclerosis leading to CVDs. 10 It has been reported that palm oil is strongly associated with higher rates of death from myocardial infarction in low and middle income countries. 11 According to a USDA report (2011), palm oil contains ∼49% saturated fat, as opposed to 17% in peanut oil, 16% in soybean oil, and 7% in canola/rapeseed oil. The 49% saturated fatty acids (SFAs) of palm oil consist of 1.0% myristic acid (C14), 43.5% palmitic acid (C16), and 4.3% stearic acid (C18). On the other hand, the content of total polyunsaturated fatty acids (PUFAs) of palm oil is merely 9.3%. Consequently, a high intake of saturated fat from palm oil induces a larger increase in plasma concentrations of total cholesterol (T-CHO) and low-density lipoproteins (LDLs). 12,13
In contrast, other studies insist that the health concern over palm oil has been excessively considered and the benefit effect is rather to be supposed. According to Chong and Ng, feeding experiments in various animal species and humans did not support the allegation that palm oil raised the blood cholesterol level and it was atherogenic. 14 Palm oil was rather reported to be beneficial; palm oil consumption reduced blood cholesterol and the risk of arterial thrombosis, artherosclerosis, and inhibited platelet aggregation. 6,14 Therefore, the health effect of palm oil still remains to be elucidated. In the present study, we examined the hyperlipidemic effects of palm oil and the risk of CVD using a rat model in comparison with sunflower oil to accurately evaluate its health effects. Sunflower oil is the nonvolatile oil compressed from sunflower (Helianthus annuus) seeds. As sunflower oil can be used in conditions with extremely high cooking temperatures, it has been used as a common cooking oil for frying at home, restaurants, and food industries. Because sunflower oil contains 11% saturated fat, which is much lower than palm oil, high levels of PUFAs (65–75%) and appreciable quantities of vitamin E, sterols, squalene, and other aliphatic hydrocarbons, it may be considered that there may be a variety of health benefits associated with the consumption of sunflower oil. 15,16 Especially, standard sunflower oil has as much as 65.7% PUFAs in the form of C18 linoleic acid. Linoleic acid is an essential fatty acid, which means that the human body cannot synthesize it from other food components and it must be consumed for proper health. According to the reports, a diet only deficient in linoleate caused mild skin scaling, hair loss, 17 and poor wound healing in rats. 18
In this study, we measured triglyceride (TG), T-CHO, LDL cholesterol, high-density lipoproteins (HDLs), and cholesterol levels in serum after dietary administration of palm oil, sunflower oil, and the combination of two oils (1:1) in male Sprague-Dawley (SD) rats. We also examined their effect on lipid accumulation in rat liver tissues by histochemical analysis. From the serum lipid concentrations, CVD risk factors such as cardiac risk index (CRI) and atherogenic index (AI) were calculated as the blood levels of LDL cholesterol and HDL cholesterol, which are closely associated with the development of CVD. 19,20
Materials and Methods
Animal adaptation
Healthy male SD rats were purchased from Central Laboratory Animal, Inc. (Seoul, Republic of Korea). Seven-week-old male SD rats were housed in a conventional animal facility at the Laboratory Animal Research Center of Chungbuk National University (Cheongju, Republic of Korea). The animals were allowed to acclimate for 1 week after arrival. All rats were used for in vivo experiments in accordance with the approved institutional guidelines of Chungbuk National University (CBNU-A-605-13-01).
Basic diet preparation
The rats were fed AIN-76 purified diets (Harlan Laboratory, Madison, WI, USA) during the experimental period. It contains casein,
Administration of lipid diets to rats
Male SD rats weighing 309±5.03 g were divided into four groups; 2.5 mL of each experimental diet was orally administered once a day to each rat of each group through a Zonde needle. The control group (n=5) was not treated with any oils. The treatment groups (n=5 each) included (1) the palm oil group treated with 2.5 mL palm oil/rat/day, (2) the sunflower oil group treated with 2.5 mL palm oil/rat/day, and (3) the mixed oil group treated with 2.5 mL of the combination of palm and sunflower (1:1) oil. Palm oil and sunflower oil were purchased from Sigma-Aldrich Corp. (St. Louis, MO, USA).
