
Abstract
Inflammatory bowel disease (IBD) is an umbrella term used to describe chronic inflammatory disorders related to a substantial reduction in the quality of life of patients. Some patients with Crohn's disease (CD) and ulcerative colitis (UC) are refractory to conventional therapies, and Curcuma longa derivatives have been considered as adjuvants. Owing to the anti-inflammatory and antioxidant effects, some clinical trials used this plant in the therapeutic approach of IBD, and some meta-analyses evaluated the outcomes found in these studies. Owing to controversial findings, our systematic review aimed to evaluate these studies to show whether C. longa compounds can still be considered in the therapeutic approach of patients with CD and UC. MEDLINE-PubMed, EMBASE, and Cochrane were searched, and Preferred Reporting Items for a Systematic Review and Meta-Analysis guidelines were followed. The results of the randomized clinical trials (RCTs) showed promising results with the use of curcumin in the therapeutic approach of both UC and CD patients. Some meta-analyses show controversial results, possibly due to the presence of bias in the included studies. The actions of curcumin are achieved by several mechanisms, such as reducing the expression of interleukin (IL)-1, IL-6, IL-12, and tumor necrosis factor-α. Moreover, it reduces the levels of reactive oxygen species, such as superoxide anions and malondialdehyde. The results of using curcumin in CD and UC patients are challenging to be evaluated because RCTs are variable in the dose and the formulations of curcumin, in the time of treatment, and the route of administration. The number of patients in the samples is also usually small.
Introduction
Inflammatory bowel diseases (IBDs) are a set of immune-mediated gastroenterological diseases that are majorly represented by ulcerative colitis (UC) and Crohn's disease (CD). In North America, the incidence rates for UC vary between 2.2 and 19.2 cases per 100,000 person-years, and for CD the incidence rates range from 3.1 and 20.2 cases per 100,000 person-years. 1,2
Both UC and CD are chronic, debilitating, remitting, and relapsing inflammatory processes that occur due to a disruption in the immune response to intestinal microorganisms or other environmental conditions, leading to an imbalance between pro- and anti-inflammatory mediators. 3,4
There are some possibilities to treat IBDs, but many patients may be refractory to these therapies. 5 Moreover, since they are associated with high costs and may produce severe adverse effects, specialists have considered the use of Curcuma longa or its primary derivative (curcumin) as an alternative therapeutic approach. 6,7
Curcumin is a polyphenol with immunosuppressive and antioxidant properties. It is associated with suppression of nuclear factor-kappa B (NF-κB) in B-lymphocytes, and downregulation in the production of tumor necrosis factor-α (TNF-α), interferon-γ (IFN-γ), interleukin-1β (IL-1β), IL-6, IL-12, and IL-17 (Refs. 8 –10 ). This compound has shown unique anti-inflammatory activities and ability to modulate gut microbiota as shown in a meta-analysis with irritable bowel syndrome. 11
Owing to the anti-inflammatory and antioxidant effects attributed to C. longa compounds, some clinical trials used this plant in the therapeutic approach of IBD and some meta-analyses evaluated the outcomes found in these studies. Owing to controversial findings, our systematic review aimed to evaluate these studies to show whether C. longa compounds can still be considered in the therapeutic approach of patients with CD and UC.
Methods
Focused question
This review was performed to answer the focused question: Can Curcuma longa induce clinical and endoscopic remission on Crohn's disease and ulcerative colitis?
Language
Only studies in English were selected.
Databases
This systematic review has included studies published in MEDLINE–PubMed (National Library of Medicine, National Institutes of Health), EMBASE, and Cochrane databases. The descriptors were “Curcumin or Curcuminoids or Curcuma longa and Inflammatory Bowel Diseases or Ulcerative Colitis or Crohn's Disease.” The use of these descriptors helped us to identify randomized clinical trials (RCTs) related to the use of curcumin and its effects on UC and CD patients. We followed PRISMA guidelines (Preferred Reporting Items for a Systematic Review and Meta-Analysis) to perform the search.
Study selection
The inclusion criteria were RCTs, primary, and interventional studies, and the exclusion criteria were reviews, studies not in English, editorials, and case reports.
Eligible criteria
The eligible criteria for this systematic review followed the PICO (population, intervention, comparison, and outcomes) format, and the studies involving IBD patients who were treated with curcumin were included.
Data extraction
Two independent judges, R.A.G. and S.M.B., independently performed the search to identify the RCTs in the databases. The MESH terms were Curcuma longa, curcumin, inflammatory bowel diseases, ulcerative colitis, and Crohn's disease. The abstracts of the studies were evaluated, and full-text articles (with only one exception) were also evaluated to support the decision-making process. Disagreements between the judges were evaluated and decided by other reviewers (E.L.G. and A.C.A.). Our research included studies published from January 2006 to June 2020.
