
Abstract
Resveratrol, a polyphenolic compound, is a powerful antioxidant with remarkable anti-inflammatory properties. Inflammation and pain plays an important role in the pathogenesis of knee osteoarthritis (OA) and could cause tissue damage and morbidity. The aim of this study was to evaluate the anti-inflammatory and pain reduction activities of orally administered resveratrol in patients with knee OA. We carried out a 90-day pilot study to evaluate the ability of orally administered resveratrol, as an adjuvant with meloxicam, to decrease knee joint pain and biomarkers of inflammation in comparison with a placebo. One hundred ten men and women (45–75 years old) diagnosed with mild to moderate knee OA were treated with 15 mg per day meloxicam and either 500 mg per day resveratrol or placebo for 90 days in a double-blind, randomized control trial. Pain severity was evaluated at the beginning and at the end of treatment using Visual Analogue Scale-100 scores. Fasting blood was collected to determine serum interleukins 1β and 6, tumor necrosis factor-α, C-reactive protein, and complement proteins C3 and C4. The resveratrol-treated group experienced a time-dependent significant decrease in pain severity (P < .001). Serum levels of the biochemical markers were significantly reduced compared with the placebo-treated group (P < .01). These findings suggest that resveratrol may be an effective “add-on” option with meloxicam in the treatment of patients with mild to moderate knee OA.
Introduction
O
Materials and Methods
Study design
A prospective randomized, double-blind, placebo-controlled multicenter trial was conducted to evaluate the supplementary effect of resveratrol with meloxicam versus meloxicam alone on the serum levels of certain inflammatory markers in patients with knee OA. The study was performed during December 2016–October 2017, including patient enrollment, sample collection, and biochemical analysis. The trial was carried out at the outpatient department of Shar Teaching Hospital and the Specialized Rheumatology Center, Sulaimani City, Iraq. The study protocol was approved by the Research Ethics Committee of the College of Medicine, University of Sulaimani (No. 42 in November 21, 2016) in accordance with the Declaration of Helsinki and its amendments, and the Guidelines for Good Clinical Practices issued by the Committee of Propriety Medicinal Products of the European Union. All participants were asked to sign a written informed consent voluntarily before participation in the study. Patient's safety was closely monitored by a special board of specialists who conducted regular examinations during the study. The study consisted of a 12-week follow-up with four visits; first day of week 1 (day 0), week 4, 8, and 12. Each participant who enrolled in the present study was evaluated with a thorough history and physical examination to record the side effects of interventional medications. Biochemical analysis was performed for all the participants at baseline visits (pre-treatment) and last day of week 12 (post-treatment, day 90; Fig. 1).
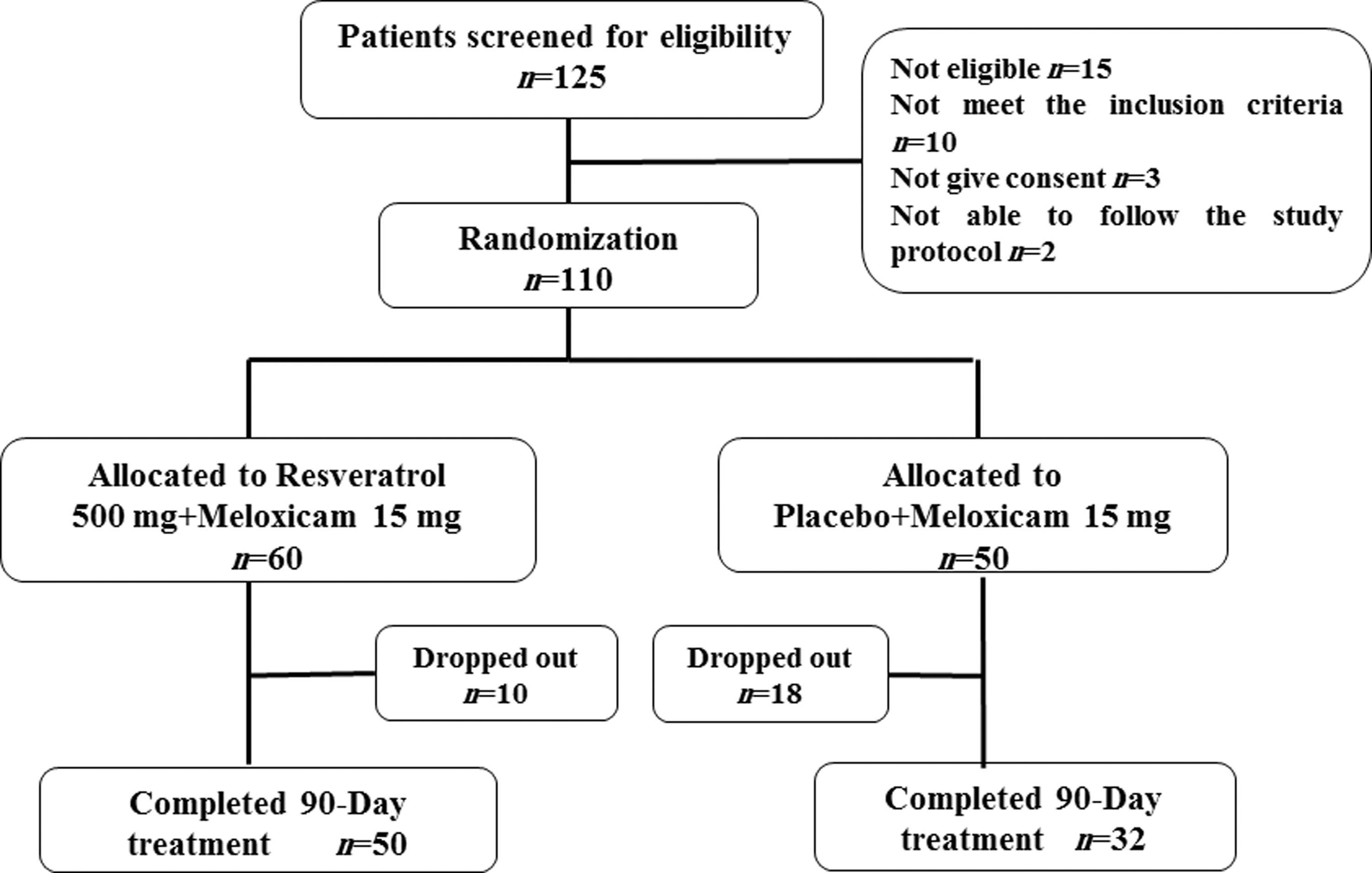
Flow diagram of participants' enrollment, randomization, intervention, dropout rate, and completion of 90-day trial. n, number of patients.