Analysis of body weight
The body weights of SD rats were measured before feeding at 2- or 3-day intervals for 22 days.
Analysis of serum lipids
During the experimental period, blood samples were collected on day 22, the last day of the experimental period. On the day of blood collection, all rats were starved for 18 h and blood samples were then collected from the tail vein after anesthesia using ether. Ten to twelve hundred cc of blood was collected using a Vacuum Serum Separation Tube (SST; Green CROSS CORP., Yongin, Gyeonggi, Republic of Korea) and left at room temperature for 1 h. Serum was isolated from the blood samples by centrifugation at 1977 g at 4°C for 20 min and then stored at −20°C. Serum analysis was conducted with a HITACHI Clinical Analyzer 7080 (Hitachi Korea Ltd., Seoul, Republic of Korea) to measure the serum concentrations of various lipid components, including TG, T-CHO, HDL cholesterol, and LDL cholesterol. The AI and CRI were determined based on serum LDL cholesterol, HDL cholesterol, and T-CHO concentrations. The AI was calculated as (T-CHO−HDL cholesterol)/HDL cholesterol. 21 The CRI was calculated as T-CHO/HDL cholesterol. 22
Histological analysis by Oil Red O staining
At 24 h after the last oral administration of the experimental diets, liver tissues were harvested from the sacrificed rats and immediately frozen in a −80°C cryongenic freezer. Frozen liver tissues were cryosectioned (6-μm thick), fixed in a 10% formalin solution (OCI Company Ltd., Seoul, Republic of Korea) at 4°C for 5 min, and then rinsed three times with distilled water. A 5% Oil Red O working solution was prepared by dissolving Oil Red O powder (Sigma-Aldrich) in propylene glycol (OCI Company Ltd.) and used to stain the sectioned tissues according to the manufacturer's instructions. Counter staining was conducted with hematoxylin (Sigma-Aldrich) and the sections were then mounted in glycerine (OCI Company Ltd.). Lipid-containing cells were detected as ones containing red inclusions using a light microscope (BX51 U-LH100HGWIG; Olympus, Tokyo, Japan; ×200 and ×400 magnification).
Statistical analysis
All data were analyzed using GraphPad Prism software (San Diego, CA, USA). In vitro data are presented as the mean±SEM. A one-way analysis of variance was performed followed by Dunnett's multiple comparison test. P-values<.05 were considered to be statistically significant.
Results
Body weight
The initial mean body weight of the rats was 309±5.03 g and increased in only two groups (the sunflower oil group and the combination of palm and sunflower [1:1] oil group) during the study (Fig. 1). The body weights of SD rats administrated with sunflower oil and the combination of palm and sunflower oil increased significantly to 349±19 g and 355.25±10.53 g, respectively, at the end of the experiment. However, there were no significant increases in body weights of the rats of the control and palm oil groups. Rather, the body weight of the rats administrated with palm oil was decreased at the initial stage of the experiment, which was attributed to diarrhea. As palm oil is in the semisolid state at room temperature, it is thought that palm oil is hard to digest and be absorbed by rats. After 7 days of adaptation, the diarrhea subsided and the body weight returned to normal without any increases compared to a control.