Results
The flow diagram in Figure 1 shows the selection of the articles, as well as the included studies (this diagram followed PRISMA guidelines 12 ). Eight RCTs were selected to build this review (Table 1). Among these studies, one was an open-label trial, and seven were RCTs. Altogether, 750 individuals were enrolled in the selected studies, age 18–65 years old (259 men; 461 women; in one study, we did not identify the gender (n = 30). Table 2 gives the bias risk assessment for the included studies.
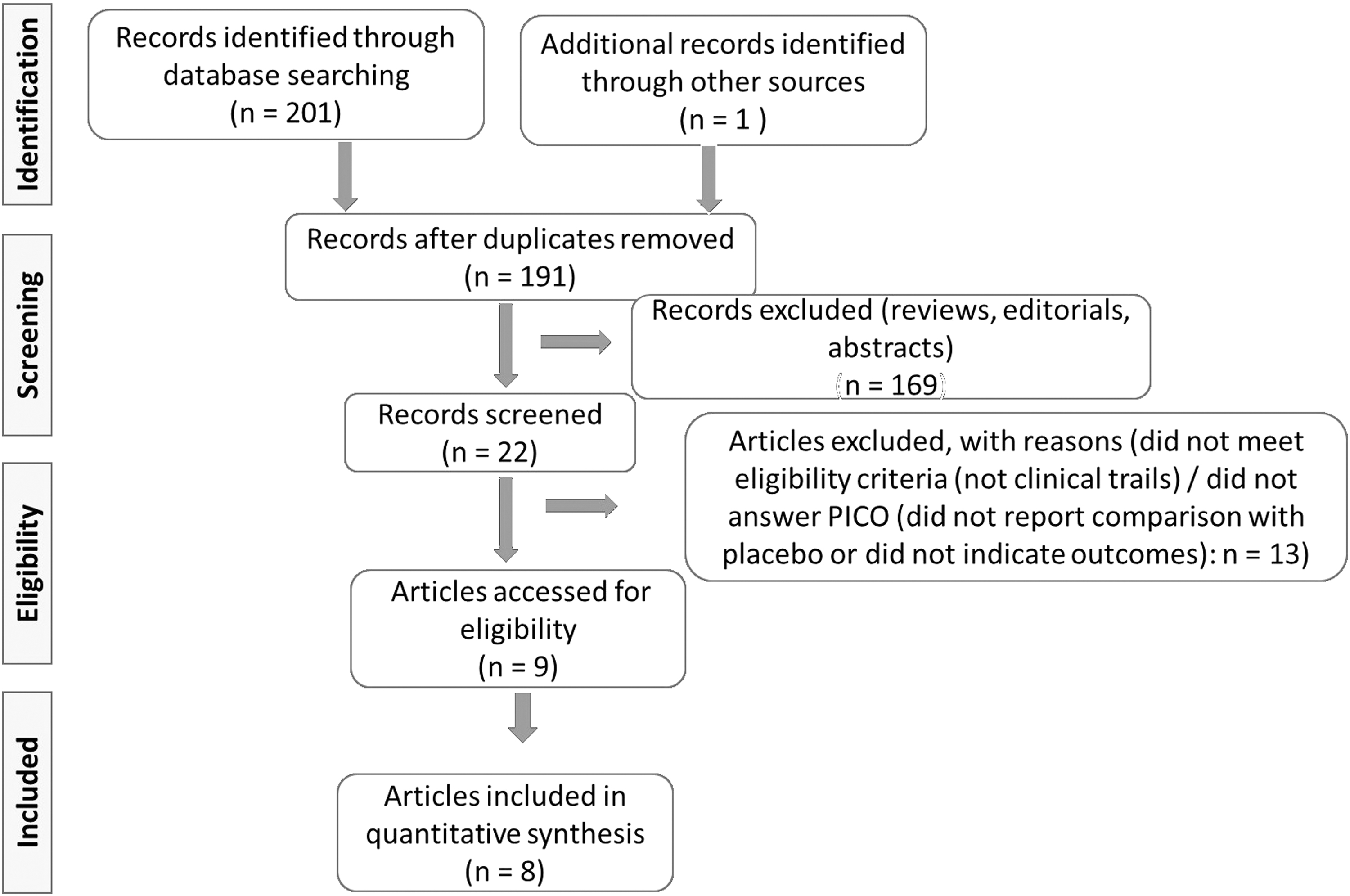
Flow diagram showing the study selection. PICO, population, intervention, comparison, and outcomes.