Recruitment and randomization
One hundred twenty-five patients were screened for eligibility; 110 eligible patients of both sexes (aged 45–75 years) were included in the study. All eligible participants were patients who fulfilled the American College of Rheumatology criteria for knee OA 17 and had Kellgren–Lawrence grade I–III OA of the knee, certified by radiographic imaging 18 with the presence of typical knee symptoms (pain, stiffness, disability) lasting for more than 6 months. The Kellgren–Lawrence scoring was conducted by a specialized orthopedician and a senior rheumatologist.
All candidates went through a standardized interview process and was informed about the nature of the study and the treatments. Written consents were obtained from all participants before inclusion. The intervention protocol, procedures, and potential risks and benefits of the study were also explained thoroughly to the participants. Exclusion criteria included secondary OA due to metabolic arthropathy, pain associated with acute joint trauma, patients with grade IV knee OA on the Kellgren–Lawrence grading system, infiltration of hyaluronic acid in the evaluated knee within 6 months before inclusion, and use of coumarin anticoagulants, heparins, and anti-platelets. Patients using antioxidants-containing drugs or dietary supplements that contain polyphenols were also excluded. The use of NSAIDs other than that indicated during the trial period (meloxicam) was not allowed. The participants were advised not to use any other analgesics or anti-inflammatory agents. The patients were thoroughly informed and given absolute right of withdrawal at any time during the clinical trial.
After recruitment, eligible participants were randomly and blindly assigned to one of two groups in a 1:1 ratio: first group was treated with 15 mg meloxicam (Boehringer Ingelheim, Germany) and a placebo (specially prepared for the study) administered orally once daily for 12 weeks and considered a control group (Mlx+placebo); the second group (Mlx+Res) was treated with 15 mg meloxicam and 500 mg resveratrol (Sigma-Aldrich, United Kingdom) administered orally once daily for 12 weeks. 19 Meloxicam is a well-recognized NSAID and widely prescribed to treat various types of arthritis due to its properties of reducing pain, swelling, and joint stiffness. The choice of meloxicam was based on its well-recognized gastrointestinal safety, affordability of the dosage form, and the wider use by clinicians during daily clinical practice in our region. The placebo was formulated as hard gelatin capsules that had identical color, form, and size as resveratrol capsules. All those involved in the trial (investigators, participants, data entry personnel, and statistician) were blinded to the treatment allocations.
Patients were instructed to bring their medication bottles at each visit. Remaining capsules were counted and recorded in the subject's profile to monitor patient compliance. Safety assessments were performed at all visits by the site investigator, and severity of pain was evaluated using Visual Analogue Scale-100 (VAS-100). Basic demographic information, knee OA grade based on Kellgren–Lawrence grading system, duration of symptoms, and treatment history were reported for all participants in the first visit.
Biochemical analysis
Blood samples (10 mL) were obtained from each participant twice; at baseline (first day of week 1) and at the end of the intervention (last day of week 12) to measure serum levels of the pro-inflammatory cytokines such as TNF-α, IL-1β, IL-6, and the inflammatory markers such as high-sensitivity CRP (hs-CRP) and C3, C4 complement proteins. Blood samples were left to clot, and serum was isolated by centrifugation at 1700 g for 10 min and stored at −80°C until the time of biochemical analysis. Serum was analyzed for IL-1β, IL-6, and TNF-α using an enzyme-linked immunosorbent assay (ELISA) kit (Bioassay Technology Laboratory, Korain Biotech Co., Ltd., Shanghai, China) according to the manufacturer's instructions. The analysis of hs-CRP and complement proteins C3 and C4 was performed by spectrophotometric method utilizing ready-made kits (Roche Diagnostics GmbH, Mannheim, Germany) according to the manufacturer's recommendations.
Statistical analysis
Detailed statistical analyses were performed using Graph Pad Prism 5.0.1 software (Graph Pad Software, Inc., CA). The baseline demographic data and patient characteristics were compared between the treatment groups. Categorical data were analyzed with the chi-square test. Continuous variables were analyzed using independent sample t-test or the two-way ANOVA and Bonferroni's post hoc test. A P-value <.05 was considered as statistical significance.
Results
In the present study a total of 125 patients were assessed for eligibility, and 110 patients were recruited and randomized to the study protocol. Of these, 28 dropped out from the study (18 from Mlx+placebo group and 10 from Mlx+Res group) because they were not fully complying with one or more aspects of the protocol. This left 82 patients (50 of Mlx+Res group and 32 in the Mlx+placebo group) who completed all the scheduled visits and provided blood at post-intervention (day 90).
Baseline demographic characteristics
The basic characteristics of the participants are given in Table 1. The results show comparable values for the measured parameters between the two groups. No significant differences in age, gender, body weight, body mass index, and disease grade or disease duration between the two groups were observed. Moreover, the baseline value of the biochemical tests was also not significantly different between the two groups, except for TNF-α; the serum level of TNF-α was significantly higher in the group that used supplementary resveratrol with meloxicam compared with the group that used meloxicam alone. Clinical assessment parameters of pain were found to be nonsignificantly different between the two groups.
