
Abstract
Abstract
Purpose:
To determine the effect of 4 formulations of commercially available prostaglandin analogs (PGAs) on human corneal epithelial cells in vitro.
Methods:
The test solutions (PGAs) examined were tafluprost 0.005% with 0.010% benzalkonium chloride (BAK), travoprost 0.004% with 0.015% BAK, travoprost 0.004% with sofZia™, and latanoprost 0.005% with 0.020% BAK. Also tested independently were the 4 respective BAK or sofZia concentrations related to each PGA. Balanced salt solution (BSS) was used as the live control, and a fixative solution containing 70% methanol and 0.2% saponin was used as the dead control. Immortalized human corneal epithelial cells were exposed to test or control solution for 25 min at 37°C and 5% CO2. A live/dead assay was used to measure the toxicity of the PGAs.
Results:
The percentage of live cells in the PGA groups ranged from 2% to 72% of the BSS group (live control). The PGA with the highest relative live cell percentage, at 72% of the live control, was travoprost with sofZia. The next highest PGA, exhibiting 14% live cells, was the formulation of travoprost containing BAK. The other 2 PGAs, tafluprost and latanoprost, had few surviving cells, with 3% and 2% live cells, respectively. The BAK concentrations exhibited 4%, 3%, and 3% for the 0.01%, 0.015%, and 0.02% concentrations, respectively. The stand-alone sofZia cell survival was 68% of the live control.
Conclusions:
All 4 PGA formulations tested demonstrated significantly more toxicity in human corneal epithelial cells than the live control, but there were significant differences among the PGAs. Travoprost with sofZia exhibited the least toxicity, followed by travoprost with BAK, and then tafluprost and latanoprost. The stand-alone preservative systems were also tested and showed similar survival percentages to each respective PGA. The true clinical implications of these findings require further investigation.
Introduction
One of the most commonly prescribed classes of hypotensive agents are prostaglandin analogs (PGAs), which are frequently used as first-line monotherapy for patients with glaucoma or ocular hypertension, reducing IOP by ∼25%–30%. 2 However, conventionally preserved PGAs are known to cause a number of in vivo ocular surface alterations, including loss of corneal epithelial tight junctions, 3 reduction in superficial epithelial density, 4 and an increase in basal epithelial density. 5 In vitro studies have also shown that PGAs produce expression of inflammatory markers on the surface of conjunctival cells 5 as well as induce toxicity in ocular surface cell lines.6–8
The aim of this study was to compare the relative effects of 4 PGA formulations with varying concentrations of benzalkonium chloride (BAK) or the oxidizing preservative sofZia™ on cultured human corneal epithelial cells. Critical to this study was the comparison between 2 formulations of travoprost (with and without BAK) that could shed light on the relative contributions to cell toxicity of the active ingredient and the preservative systems.
Methods
Cell culture
The transformed human corneal epithelial cell line (10.014 pRSV-T) was obtained from the American Type Culture Collection (Manassas, VA). Corneal epithelial cells were cultured at 37°C and 5% CO2 in Keratinocyte-Serum-Free Medium (Invitrogen, Carlsbad, CA) containing 5 ng/mL human recombinant epidermal growth factor (Invitrogen), 0.05 mg/mL bovine pituitary extract (Invitrogen), 0.005 mg/mL insulin (Sigma-Aldrich Corp., St. Louis, MO), 500 ng/mL hydrocortisone (Sigma-Aldrich Corp.), and antibiotics. Flasks and plates used for culturing were previously coated with 0.01 mg/mL bovine serum albumin (Sigma-Aldrich Corp.), 0.01 mg/mL human fibronectin (BD Biosciences, San Jose, CA), and 0.03 mg/mL bovine collagen type I (BD Biosciences) for 2 h at 37°C.
