
Abstract
This clinical study aimed to assess the effectiveness and safety of Vuong Hoat (VH) natural health supplement for reducing the negative impact of low back pain, improving the quality of life, and enhancing functional activities in patients with lumbar degenerative disc disease (LDD). The open-label, randomized, controlled clinical trial involved 60 patients suffering from low back pain caused by LDD. The participants were randomly assigned to either a study group (SG) comprising 30 subjects or a control group (CG) comprising 30 subjects. Patients in the CG received treatment with electro-acupuncture, while those in the SG were administered VH in conjunction with the same electro-acupuncture protocol for 28 days. The clinical progression and tolerability of both groups were compared based on seven objective measurements: visual analog scale index, Schober test, fingertip-to-floor distance, spinal flexion, spinal extension, spinal tilt, and spinal rotation. After 14 days of treatment, the SG showed a significant improvement in overall outcomes compared to the CG. Specifically, 43.3% of SG patients achieved very good results, 53.3% had good results, and 3.4% had moderate results, whereas corresponding figures for the CG were 6.7%, 76.7%, and 16.6%, respectively (P < .05). After 28 days of treatment, both groups demonstrated a shift toward very good results, with the SG continuing to show better outcomes than the CG (P < .05). In the SG, the very good results increased to 76.7%, good results decreased to 20%, and moderate results were 3.3%. On the other hand, the CG had 46.7% very good results, 43.3% good results, and 10% moderate results. Notably, no side effects were reported from the VH treatments during the study. The findings of this study indicate that VH health supplement is a safe and effective approach for managing low back pain and limited spinal movement in patients with LDD.
INTRODUCTION
Lumbar degenerative disc disease (LDD) is a prominent cause of chronic low back pain and a leading contributor to disability/lost workdays worldwide. LDD may present as disc herniation, lumbar spinal stenosis, facet joint arthropathy, or a combination of these conditions. The prime symptoms of LDD include lower back pain and sciatica, which may intensify by standing, walking, bending, straining, and coughing. 1 –5 Although lumbar degeneration can occur at any level of the spine, it predominately affects the L3-L4 and L4-S1 vertebrae. 6 Sciatica presents as unilateral or bilateral leg pain radiating to the feet and toes, often accompanied by numbness and a positive straight leg raising test. 7 Sensory disturbances in the legs, claudication, pain relief when bending forward, and weakness are also observed as symptoms of LDD. 8
Notably, LDD is becoming more prevalent among younger individuals, with a rising number of cases reported in people in their 30s, whereas it was previously more common in those over 50 years old. The economic impact of diagnosing and managing lumbar spine diseases and back pain in the United States is substantial, reaching up to 100 billion USD annually. 4,9 The burden of recurrent low back pain is significant at both the individual and societal levels. 10,11 Over the past three decades, there has been a notable increase in the demand for chronic low back pain treatment. Studies utilizing national and insurance databases have highlighted the greater utilization of spinal anti-inflammatory injections, surgery, and opioid medications to manage low back pain in individuals with LDD. 12 –16 In addition, there has been a documented rise in prescriptions for analgesic medications and visits to health care providers, physical therapists, and chiropractors for low back pain management. 14,17
The optimal management of LDD involves addressing the root cause of pain and tailoring treatment based on individual patient needs. 18,19 However, long-term use of nonsteroidal anti-inflammatory drugs in patients with LDD can lead to severe complications, including stomach ulcers, hepatic failure, cardiovascular issues, and undesirable effects such as nausea, constipation, bleeding, and the risk of drug dependency. 20,21
Vuong Hoat (VH) is a registered health supplement with ingredients of herbal extracts and nutritional agents, including Commiphora myrrha, Morinda citrifolia extract, Homalomena occulta extract, Salix alba’s bark extract, along with copper gluconate and methylsulfonylmethane. Previous traditional herbal therapy experiences and published studies have suggested that VH’s ingredients may reduce the risk of degenerative spine conditions, spondylosis symptoms, disc herniation, back pain, neck pain, and shoulder pain, while enhancing mobility in individuals with osteoarthritis, particularly those affecting the spine. These ingredients also support slowing down the degenerative process of the spine and disc herniation and may be beneficial in managing pain, inflammation, and LDD. 22 –29
VH has received the Certificate of Conformity with Food Safety Regulations from the Food Safety Department of the Vietnamese Health Ministry. It has undergone evaluation for acute toxicity at the National Institute of Drug Quality Control and chronic toxicity assessment at Hanoi Medical University, demonstrating its safety for human use.