Demographic Data and Baseline Characteristics of Knee Osteoarthritis Patients Treated with Meloxicam Supplemented with Resveratrol (Mlx+Res) or Meloxicam with Placebo (Mlx+placebo)
BMI, body mass index; KOOS, Knee Injury and Osteoarthritis Outcome Score; VAS, Visual Analogue Scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Assessment of pain severity
Figure 2 indicates that severity of pain, measured by VAS-100, was not significantly different between the Mlx+placebo and Mlx+Res groups at baseline (P > .05). However, adjuvant use of resveratrol produced a significant decrease in pain score compared with baseline values (64% and 72.5%, respectively) and meloxicam alone after 30 and 60 days, and no further significant decrease in pain severity was achieved after 90 days compared with the values obtained before. Furthermore, the effect of meloxicam alone remained nonsignificantly different after 60 and 90 days.
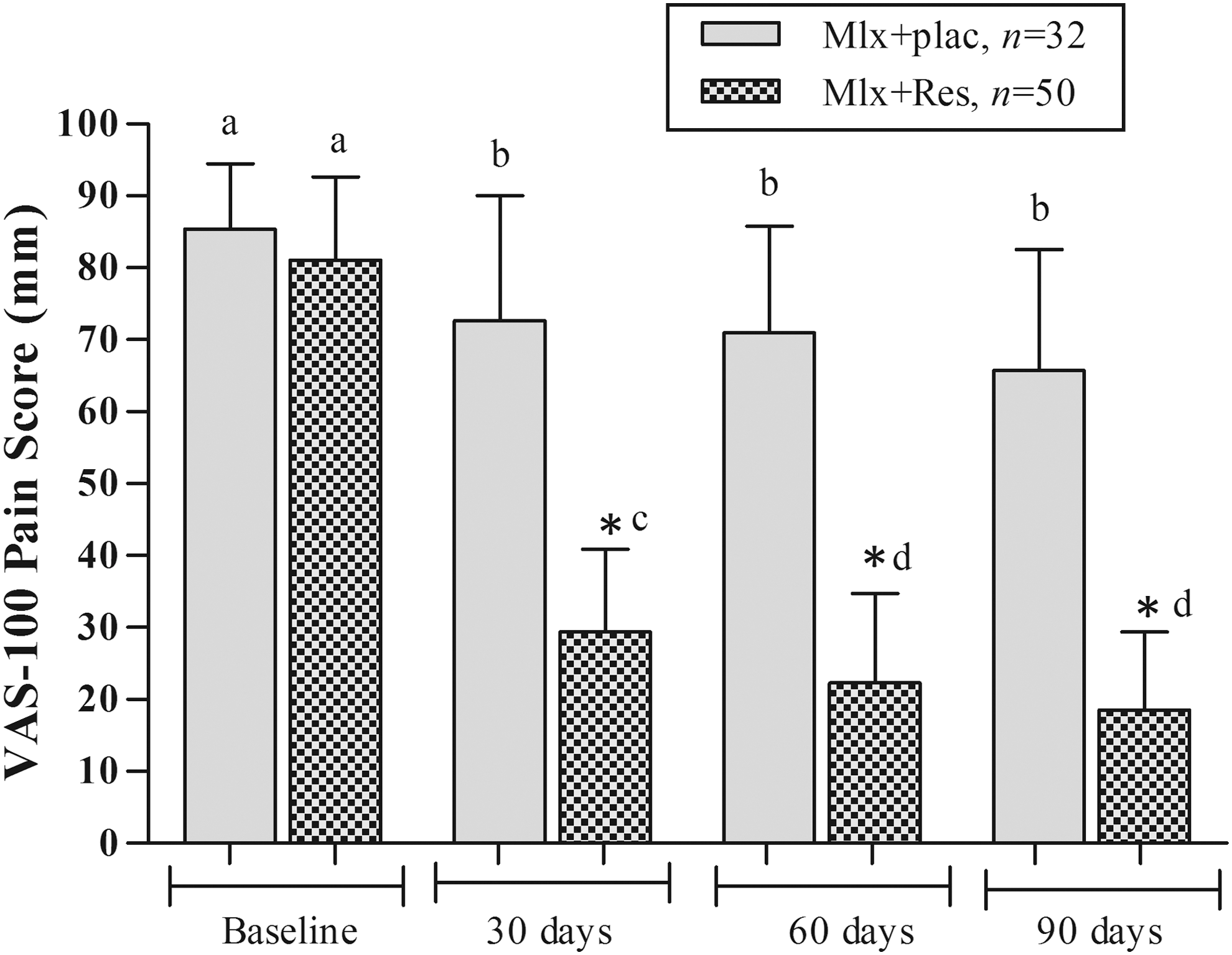
Effect of resveratrol, as adjuvant with meloxicam for 90 days, on the pain severity of patients with mild to moderate knee OA measured by VAS-100. * represents significant difference compared with control group at the same time period (P < .05); values with non-identical letters (a, b, c, d) among groups are considered significantly different (P < .05). OA, osteoarthritis; VAS, Visual Analogue Scale.
Pro-inflammatory markers
In Figure 3, adjuvant use of resveratrol significantly decreased serum levels of the pro-inflammatory cytokine TNF-α in patients with knee OA treated with meloxicam for 12 weeks (P < .05), compared with both the baseline level and that of the group treated with meloxicam alone. Additionally, analysis of TNF-α in the group treated with meloxicam alone showed nonsignificant elevation of this biomarker within the same period (P > .05). Moreover, treatment with resveratrol in supplementation with meloxicam also resulted in a significant reduction in the serum levels of IL-1β and IL-6 after 90 days, compared with both the baseline values and those reported in Mlx+placebo group within the same period. However, statistically nonsignificant elevation was noted in the levels of both biomarkers (IL-1β and IL-6) in Mlx+placebo group compared with the baseline values (Figs. 4 and 5). In contrast, the combination of resveratrol and meloxicam significantly decreased the serum levels of complement proteins C3 and C4 (P < .05) after 12 weeks of treatment compared with the baseline values of the same group and the values of the group treated with meloxicam alone (Figs. 6 and 7). Moreover, Figure 8 indicated that 90 days of treatment with resveratrol, as adjuvant with meloxicam, produced a significant decrease in serum hs-CRP levels compared with both the baseline values and the levels of the corresponding group that used meloxicam alone (P < .05).