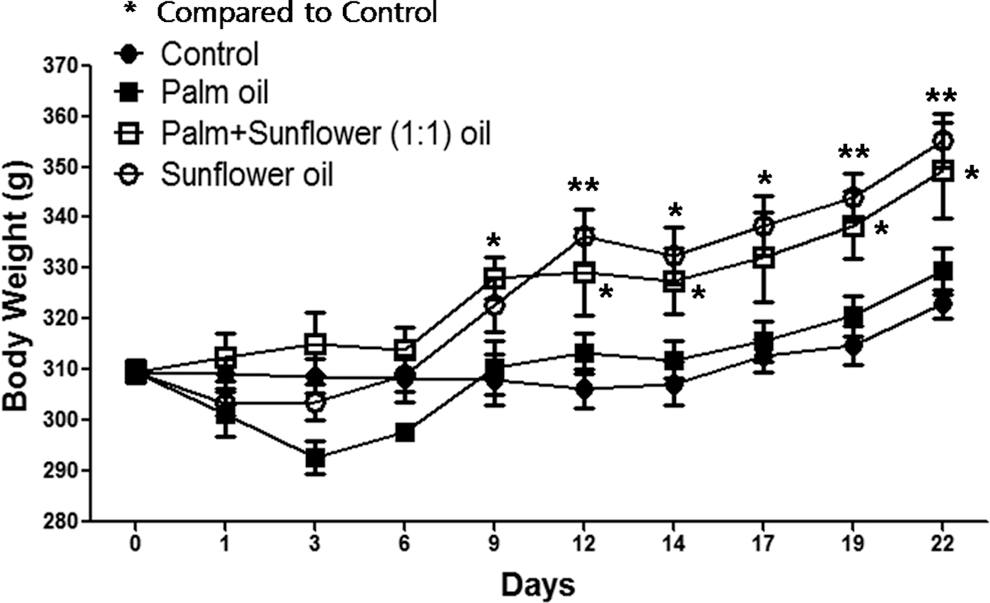
The body weights of animals during the experimental period. The body weights of Sprague-Dawley rats of each group were measured at 2- or 3-day intervals for 22 days. The animals were treated as follows. The control group received no oil. The palm oil group received 2.5 mL palm oil/rat/day. The mixed oil group received 2.5 mL of the combination of palm and sunflower (1:1) oil/rat/day. The sunflower oil group received 2.5 mL sunflower oil/rat/day. *P<.05, **P<.01 (Dunnett's multiple comparison test).
Serum lipid concentrations
Serum lipids, including HDL cholesterol, LDL cholesterol, T-CHO, and TGs were measured twice during the experiment period, at 10 days (a middle stage) and 22 days (a last stage). Because the results at 10 days showed no significant changes between groups, only the results of 22 days were presented in Figs. 2 –4. For HDL cholesterol, there was a significant reduction in the palm oil group compared with the control group (Fig. 2A). For LDL cholesterol, there were significant changes between groups (Fig. 2B). For T-CHO, the palm oil group showed a significant decrease compared with the control group, but other groups had no changes (Fig. 3A). For TG, there was a significant reduction only in the sunflower oil group compared with the control group, although there was a decreasing trend in the palm oil group. Unlike these results, the combination of palm and sunflower oil group did not result in any changes compared with the control group (Fig. 3B).
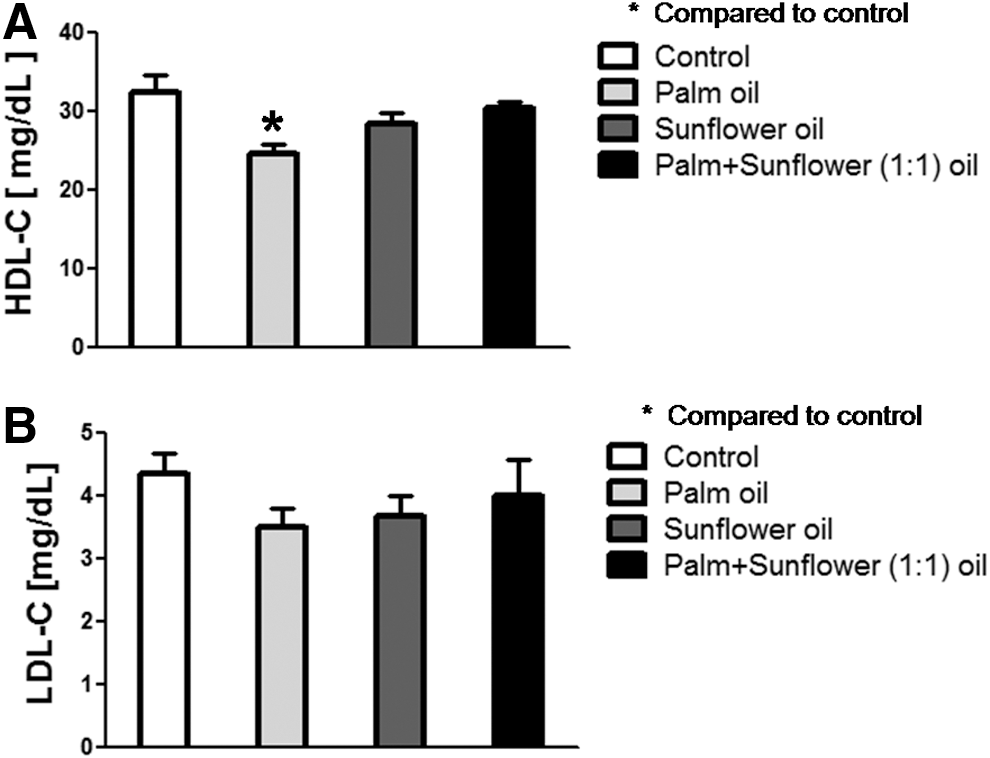
Serum high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) analysis. After oral administration of palm oil, sunflower oil, and the combination of palm and sunflower (1:1) oil, blood samples were collected at the end of the experiment and left at room temperature. Serum was isolated from the blood samples by centrifugation and the serum concentrations of HDL-C and LDL-C were measured.