Randomized Clinical Trials That Evaluated the Effects of Curcuma longa in the Inflammatory Bowel Diseases
5-ASA, 5-aminosalicylate; CAI, clinical activity index; CD, Crohn's disease; EI, endoscopic index; ESR, erythrocyte sedimentation rate; hs-CRP, high-sensitivity C-reactive protein; NCB-02, a standardized extract of Curcuma longa with a composition of 72% curcumin, 18.08% demethoxy curcumin and 9.42% bis-demethoxy curcumin; SCCAI, simple clinical colitis activity index; SMEDDS, novel self-micro emulsifying drug delivery system; UC, ulcerative colitis; UCDAI, ulcerative colitis disease activity index.
Descriptive Table of the Biases of the Included Randomized Clinical Trials
NR, not reported.
Discussion
IBDs: main pathophysiological aspects
Genetic, environmental, and immunological factors, mainly associated with intestinal microbiota unbalance, are considered at the onset of IBD. In the homeostasis, the immune system can prevent the increase of harmful bacteria that could penetrate the lamina propria, and at the same time can tolerate the commensal microorganism. Disruption in this balance can result in the increase of harmful bacteria in the intestine and lead to abnormal inflammatory response. 13,14
Among the numerous genetic factors and gene loci related to the development of IBD, studies have shown that changes in alleles of genes that are responsible for surface proteins and receptors of immune cells, such as monocytes, lymphocytes, and macrophages, are related to the production and activation of proinflammatory factors such as TNF-α, IFN-γ, IL-1β, IL-6, and IL-12 (Refs. 15 –17 ).
Environmental factors are directly linked to modern Western dietary habits and lifestyle. IBD prevalence is known to be higher in industrialized Western countries, and some studies attribute this to the higher intake of xenobiotics present in industrialized foods and condiments instead of a healthier diet, including fruits, vegetables, and fibers. Nevertheless, other lifestyle habits are included as factors on the development of IBD, such as smoking, alcohol consumption, and elevated sugar intake, once these are related to promoting an exacerbated inflammatory response, oxidative stress, and disruption of the epithelial barrier. Moreover, the indiscriminate use of drugs, especially antibiotics, which can alter the intestinal microbiome and enable dysbiosis, can also be associated (Fig. 2). 14,18 –21
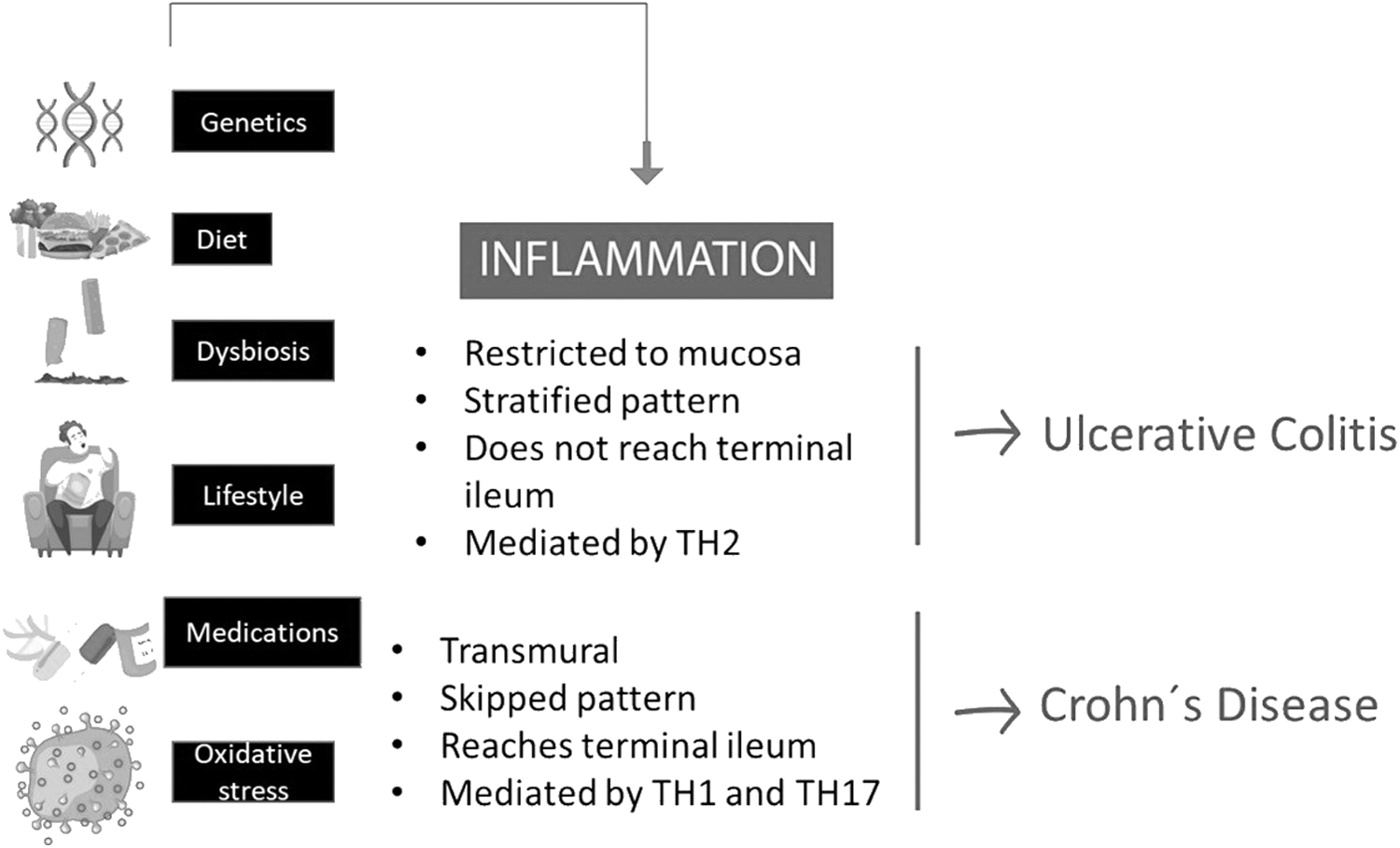
Possible causes of IBDs and some differences between UC and CD. CD, Crohn's disease; IBDs, inflammatory bowel diseases; TH, T helper cell; UC, ulcerative colitis.