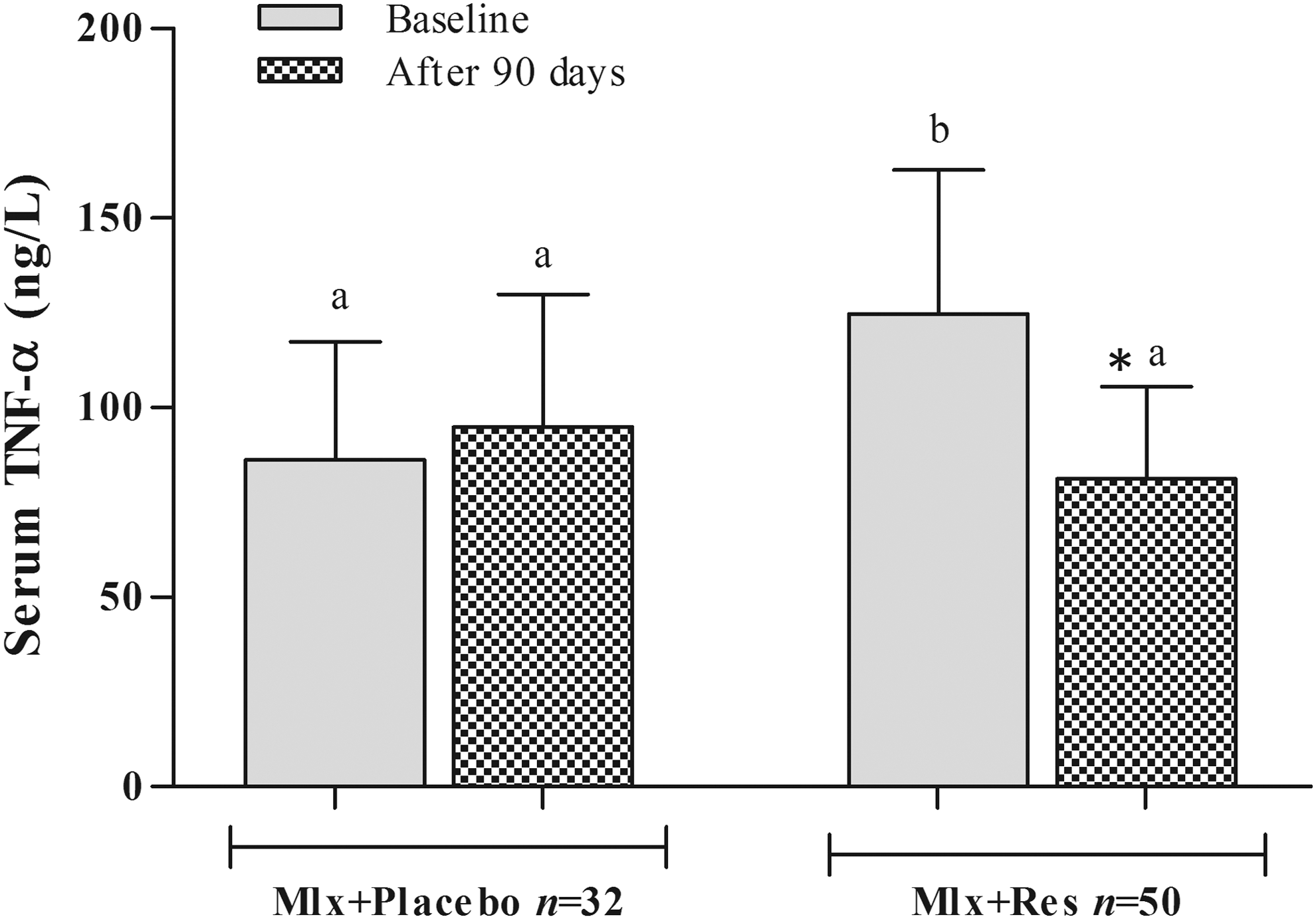
Effects of resveratrol, as adjuvant with meloxicam, on serum level of TNF-α in patients with mild to moderate knee OA. * represents significant difference compared with baseline of the same group (P < .05); values with different letters (a, b) are significantly different among different groups (P < .05). Mlx, meloxicam; OA, osteoarthritis; Res, resveratrol; TNF, tumor necrosis factor.
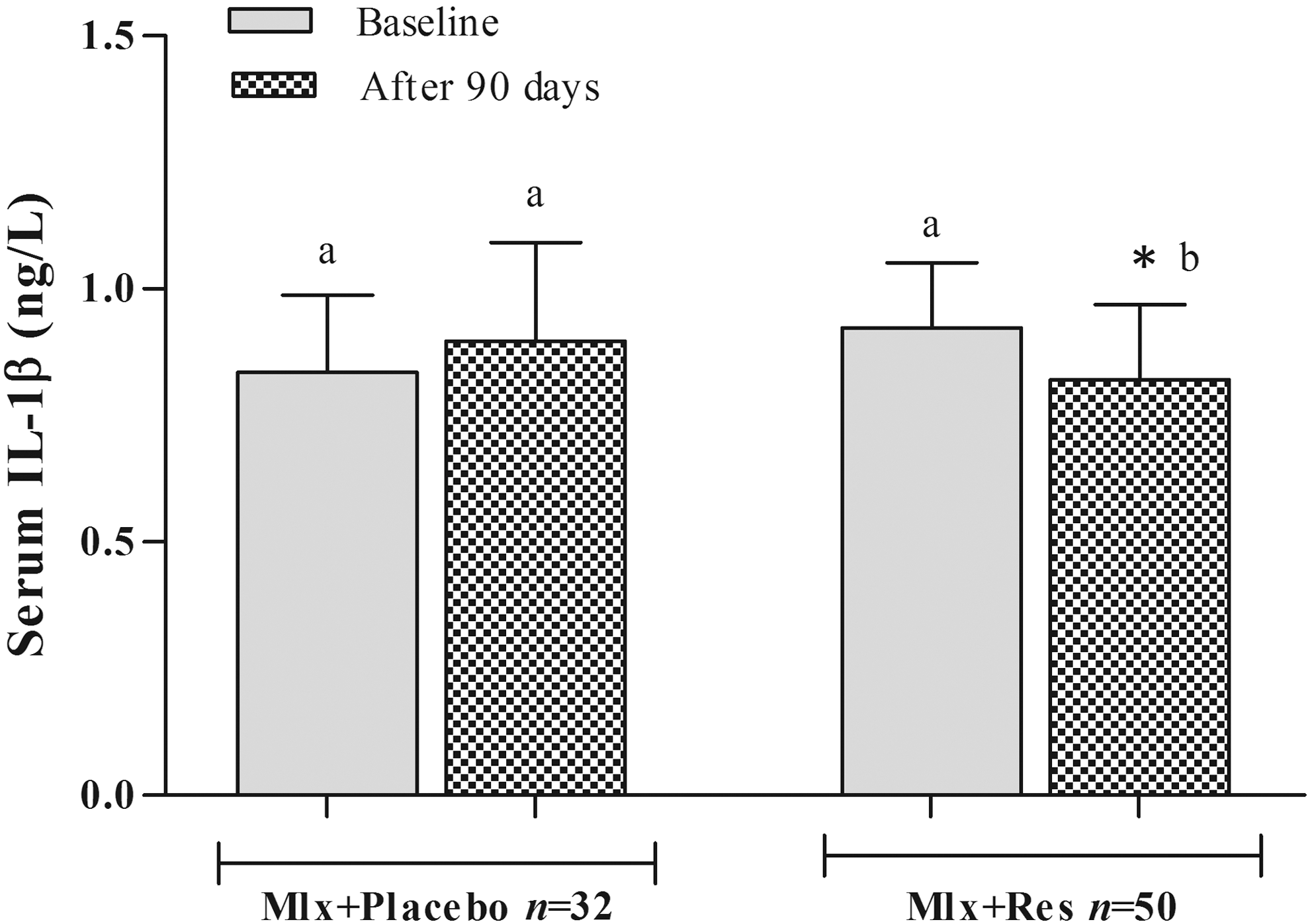
Effects of resveratrol, as adjuvant with meloxicam, on serum level of IL-1β in patients with mild to moderate knee OA. * represents