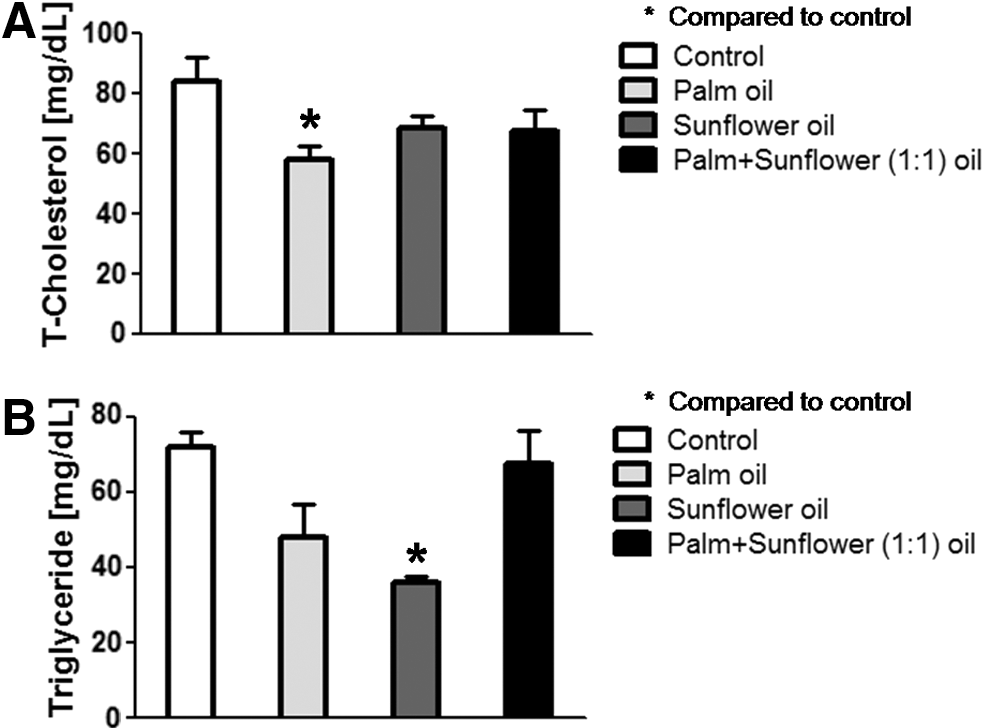
Analysis of triglyceride (TG) and total cholesterol (T-CHO) serum concentrations. After oral administration of palm oil, sunflower oil, and the combination of palm and sunflower (1:1) oil, blood samples were collected and left at room temperature. Serum was isolated from the blood samples by centrifugation and the serum concentrations of TG and T-CHO were measured.