Dysbiosis is an unbalance between the commensal microbiota and pathological microorganisms. It is known that a well-balanced relationship between the different kinds of bacteria, fungi, and viruses in the intestines diminishes the occurrence of inflammation and IBD. Pathogenic microorganisms stimulate immune responses that can be exacerbated when other predisposing factors are present. 22,23
The augmented permeability to luminal antigen contributes to the massive immune response (Fig. 3). Antigens are related to the activation of dendritic cells (DCs), macrophages, and NF-κB leading to excessive production of proinflammatory cytokines. Beyond that, desmosomes, tight junctions and adherens junctions from the intestinal epithelial barrier, also seem to play an important role in IBD pathogenesis. 24,25
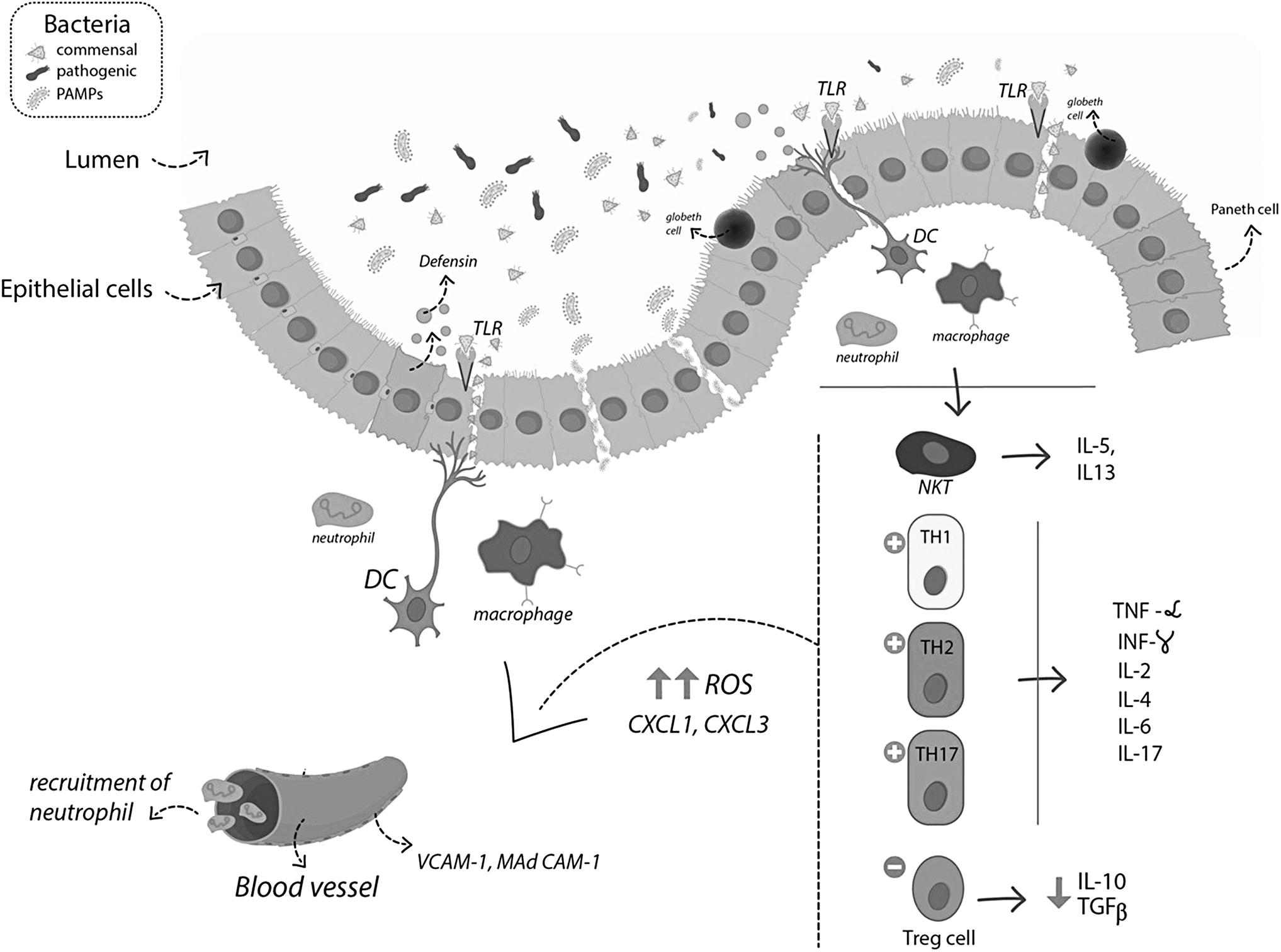
Pathophysiologic aspects of IBDs. The disruption in the mucinous layer and loss of tolerance to microbiota increase the permeability and leads to an abnormal inflammatory response. The main processes are mediated by the upregulation of TH1, TH2, and TH17, resulting in the increased release of TNF-α, IFN-γ, IL-2, IL-6, and IL-17. DCs, dendritic cells; IFN-γ, interferon gamma; IL, interleukin; MAdCAM-1, mucosal addressin cell adhesion molecule 1; NKT, natural killer T cells; PAMPS, pathogen-associated molecular pattern; ROS, reactive oxygen species; TNF-α, tumor necrosis factor-alpha; VCAM-1, vascular cell adhesion protein 1.
CD and UC present significant differences, especially in the pathophysiology and inflammation patterns. CD is characterized by intramural lesions that can occur in any part of the gastrointestinal tract, from mouth to anus. Lesions in CD can be discontinuous, showing skipped areas of healthy and inflamed tissues. Furthermore, the inflammatory process is mainly mediated by TH1 and TH17 cells. In contrast, UC is a typically hemorrhagic disease that affects the mucosal layer of the large intestine, especially the rectum and the terminal segments of the colon. Unlike CD, UC lesions show no skipped areas (Fig. 2). The inflammatory response in UC is mediated mainly by a TH2 response, with an ulcerative pattern. Clinically, both diseases cause abdominal pain, diarrhea, vomiting, and bloody stools that are related to the worsening of the patient's quality of life and lead to incapacity for work or social life. 26,27
Curcumin