significant difference compared with baseline value of the same group (P < .05); values with different letters (a, b) are significantly different among different groups (P < .05). IL, interleukin; OA, osteoarthritis.
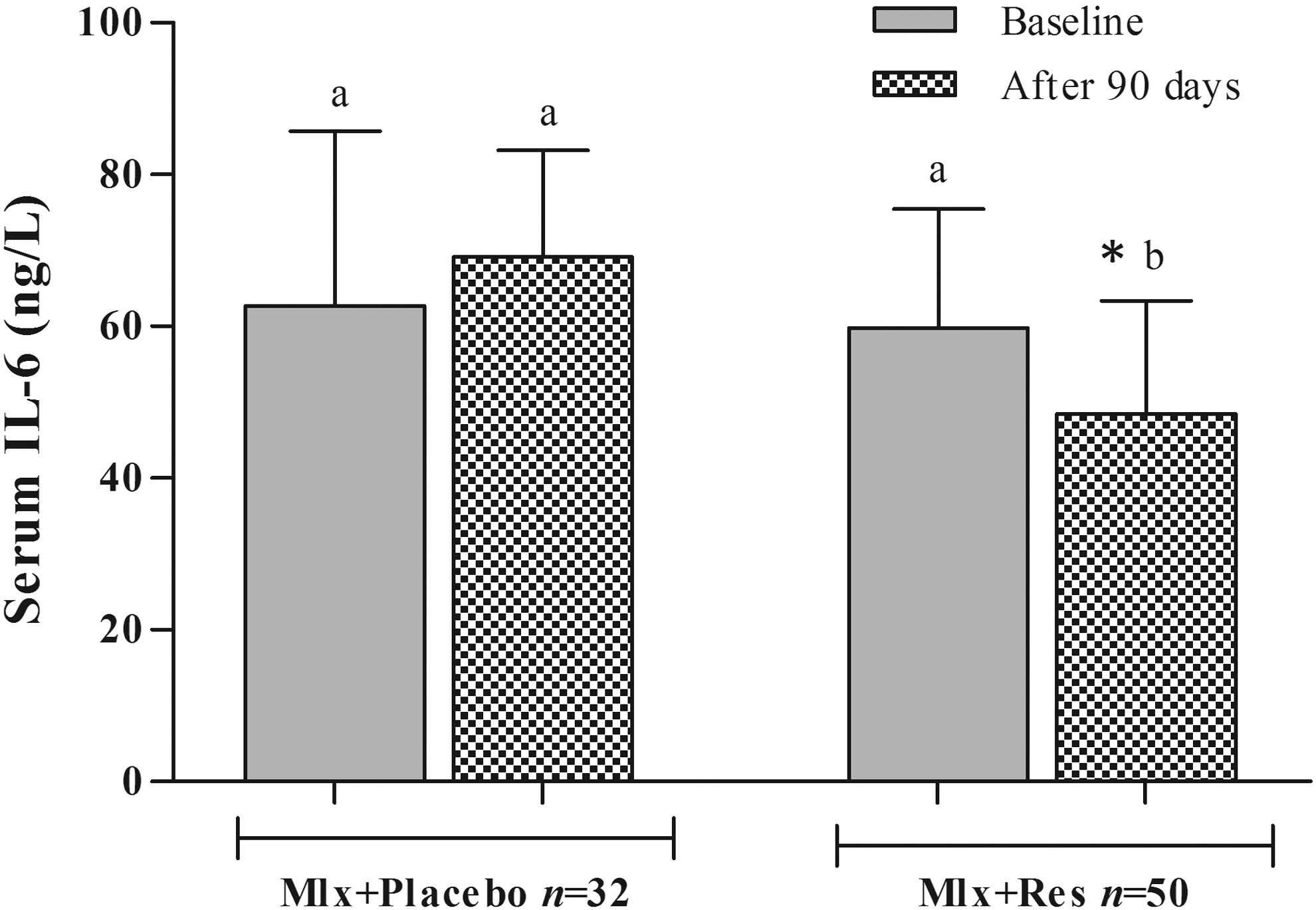
Effects of resveratrol, as adjuvant with meloxicam, on serum level of IL-6 in patients with mild to moderate knee OA. * represents significant difference compared with baseline value of the same group (P < .05); values with different letters (a, b) are significantly different among different groups (P < .05). IL, interleukin; OA, osteoarthritis.