The current study aims to assess the efficacy and tolerability of VH in patients with low back pain induced by LDD, with specific objectives: (i) To evaluate the clinical effectiveness of VH in treating patients with low back pain induced by LDD. (ii) To investigate any undesirable effects of VH on clinical and paraclinical parameters. By examining the effectiveness and safety of VH in managing LDD-related low back pain, this research seeks to provide valuable insights into a potentially promising treatment option for this debilitating condition.
MATERIALS AND METHODS
Material for the study
VH health supplement tablets are registered with the Department of Food Safety and Hygiene—Ministry of Health under registration number 5445/2020DKSP. The product is distributed by Fobic Pharmaceutical LTD, based in Hanoi, Vietnam. The specific research lot, with lot number 011221, was manufactured on 10/12/2021, and its expiration date is 09/12/2024. To ensure the quality and safety of the product, the research lot underwent testing by the Testing Center at the Vietnam Institute of Dietary Supplements. This thorough testing process aims to guarantee that the health supplement tablets meet the required standards and are safe for consumption by users.
Place and time of study
The study was conducted at the Tue Tinh Hospital—Viet Nam University of Traditional Medicine, Hanoi, Vietnam. The research period was from January 2022 to December 2022.
Research subjects
The research included patients diagnosed with low back pain due to LDD who met specific criteria.
The inclusion criteria were as follows: Age: From 38 to 70 years old, regardless of gender and occupation. Patients with a history and symptoms of LDD. Clinical manifestations of pain in the lumbar spine area, limited lumbar spine movement, and visual analog scale (VAS) score <7. X-ray shows one of the images of degeneration, joint space narrowing, bone thickening, bone bridge, spina bifida (double spine), lumbar fusion, and lumbar spine displacement. Patients who voluntarily participated in the study and complied with the treatment protocol.
The exclusion criteria were as follows: Low back pain accompanied by infection and systemic diseases. Patients with ankylosing spondylitis, spinal tuberculosis, primary and secondary cancer, and vertebral fracture. Patients with heart failure, liver failure, kidney failure, and blood clotting disorder. Patients suffering from inflammation or gastric ulcer. Patients who are sensitive to the ingredients of the product. Patients who did not voluntarily participate in the study or complete the pretreatment tests. Pregnant or lactating women.
Sample size
Sixty patients who met the research sample selection criteria mentioned above were randomized into two groups: the study group (SG) and the control group (CG). Thirty patients in the SG were treated with VH tablets combined with electro-acupuncture. Thirty patients in the CG were treated with electro-acupuncture alone (acupuncture point protocols are the same as the SG).
Dosage and usage of VH tablets in the study
The VH tablets were administered to the SG as follows: During the first 14 days: two times a day, three tablets each time, 1 h after meals in the morning and afternoon. From the 15th to the 28th day for maintenance doses: two times a day, two tablets, 1 h after meals in the morning and afternoon.
Data processing method
Data were processed using IBM SPSS Statistics 25.0 software. Algorithms used in the study include chi-squared, percentage calculation, and t-test. Statistical significance was determined with P < .05.
Research ethics
Before the study, patients were provided with consultation and gave informed consent to participate. Patients had the right to withdraw from the study at any time without providing specific reasons. The study protocol BVTT-BCNTDT-08 was approved by the Scientific Research Council, the Ethics Committee of Tue Tinh Hospital-Vietnamese University of Traditional Medicine, and the Ethical Council of the Vietnamese Institute of Dietary Supplement.