The genus Curcuma, belonging to the Zingiberaceae family, consists of a group of perennial rhizomes, native and widely cultivated mainly in Asia and other tropical and subtropical regions such as South America and Australia. Almost 500 chemical compounds have already been identified from Curcuma spp. The genus is rich in compounds such as flavonoids, tannins, anthocyanin, phenolic compounds, organic acids, and inorganic compounds. Among Curcuma spp., C. longa stands out. It is known worldwide as saffron or turmeric and is widely used in alternative medicine since ancient times due to its beneficial actions in the treatment of respiratory, gynecological, urinary, and gastrointestinal disorders. Besides, its effects are related to antirheumatic actions, improvement of metabolic profile, antihypertensive, antimicrobial, neuroprotective, antioxidant, and anti-inflammatory effects. 28 –30
The main compounds are curcuminoids (curcumin, demethoxycurcumin, and bisdemethoxycurcumin) that are nontoxic polyphenolic components to which several biological actions are attributed. Curcumin (diferuloylmethane) is the major and one of the main active ingredients that gives turmeric a potent anti-inflammatory and antioxidant potential. 31,32
C. longa and IBD
Curcumin exerts anti-inflammatory and antioxidant effects by different mechanisms of action. Studies have indicated that pretreatment with this compound suppresses lipopolysaccharide-induced NF-κB p65 translocation and mitogen-activated protein kinase phosphorylation in DCs, leading to a reduction in inflammation. It also reduces the expression of IL-1, IL-6, IL-12, and TNF-α, inhibiting the ability of DCs to induce TH1-type responses. An essential action of curcumin on DCs is the suppression of indoleamine 2,3-dioxygenase, with an anti-inflammatory effect similar to corticosteroids. Curcumin can block the stimulation of TH1 subset by suppressing macrophage activation, and can also inhibit the activation of TH17, reducing the production of proinflammatory cytokines such as IL-6, IL-21, and IL-17. The cyclooxygenase-2 (COX-2), an inflammatory enzyme induced by NF-κB and activator protein 1 (AP-1) signaling, is an essential mediator in prostaglandin synthesis, and it is known to be upregulated in IBD. In BV2 microglial cells, curcumin treatment abrogated COX-2 gene expression through the reduction of both AP-1 and NF-κB signaling. Furthermore, curcumin can also inhibit the receptors for COX-2. In summary, curcumin can downregulate the production of TNF-α, IFN-γ, IL-1, IL-2, IL-6, and IL-8, while elevates IL-10 and transforming growth factor-β, promoting a crucial anti-inflammatory action. 33 –36