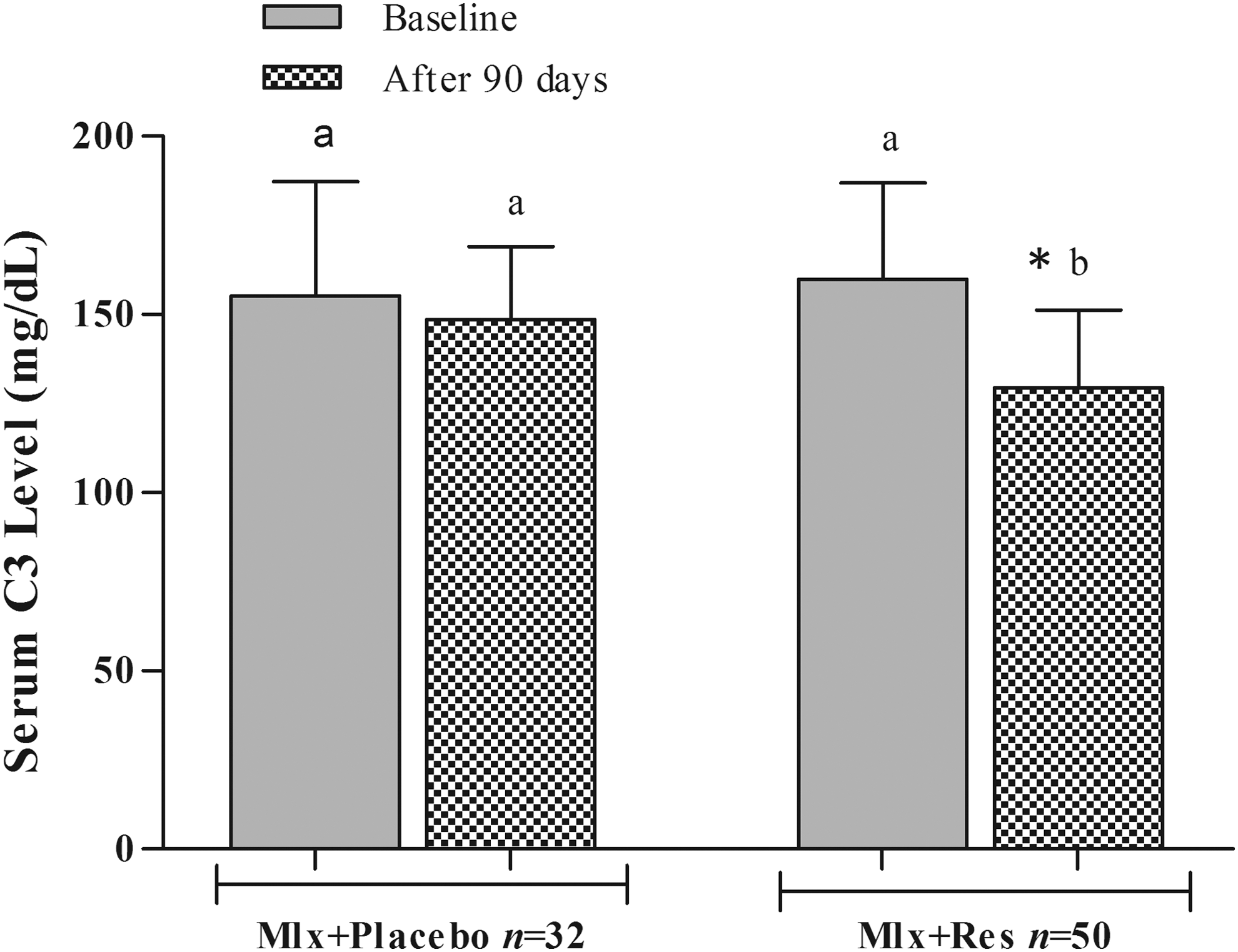
Effects of resveratrol, as adjuvant with meloxicam, on serum level of complement C3 in patients with mild to moderate knee OA. * represents significant difference compared with baseline value of the same group (P < .05); values with different letters (a, b) are significantly different among different groups (P < .05). OA, osteoarthritis.