The pain level on a VAS
The patient’s pain level was assessed on a VAS ranging from 0 to 10, where 0 presents no pain, and 10 presents the worst pain one could imaginable. Prior to the assessment, the patient was in a rested state and not exposed to any external stimuli. The pain assessment method was explained to the patient using five icons representing different pain levels, allowing the patient to indicate their perceived pain level. The patients’ pain ratings were then categorized into a point system.
Measurement of lumbar spine dilation (Schober test)
To evaluate lumbar spine flexibility, each patient was asked to stand upright with their heels close together and their feet open at an angle of 60°. Two marks were placed on the patient’s back, one at the superior edge of the S1 vertebrae and the other 10 cm above it. The distance between these two marks was measured again when the patient was instructed to bend down as far as possible. This measurement allowed the assessment of the discrepancy between the two positions, representing the lumbar spine elongation. A normal distance of 4–5 cm is typically expected in this test (31). The patients’ lumbar spine elongation was evaluated using a point system.
Fingertip-to-floor test
The fingertip-to-floor test involved measuring the distance from the patient’s fingers to the ground while standing upright with feet parallel to each other and slowly bending down. A normal fingertip-to-floor distance for healthy individuals is d ≤ 10 cm. 30 The patient’s lumbar spine elongation was rated into a point system.
Lumbar spine range of motion assessment
The assessment of the lumbar spine range of motion included four components: flexion of the spine, extension of the spine, spine tilt, and spinal rotation. The point system was used to evaluate the patient’s performance in these movements (33–36).
Evaluation of the overall outcome of the treatment
The overall outcome of the treatment was evaluated based on the total score of seven objective measurements, which included the VAS score, Schober test results, Fingertip-to-floor distance, Spinal flexion, Spinal extension, Spinal tilt, and Spinal rotation. The treatment results were rated according to the percentage of reduction in clinical symptoms: more than 80% improvement was categorized as “very good,” 60–80% improvement as “good,” 40–60% improvement as “moderate,” and less than 40% improvement as “poor.” This scoring system helped assess the overall effectiveness of the treatment in managing the patient’s condition.
RESULTS
General characteristics of the study subjects
The mean age of the SG was 59.23 ± 9.47, and in the CG was 61.17 ± 8.44. The gender ratio in both groups was relatively equivalent, with 51.7% of males and 48.3% of females. In terms of occupation, both SG and CG had a higher rate of individuals engaged in intensive physical labor (55%) compared with light labor (45%). Statistical analysis revealed that the age distribution in both groups was not significantly different, with P > .05.
Characteristics of disease
The majority of patients in both groups had been suffering from the disease for 3–6 months, accounting for 56.7% in SG and 53.3% in CG. The distribution of patients according to the duration of the disease did not show any significant difference between the two groups, with P > .05. Table 1 displays the baseline assessment at the time of admission. The pain level, lumbar spine range of motion (flexion, extension, tilt, rotation), lumbar spine stretch, and daily living function in both groups were similar, with P > .05 (Table 1).
Pathological Characteristics Before Treatment of the Two Groups
CG, control group; SG, study group; VAS, visual analog scale.
Table 2 exhibits the characteristics of X-ray images before the treatment in both groups. The image of subchondral bone solidification was the highest, with 63.3% in the SG and 60% in the CG. The value P > .05 shows no discrepancy observed between the two groups (Table 2).
Characteristics of X-Ray Images of the Two Groups Before Treatment
CG, control group; SG, study group.
Analgesic effect according to the VAS scale
The overall outcome in both SG and CG was significantly improved after 14 days and 28 days of treatment. The number of patients experiencing no or mild low back pain increased, while the number of patients with moderate pain decreased. The statistical analysis with P < .05 demonstrated notable pain alleviation in both groups from the 14th day to the 28th day of treatment.