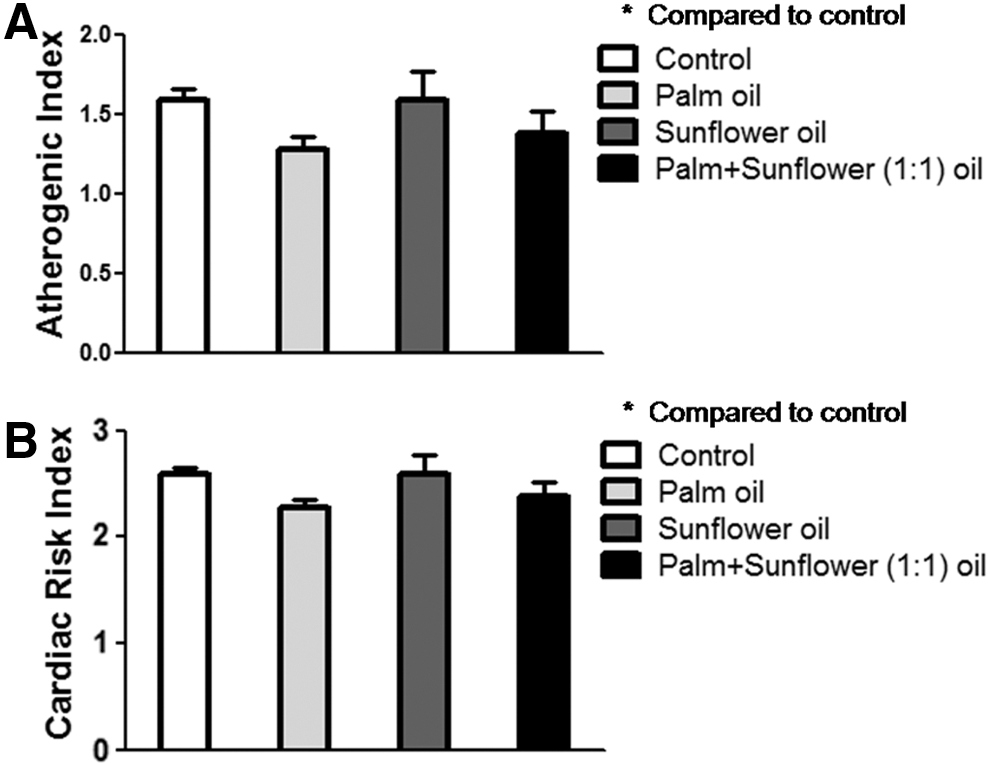
Atherogenic index (AI) and cardiac risk index (CRI) analysis. After measuring serum lipid concentrations, values for each factor were calculated as follows: AI=(T-CHO−HDL cholesterol)/HDL cholesterol and CRI=(T-CHO−HDL cholesterol/HDL cholesterol).
CVD risk factors
CVD risk, CRI and AI, of rats fed palm oil, sunflower oil, and the combination of palm and sunflower oil was calculated from the results of serum lipid concentrations. Although there were some modest changes in serum lipid concentrations between groups, the values converted to AI and CRI of each group showed no differences compared to the control group, respectively, as shown in Fig. 4A and B.
Lipid accumulation in live tissues
Lipid accumulation in SD rat liver tissues was detected by Oil Red O staining in the histological analysis and shown in Fig. 5. The red spots or inclusions corresponded to lipids derived from TG and T-CHO from the oil diet. Significant levels of lipid accumulation were observed in the palm oil group. Numerous large red spots were detected in most liver samples (90%) obtained from the rats fed palm oil and any red spots were not detected in only two samples (6.67%) from the palm oil group (Fig. 5B). On the contrary, large red spots were detected in only three samples (13.64%) obtained from the rats fed sunflower and no red spots were detected in 11 samples (50%) of the sunflower oil group (Fig. 5D). Lipid accumulation in the palm plus the sunflower oil group was recorded to be at the intermediate level between the palm oil group and sunflower oil groups (Fig. 5C). These quantitative data measured from the histological images are presented in Table 1.