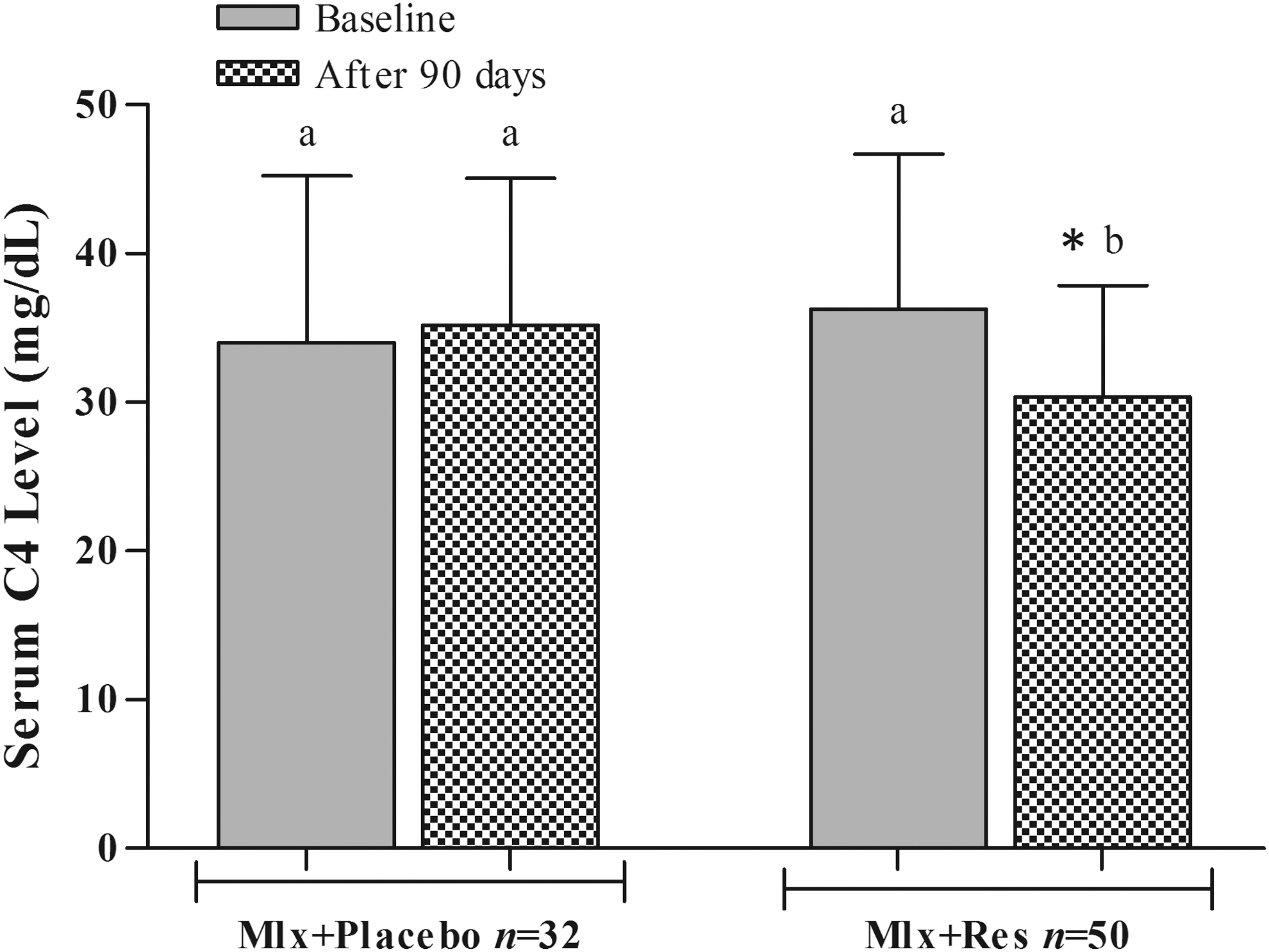
Effects of resveratrol, as adjuvant with meloxicam, on serum level of complement C4 in patients with mild to moderate knee OA. * represents significant difference compared with baseline value of the same group (P < .05); values with different letters (a, b) are significantly different among different groups (P < .05). OA, osteoarthritis.
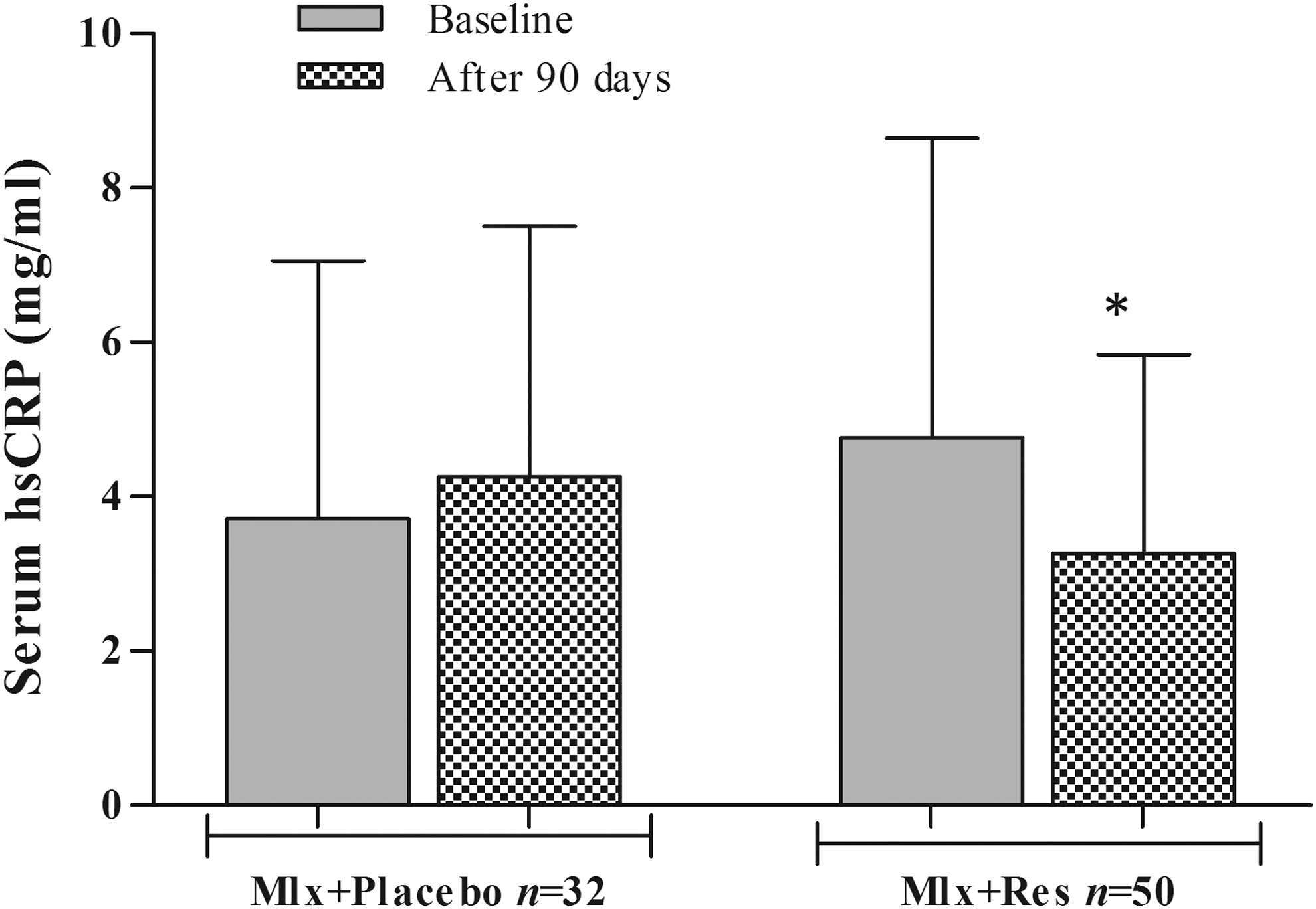
Effect of resveratrol, as adjuvant with meloxicam on serum level of hs-CRP in patients with mild to moderate knee OA. Values are presented as means ± SD; * represents significant difference compared with baseline value of the same group (P < .05); values with different letters (a, b) are significantly different among different groups (P < .05). hs-CRP, high-sensitivity C-reactive protein; OA, osteoarthritis.