Authors have shown that oxidative stress plays a pathogenic role in s. Physiological levels of nitric oxide (NO) protect the intestinal mucosa, but increasing amounts of NO produced through inducible nitric oxide synthase, and potentially endothelial nitric oxide synthase, can lead to tissue injury and necrosis. The imbalance of reactive oxygen species (ROS) and reactive nitrogen species can lead to the peroxidation of membrane lipids, DNA damage, and the denaturing of cellular proteins. Curcumin reduces the levels of ROS, such as NO, superoxide anions, and malondialdehyde. Myeloperoxidase (MPO), which is a component of monocyte and neutrophil granules, produces high levels of ROS, and curcumin has been shown to decrease intestinal inflammatory disease associated with MPO activity. Moreover, curcumin increases the levels of free radical-scavenging superoxide dismutase. It can upregulate phase II enzymes related to the metabolism and detoxification of xenobiotics, as well as additional antioxidant proteins, such as nuclear factor (erythroid-derived 2)-related factor (Nrf2), a transcription factor working as a crucial regulator of antioxidant proteins, and heme oxygenase-1, a redox-sensitive stress-induced protein, capable of degrading heme to iron, biliverdin, and carbon monoxide. Curcumin also provides a protective effect against hydrogen peroxide-induced tight junction disruption, and the associated increase in paracellular permeability. 34,37 –41 Figure 4 shows a summary of the effects of curcumin in IBDs.
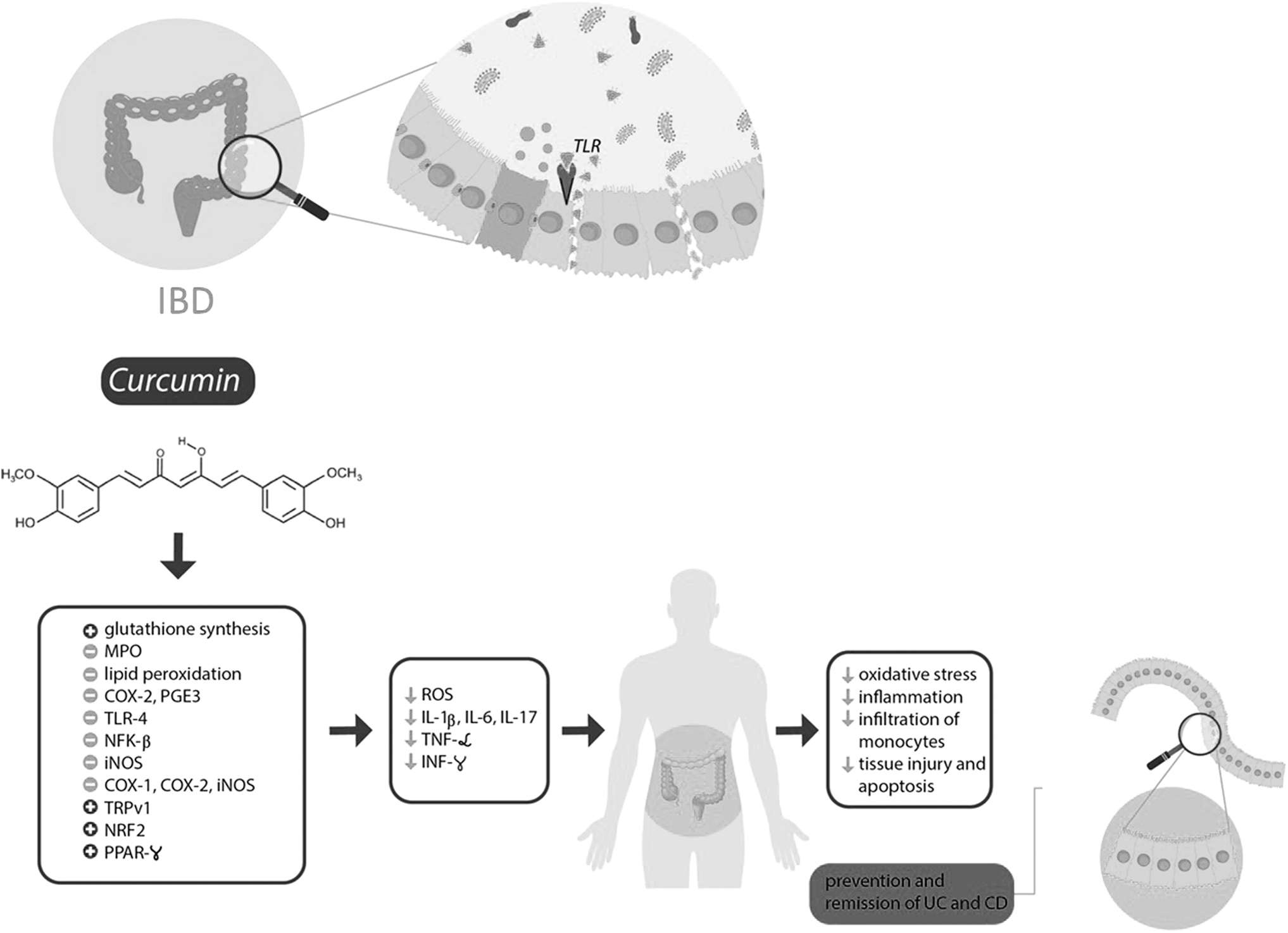
Effects of Curcuma longa in bowel inflammatory process. COX-2, cyclooxygenase 2; iNOS, inducible nitric oxide synthase; MPO, myeloperoxidase; Nrf2, nuclear-related factor 2; PGE3, prostaglandin E3; PPARγ, peroxisome proliferator-activated receptor gamma; TLR-4, toll-like receptor 4; TRPV1, transient receptor potential vanilloid type 1.
Curcumin also has the ability to inhibit the growth of Helicobacter pylori. In addition, curcumin favors the production of short-chain fatty acids that present anti-inflammatory properties. 36,42 –45
The use of curcumin in humans
We found only one RCT that evaluated the use of C. longa in the therapeutic approach of CD, but some interesting studies have also shown the effects of this plant in patients with mild-to-moderate UC. Most of them used curcumin orally (six studies), and one study used an enema. These studies are summarized in Table 1 and discussed hereunder.
Sugimoto et al. 46 performed the first and unique study using curcumin in the therapeutic approach of CD. In this RCT, authors evaluated patients from five medical centers (Japan) and used a formulation named Theracurmin® in patients with active mild-to-moderate CD for 2 months. They evaluated the efficacy of the formulation through clinical and endoscopic parameters, healing of anal lesions, and serum levels of inflammatory biomarkers. Theracurmin is considered to exhibit a rate of 27-fold higher absorption than natural curcumin powder. The results of the study showed that this formulation resulted in significant clinical and endoscopic improvement (the rates of endoscopic remission were 15% for the treated group and 0% in the placebo group, and clinical remission was significantly higher in the curcumin group). Furthermore, serious adverse effects were reported, indicating that Theracurmin has a safety profile.