Table 3 further illustrates the differences between the SG and CG, with P < .05. After 14 days of treatment, 30% of patients in the SG reported no pain, 53.3% experienced mild pain, and 15.7% had moderate pain. In contrast, only 6.7% of patients in the CG had no pain, 60% reported mild pain, and 33.3% experienced moderate pain. After 28 days of treatment, pain management in the SG proved more effective, with 63.3% reporting no pain, 33.3% experiencing mild pain, and only 3.4% reporting moderate pain. In comparison, the percentage of patients in the CG with no pain was 26.7%, mild pain was 56.7%, and moderate pain was 16.7% (Table 3).
Pain Level According to VAS of Two Groups Over Time
CG, control group; SG, study group.
Improve lumbar spine stretch according to the Schober test
Table 4 presents a comparison of the degree of lumbar spine flexibility between the two groups before and after the treatment. The lumbar spine stretchability was found to be similar in both groups at the time of admission to the hospital. However, after 14 days and 28 days of treatment, the lumbar spine flexibility showed a significant improvement, with a shift toward good and very good results. The number of patients with moderate and poor lumbar spondylolisthesis decreased drastically after the treatment. The improvements observed from the 14th to the 28th day in both groups were statistically significant, with P < .05.
Degree of Lumbar Spine Dilatation According to Schober Test Over Time
CG, control group; SG, study group.
Following 14 days of treatment, there were no patients with low lumbar spondylolisthesis. In the SG, 23.3% of patients exhibited good lumbar spine dilatation, whereas in the CG, this percentage was only 3.3%. After 28 days of treatment, the number of patients with good lumbar spine flexibility in the SG increased to 56.7%, approximately twice the number of patients in the CG, which accounted for 26.7%. The difference in the degree of lumbar spine stretch between the SG and CG was profound (P < .05), indicating a significantly greater enhancement in the SG’s lumbar spine flexibility compared with the CG (Table 4).
Enhance fingertip-to-floor distance
After 14 days and 28 days of treatment, there was a significant decrease in the number of patients in both the SG and the CG with fingertip-to-floor distance, with no poor results observed. Notably, there was a remarkable shift (P < .05) from moderate to very good results observed between the 14th and 28th days of treatment.
Table 5 illustrates the reduction trend in fingertip-to-floor distance for both groups. On the 14th day of treatment, the percentage of patients in the SG with very good hand spacing was calculated to be 36.7%, which was more than ten times the percentage observed in the CG, which was only 3.3%. Similarly, on the 28th day of treatment, the number of patients with good hand spacing in the SG (56.7%) was more than twice that of the CG (26.7%). The statistical analysis with P < .05 further demonstrated a significant difference in the overall outcome of the two groups (Table 5).
Level of Fingertip-To-Floor Distance of Two Over Time
CG, control group; SG, study group.
Increase the degree of spinal flexion
Table 6 demonstrates a notable trend in the improvement of spinal flexion for both the SG and the CG. Both groups exhibited significant enhancement in the degree of flexion after the treatment, with no poor results reported after 14 days of treatment. From the 14th day to the 28th day, there was a drastic increase in the number of patients achieving very good results and a decrease in the number of patients with moderate results.
The effectiveness of the treatment in the SG is clearly demonstrated through the statistical analysis with P < .05. After 14 days of treatment, the number of patients in the SG with very good spinal flexion accounted for 36.7%, while in the CG, it was only 3.3%. Following 28 days of treatment, the number of patients with very good spinal flexion further increased to 60% in the SG and 26.7% in the CG (Table 6).
Degree of Spinal Flexion of the Two Groups Over Time
CG, control group; SG, study group.
The overall outcomes of the treatment in SG and CG groups
After 28 days of treatment, the SG showed a significantly higher improvement rate compared to the CG. This shift toward very good results was statistically significant with P < .05, as depicted in Figures 1 and 2.