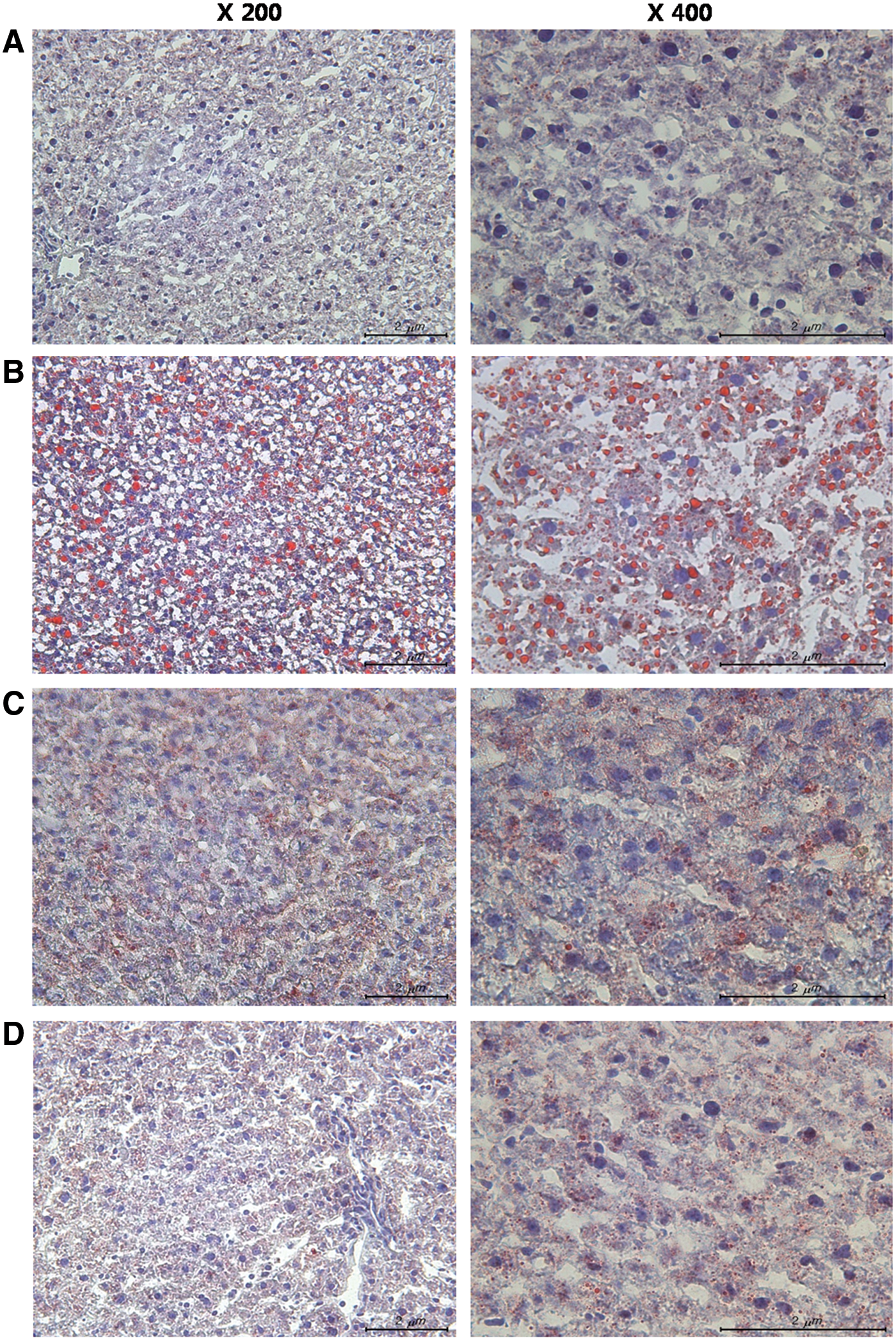
Histological analysis of liver tissues. After oral administration of palm oil, sunflower oil, and the combination of palm and sunflower (1:1) oil, liver tissues were harvested from the rats, frozen, cryosectioned, and stained with an Oil Red O working solution. Counterstaining was conducted with hematoxylin and the tissue sections were then mounted with glycerine. Lipid in the cells appeared as red inclusions under a light microscope (×200 and ×400 magnification).