Sadeghi et al. 2 performed an RCT with UC patients with active symptoms of the disease. Patients in the curcumin group significantly achieved remission, Simple Clinical Colitis Activity Index (SCCAI) scores ≤2, and improvement of the disease, which was defined by a decrease of ≥3 in SCCAI score, and the mean difference of the IBD Questionnaire-9 score increased significantly in the curcumin group compared with the placebo group. Although the authors have shown promising results with the use of curcumin to induce remission in UC patients, a possible bias in this study is that it is not clear what were the conventional medications or doses used by patients.
The RCT performed by Masoodi et al. 47 included UC patients treated with curcumin nanomicelles due to the better bioavailability of this preparation. Although there was a clinical improvement in patients in the treated group, there was no evaluation of laboratory parameters such as hemoglobin, erythrocyte sedimentation rate, C-reactive protein, liver function tests, and stool calprotectin.
Kedia et al. 48 did not show the effectiveness of using oral curcumin at a dose of 450 mg daily in inducing clinical remission, clinical response, and mucosal healing in UC patients. Furthermore, the authors concluded that remission was not achieved possibly due to the small dose of curcumin, which constitutes a potential bias in this study.
The study by Banerjee et al. 49 evaluated the properties of curcumin in improving clinical response (reduction of ≥3 points of Partial Mayo score) and endoscopic remission (Partial Mayo score ≤1) in patients with active mild-to-moderate UC. Curcumin group received SMEDDS, a self-micro emulsifying drug delivery system. The authors showed that the association of bioenhanced curcumin with mesalamine appears to be effective in inducing remission and requires smaller doses of curcumin. The patients were evaluated after 6 weeks and 3 months, and clinical improvement in the curcumin group was significant in the two moments.
The results of the study performed by Lang et al. 50 indicated that the administration of curcumin is more effective than placebo in achieving clinical and endoscopic remission. Treatment optimization included the administering of oral 5-ASA concomitantly with topical 5-ASA enema or suppository. This variability in the form of topical administration of the medication is a possible bias. The short time of administration should also be considered.