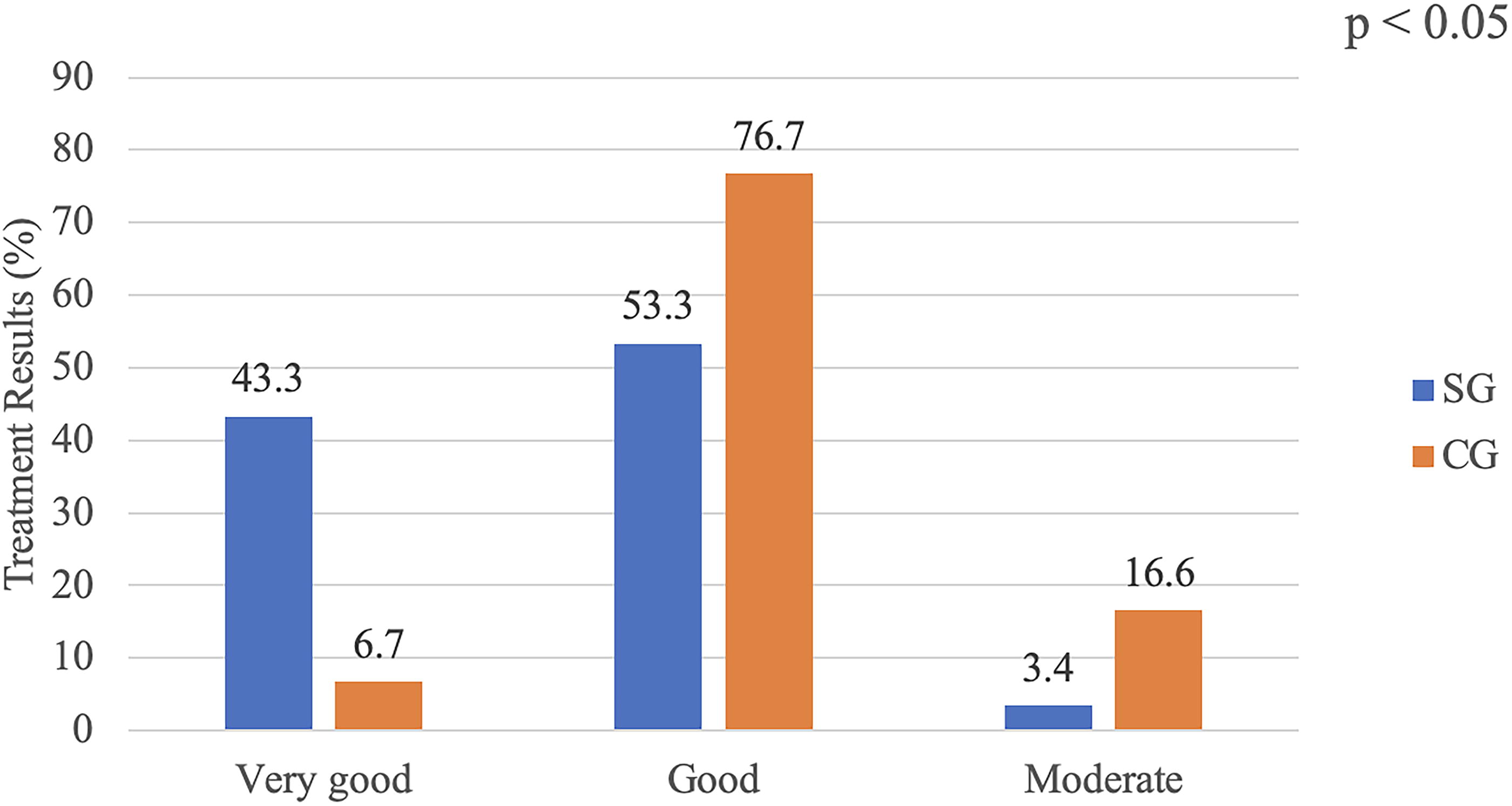
Overall treatment results after 14 days of treatment of two groups.
On the 14th day of treatment, the overall treatment outcome for the SG was as follows: very good results for 43.3% of patients, good results for 53.3%, and moderate results for 3.4%. In comparison, the CG had 6.7% with very good results, 76.7% with good results, and 16.6% with moderate results (Fig. 1).