Discussion
CVD refers to any disorders that affect the heart itself and/or the circulatory system, including coronary heart disease, cardiomyopathy, ischemic heart disease, atherosclerosis, and congestive heart failure. 23 It has been the biggest cause of death worldwide over the last two decades 24 and increased the economic burden due to high costs of medical treatment. 25,26 Hyperlipidemia, an abnormal elevation of any or all lipids and/or lipoproteins in the blood, is a leading contributor to mortality due to CVD 7 and is mainly caused by hypercholesterolemia and unhealthy ratios of the two smallest lipoprotein cholesterols LDL cholesterol and HDL cholesterol. LDL cholesterol is often called bad cholesterol because it tends to form deposits in the walls of arteries while circulating through the bloodstream, decrease artery diameter, and result in atherosclerosis. 27 On the contrary, HDL cholesterol is referred to as good cholesterol because it can maintain the healthy state of the inner blood vessel walls by scavenging and recycling cholesterol through transporting it to the liver where it can be reprocessed. 28 –30 Accordingly, CVD risk indicators such as AI and CRI are measured from the blood levels of LDL cholesterol, HDL cholesterol, and T-CHO. The larger the index value, the greater the risk of CVD. As hyperlipidemia is usually caused by a high-fat diet, palm oil, which is one of the most consumed vegetable oils globally and a highly saturated oil, has been suspected to be a cause of hyperlipidemia and CVD. 31
As the assertion of the dangers of palm oil is still disputable, we examined its effect on hyperlipidemia comparing it with another vegetable oil, sunflower oil. In vivo examination using SD rats for 22 days revealed no significant alterations in serum lipid levels, showing that palm oil may not cause hyperlipidemia and elevate CVD risk. Surprisingly, palm oil was shown to significantly reduce both T-CHO as well as HLD cholesterol, a good cholesterol. Therefore, there were no significant effects on AI or CRI. Contrary to our expectations, sunflower oil, which is considered a heart-healthy oil, did not affect HDL cholesterol, LDL cholesterol, and T-CHO, but sunflower oil did significantly reduce serum TG. Sunflower oil also did not influence AI or CRI. Unlike the results from serum lipid levels, we detected outstanding consequences in lipid accumulation in live tissues. Liver tissues obtained from SD rats fed palm oil showed a lot of large lipid inclusions stained with the Oil Red O working solution, but not much lipid accumulation was observed in rats treated with sunflower oil. In addition, lipid accumulation of the combination of palm and sunflower oil group was shown to be intermediate between the palm oil group and sunflower oil groups, as expected.
Liver is a vital organ playing a major role in cholesterol homeostasis and it especially produces bile, an alkaline compound, which aids in digestion through the emulsification of lipids. In terms of lipid metabolism, liver is quantitatively a major site of cholesterol synthesis and secretion. Nascent HDLs and very LDLs are synthesized and secreted into the circulation by the liver, and mature forms of lipoproteins such as LDLs, intermediate-density lipoproteins, and HDLs are taken up by the liver in a regulated manner. Therefore, total plasma cholesterol levels are closely related with the liver function. 32 In the present study, palm oil was shown to be hard to metabolize in the liver tissue. Compared with palm oil, sunflower oil was more easily metabolized in the liver. Although this phenomenon was associated with the lowering effect of sunflower oil on the total serum cholesterol level, unfortunately there were no general relationships between lipid accumulation in the liver and serum lipid levels in this study. This may be due to the differences in the rat lipid metabolism and/or the selection of the test period used in this study. The effect of long-term chronic exposure to these oils needs to be studied to obtain better results. Nevertheless, we obtained a meaningful result from the current study and may conclude that palm oil can induce dysfunction in the liver lipid metabolism before affecting serum lipid levels. On the other hand, sunflower oil tends to be well metabolized in the liver. These results seem to be associated with differences in the lipid profiles of the two vegetable oils. Palm oil has more SFAs (e.g., palmitic acid) that can act as trans fats. On the other hand, sunflower oil has much more PUFAs (e.g., linoleic acid) that can act as essential fatty acids.
Footnotes
Acknowledgment
This study was supported by the Priority Research Centers Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (MEST) of the Korean government (2009-0094035).
Author Disclosure Statement
None of the authors have any conflicts of interest to declare.