Discussion
The principal findings of the present study were: (1) resveratrol 500 mg per day administered as adjuvant with meloxicam for 90 days reduced the pain severity in patients with mild to moderate radiological evidence of knee OA; (2) orally administered resveratrol at the mentioned doses significantly decreased serum levels of many inflammatory mediators such as TNF-α, IL-1β, IL-6, hsCRP, and complement proteins compared with placebo. The pharmacological effects of resveratrol have been well defined in various literatures. In addition to its well-recognized cardioprotective and neuroprotective roles, 20,21 the clinical benefits of resveratrol can be attributed to its antioxidant, antiapoptotic, and anti-inflammatory properties. 22,23 Accordingly, it can be considered as an effective “add-on” treatment and/or as an alternative to the currently used pharmacological agents for OA. The potential role of resveratrol in experimental animal models of OA was reported in rabbits, where resveratrol effectively attenuated collagenase-induced degradation of knee joint cartilage in this model. 24 To our knowledge, this study is the first pilot clinical trial that focuses on the effects of resveratrol on pain severity and inflammatory biomarkers of patients with mild to moderate knee OA. The orally administered resveratrol, as adjuvant with meloxicam, for 90 days led to a significant decrease in total pain score measured by VAS-100. Moreover, serum biomarkers of inflammation that accompany pain in knee OA, such as TNF-α, IL-1β, IL-6, and complement proteins, were shown to be significantly lowered in resveratrol-treated group compared with placebo. The presented data support the suggested role of many natural polyphenols, such as resveratrol, as a complementary treatment option in the management of pain and inflammation, the markers of disease progression in knee OA. Pain relief was considered a major goal of knee OA treatment, and OA-associated pain symptoms were correlated with the severity of inflammation, oxidative stress, and cartilage degradation. 25,26 Accordingly, it seems rational that supplementation with powerful antioxidants may be beneficial in this regard.
In the present study, the patients reported significant decreases in pain severity after 30 days of using resveratrol, reaching maximum improvement after 60 days compared with baseline according to VAS-100 scores. This finding is consistent with those reported by others who used other polyphenols such as curcumin and catechins, 11,27 which significantly decreased knee pain score in patients with similar intensity of pain as in our study. Moreover, the evidence that resveratrol has the ability to attenuate the production of COX-2 and PGE2 in the rat model of adjuvant arthritis might be the most convincing mechanism, among others, to explain its pain-relieving action. 28 Based on the strengths and limitations of the utilized pain assessment tool, the use of more than one tool is highly suggested to cover the multidimensional aspects of OA pain. However, the present findings highlight the need of larger trials to be validated.
Inflammatory processes were believed to play a pivotal role in the pathogenesis of knee OA. Moreover, many cytokines and inflammatory mediators, such as CRP, IL-1β, IL-6, and free radicals, are potentially involved in the pathogenesis of OA. 29 In experimental models of arthritis, resveratrol was found to significantly decrease serum levels of many inflammatory mediators, 30,31 but no previous clinical study had yet determined the effect of resveratrol on serum levels of inflammatory mediators in knee OA patients. In the present study, 90 days of treatment with resveratrol resulted in a significant decrease in serum levels of TNF-α, IL-1β, IL-6, and hs-CRP in knee OA patients, which seemed to be consistent with the anti-inflammatory effects of other dietary polyphenols in OA management. These clinical findings are consistent with data showing that blueberry and raspberry extracts lower pain, inflammation, and articular destruction in experimental arthritis, 32,33 and silymarin effectively ameliorated inflammation in patients with knee OA compared with meloxicam. 34
The present study has many limitations that may have affected interpretation and generalizability of its findings. These include a small number of patients and the lack of a dose–response protocol to evaluate larger doses of resveratrol. The included patients had mild to moderate radiographic knee OA at baseline (Kellgren–Lawrence scores <3) and relatively moderate knee pain. To know whether patients with more severe knee OA (Kellgren–Lawrence score 4) and severe pain would benefit from resveratrol intervention requires further investigation. Moreover, other markers of OA pathogenesis, such as indicators of oxidative damage, were not evaluated; in addition to that, the present study did not include assessments of these markers in the synovial fluid, which may provide more accurate determination of changes specific to knee OA. Additionally, we did not evaluate the radiological outcomes at the end of the trial.
The strengths of the present study include a randomized, placebo-controlled study design, which accounts for most of the variations in parallel-arm studies. Also, based on the treatment of a control group with a placebo formula that matched the resveratrol dosage form in sensory qualities, we were able to keep the patients and evaluators blinded to the identity of the test agents. Furthermore, we excluded knee OA patients who were taking any other kind of supplements, such as antioxidant vitamins, fish oil, and other herbal supplements for any purpose. In conclusion, this pilot study provides evidence of the role of resveratrol, administered as adjuvant with meloxicam, in improving pain and inflammation in patients with mild to moderate knee OA compared with placebo in the control group.
Footnotes
Acknowledgments
The data were abstracted from a PhD thesis submitted by B.H.M. to the College of Medicine, University of Sulaimani. The project was totally supported by the University of Sulaimani (certificate 42 in 21/11/2016). The authors gratefully thank the kind support from Shar Teaching Hospital and the Specialized Rheumatology Center in Sulaimani City.
Author Disclosure Statement
No competing financial interests exist.