On the 28th day of treatment, a noticeable shift from good to very good results was observed in the SG, with very good results for 76.7% of patients, good results for 20%, and moderate results for 3.3%. Similarly, in the CG, there was a similar trend, with very good results for 46.7%, good results for 43.3%, and moderate results for 10% (Fig. 2).
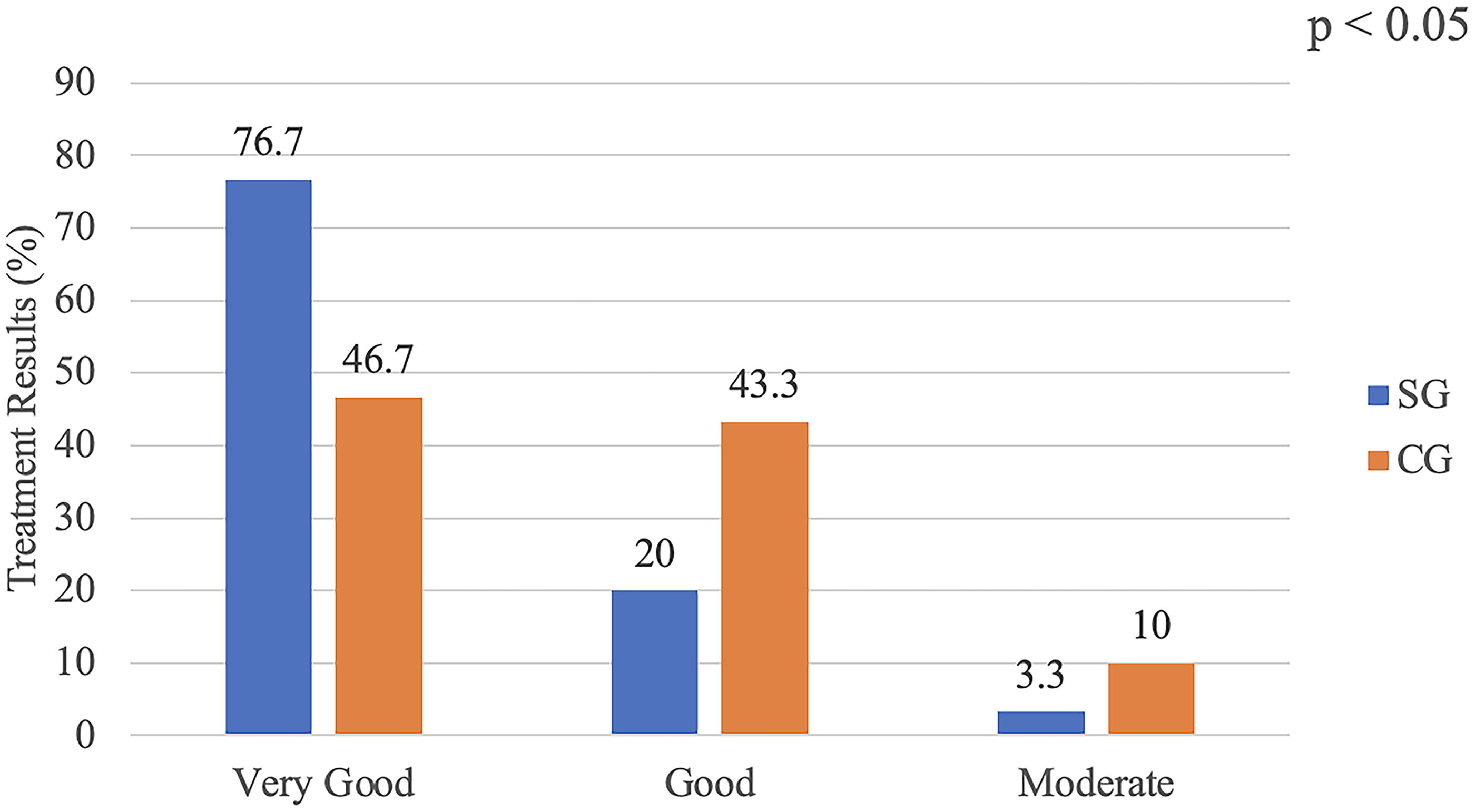
Overall treatment outcome after 28 days of two groups.