The study of Singla et al. 51 evaluated the effects of NCB-02, a standardized C. longa extract containing 72% curcumin, 18.08% dimethoxy curcumin, and 9.42% bis-dimethoxy curcumin, in patients with UC. The results showed that the use of NCB-02 with oral 5-ASA is significantly better than only 5-ASA and placebo in achieving clinical response. Many patients left the study before eight weeks, which leads to a relevant bias in the analysis of results.
The RCT performed by Hanai et al. 52 evaluated the effects of curcumin in clinical improvement in patients with quiescent UC using criteria such as clinical activity index and endoscopic index. A relevant bias in this study is that authors evaluated the effects of curcumin in patients without active disease.
Since studies began to show the promising effects of C. longa and its bioactive compounds on different inflammatory diseases, many researchers have published RCTs and meta-analysis that related to the effects of this plant to IBDs.
Simadibrata et al. 53 included in their meta-analysis three studies 50 –52 and 185 patients. However, two studies included the oral intake of curcumin, and one study included enema. Furthermore, the study by Hanai et al. 52 was performed in patients in remission (outcomes and side effects are different when comparing patients with active disease). The results of this study showed that curcumin was more effective than placebo in both patients with active mild-to-moderate UC or stable patients, and can improve clinical and endoscopic outcomes. Despite the promising results, different routes of administration and different phases of the disease represent a relevant bias in the inclusion of the studies in this meta-analysis.
Iqbal et al. 54 also meta-analyzed the effects of curcumin in IBDs and included the RCTs performed by Lang et al., 50 Singla et al., 51 and Banerjee et al., 49 totaling 143 patients. The results showed that curcumin produces higher odds of clinical and endoscopic remission. Similar to the meta-analysis of Simadibrata et al., 53 these authors also included studies using oral curcumin and enema. Furthermore, they related that curcumin associated with conventional therapy could prevent relapse; however, except for Banerjee et al., 49 the duration of the treatment was not sufficient to make this statement.
Another meta-analysis conducted by Grammatikopoulou et al. 55 included 187 patients from the studies of Hanai et al., 52 Lang et al., 50 and Kedia et al. 48 The bias of this study is the inclusion of the study performed by Hanai et al., 52 which, as already mentioned, included patients in remission from UC. Unlike Simadibrata et al. 53 and Iqbal et al., 54 the results of this review suggested that curcumin does not contribute to the achievement of remission in UC patients.
The meta-analysis of Zheng et al. 56 presents relevant biases. They included the studies of Hanai et al., 52 Kedia et al., 48 Lang et al., 50 Singla et al., 51 Banerjee et al., 49 and Masoodi et al. 47 The authors used odds ratio analysis, which is not appropriate for retrospective case–control studies (the use of a risk assessment would fit). They also included RCTs that involved curcumin orally and enema.
Chandan et al. 7 published a very recent meta-analysis with the inclusion of 380 UC patients distributed in seven studies (Hanai et al., 52 Singla et al., 51 Kedia et al., 48 Lang et al., 50 Masoodi et al., 47 Banerjee et al., 49 and Shivakumar et al. 57 ). Similar to the meta-analysis already mentioned, the authors have involved studies performing different administration routes (such as Singla et al. 51 that used enema curcumin and other studies that used oral curcumin), and different phases of the disease (as an example, Hanai et al. 52 included patients in remission). Besides that, they concluded that curcumin, combined with mesalamine, leads to superior clinical and/or endoscopic response in the patients, although with heterogeneity. For these reasons, the authors recommend curcumin as an adjunct to mesalamine in the therapeutic approach of UC.
In general, the results of the RCTs evaluated in our systematic review are promising with the use of curcumin in the therapeutic approach of patients with IBD. Meta-analysis shows controversial results, possibly due to the presence of bias in the inclusion of the studies for the statistical analysis. We cannot fail to mention that the results of using curcumin are challenging to be evaluated because RCTs are very variable in the dose and type of formulations of curcumin, in the time of treatment, and the route of administration. The number of patients in the samples is also usually small.
Conclusion
The number of IBD patients has been rising and affects relatively young ages, disabling the patient from studying or working, and leading to a profound impact on the quality of life. Beyond that, some patients are refractory to conventional therapies. Although studies are showing exciting results and new perspectives surrounding curcumin as adjuvant therapies for UC and CD, it is necessary to establish appropriate dosages, curcumin formulation, and administration routes to enhance the effects of these therapies. Although curcumin looks promising in the treatment of intestinal inflammatory diseases, further controlled clinical trials are needed.
Footnotes
Acknowledgment
We thank Renato Vono for drawing the figures.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.