Monitoring undesirable effects in SG and CG during the 28 days of treatment
The laboratory values of the patients participating in the study were within normal limits, including white blood cells, red blood cells, hemoglobin, platelets, urea, creatinine, glucose, and liver enzymes. Throughout the study, the patients in both groups denied adverse effects. The statistical analysis (P > .05) in Table 7 further demonstrates normal physiological functions with no complications observed in these patients (Table 7).
Paraclinical Index Before and After Treatment in the SG and CG
ALT, aminotransferase; AST, aspartate aminotransferase.
DISCUSSION
LDD is a chronic condition that leads to pain, limited movement, and deformity of the lumbar spine without inflammatory manifestations. The main damage caused by LDD is the degeneration of articular cartilage and spinal discs, often associated with changes in the subchondral bone. 1 This condition is closely related to age, as disc degeneration tends to worsen with increasing patient age. 31,32 Despite its global prevalence and significant impact on individuals and society, there is a need for systematic diagnosis and effective management of LDD and its associated lower back pain. 5 Patients with low back pain experience intense radiating leg pain that may be accompanied by neurological signs associated with high health care costs, work absenteeism, and economic burden. 33
In this study, the baseline characteristics of age, gender, occupation, disease duration, clinical symptoms, and pretreatment pathological factors were statistically similar between the SG and the CG. This ensured the objective and accurate evaluation of the treatment effects in both groups. Radiographical examinations revealed comparable findings of degenerative lesions in the lumbar spine for both SG and CG, characterized by joint space narrowing, bone spurs, subchondral thickening, and intervertebral foramen narrowing, which can lead to spinal deformities and loss of physiological curves. The most prevalent radiographical finding in both groups was subchondral bone solidity, indicating a consistent presentation of LDD (60% for CG and 63% for SG).
Pain is the primary reason patients with LDD seek treatment. The data from this study demonstrated that VH treatment produced a robust analgesic effect for the patients. The VAS score significantly improved after 14 and 28 days of treatment in the SG compared to the CG and the baseline measurement (D0). In addition, VH treatment resulted in improvements in various aspects related to the patients’ spinal movement limitations and reversed uncomfortable complications associated with LDD. Notably, there were statistically significant positive differences in the Schober test readings, fingertip-to-floor distance, spinal flexion, painful side spine tilt, and spinal rotation on the painful side between the SG and CG.
The combination of VH with electro-acupuncture appears to benefit the overall treatment outcome due to a synergistic effect between electro-acupuncture and VH preparation. The treatment was well-tolerated, and safety assessments indicated no unwanted effects during the 28 days of treatment and clinical monitoring. Patients did not experience adverse events such as stinging, bleeding, shock, rash, diarrhea, nausea, or weakness.
CONCLUSION
This study highlights the effectiveness and safety of VH tablets in conjunction with electro-acupuncture for managing low back pain induced by LDD. The combination therapy showed superior results compared to electro-acupuncture alone, providing significant pain relief and improving spinal flexibility and mobility. The positive outcomes and favorable safety profile make VH tablets a promising option for the management of LDD-related low back pain.
Footnotes
AUTHORS’ CONTRIBUTIONS
P.T.T.: Investigation, data curation, writing—original draft. Q.T.H.: Investigation, data curation, writing—review and editing. L.V.T.: Investigation, visualization, data curation, writing—review & editing. A.K.N.: Writing—review and editing. B.H.: Conceptualization, prepared the tables, figure, writing—review and editing. B.X.H.: Methodology, conceptualization, writing—original draft—reviewing and editing. All authors read and approved the article prior to submission.
AUTHOR DISCLOSURE STATEMENT
The authors declare no conflicts of interest.
FUNDING INFORMATION
This study was investigator-initiated and nonfunded.