Reagents
The test solutions were tafluprost 0.0015% with 0.01% BAK (Taflotan; Santen Pharmaceutical Co., Ltd., Osaka, Japan), travoprost 0.004% with 0.015% BAK (Travatan; Alcon Laboratories, Inc., Fort Worth, TX), travoprost 0.004% with sofZia (Travatan Z; Alcon Laboratories, Inc.), sofZia preservative alone (Alcon Laboratories, Inc.), latanoprost 0.005% with 0.02% BAK (Xalatan; Pfizer, Inc., New York, NY), as well as a range of BAK concentrations (Alcon Laboratories, Inc.). The live control was balanced salt solution (BSS; Alcon Laboratories, Inc.) and contained the following: 6.5 g/L sodium chloride (NaCl), 0.75 g/L potassium chloride (KCl), 0.48 g/L calcium chloride dihydrate (CaCl2 · 2H2O), 0.3 g/L magnesium chloride hexahydrate (MgCl2 · 6H2O), 3.9 g/L sodium acetate trihydrate (C2H3NaO2 · 3H2O), 1.7 g/L sodium citrate dihydrate (C6H5Na3O7 · 2H2O), and sodium hydroxide and/or hydrochloric acid to adjust pH to ∼7.5. The dead control was a fixative solution containing 70% methanol and 0.2% saponin in phosphate-buffered saline (PBS).
LIVE/DEAD® Viability/Cytotoxicity Kit for mammalian cells (Invitrogen) contained stock solutions of 2 mM ethidium homodimer (Eth-1) and 4 mM Calcein-AM dissolved in dimethyl sulfoxide (DMSO). Dulbecco's PBS (D-PBS) without calcium or magnesium (Invitrogen) was used to prepare all stains before use. D-PBS had an approximate pH of 7.4 and contained the following: 0.2 g/L KCl, 0.2 g/L potassium phosphate monobasic (KH2PO4), 8 g/L NaCl, and 2.16 g/L sodium phosphate dibasic heptahydrate (Na2HPO4 · 7H2O).
Experimental procedure
Fifty thousand human corneal epithelial cells were plated into each well of a coated 96-well plate in the culture medium. Cells were assayed upon reaching confluence, usually 2–3 days postplating. The culture medium was removed by aspiration and replaced with 100 μL of test or control solution (each solution was performed in triplicate). Cells were then incubated at 37°C and 5% CO2 for 25 min. After incubation, test solutions were removed and replaced with 100 μL of D-PBS containing 2 μM Calcein-AM. The final concentration of DMSO from the stain stock solution was ≤0.1%, a level generally innocuous to most cells.
Fluorescence was quantified within 20 min of addition of stain in a Synergy™ 4 Multi-Mode Microplate Reader using the Gen5™ Reader Control and Data Analysis Software (BioTek, Winooski, VT). Live cells were quantified by determining the Calcein fluorescence emission at 528 ± 20 nm from a 485 ± 20 nm excitation using band-pass filters (F528).
Determination of live cells
Fluorescent data were analyzed as outlined in the manufacturer's instructions. Briefly, all F528 fluorescence from cells stained with 2 μM Calcein-AM was corrected by first subtracting the F528 fluorescence of cells in wells lacking Calcein stain, as this represents the nonspecific fluorescence. The percent of live cells in each well was then determined by dividing the corrected F528 fluorescence by the average corrected F528 fluorescence in the BSS-treated cells from each experiment (100% Live Control). Data for each treatment are reported as mean ± standard deviation (n = 9).
Imaging of living/dead epithelial cells
An inverted IX81 microscope (Olympus, Center Valley, PA) with spinning-disk using filters sets for fluorescein isothiocyanate (FITC; excitation 480 ± 20 nm, emission 535 ± 25 nm) and tetramethylrhodamine isothiocyanate (TRITC; excitation 535 ± 25 nm, emission 610 ± 37.5 nm) was used to image live (FITC) and dead (TRITC) cells. Cells were viewed using a long working distance PLAN Fluorite 40 × objective, and images were taken with a Hamamatsu ORCA IIER monochromatic CCD camera using Intelligent Imaging Slidebook acquisition software (Olympus).
Statistical analysis
Each experiment was performed in triplicate. Three independent experiments were performed on 3 different dates. Results represent the means of 9 wells/test condition (3 wells each in 3 different assays), expressed as a percentage of BSS-treated live control cells. Mean values for each concentration were analyzed by the Student's t-test (Excel, Microsoft, Redmond WA); the level of significance was set at 0.05.
Results
As shown in Fig. 1, the percentage of live cells in the test solutions relative to BSS control solution ranged from 2% to 72%, depending on the PGA. The PGA with the highest relative live cell percentage was travoprost with sofZia, with 72% live cells (P < 0.00001). The next highest PGA, exhibiting 14% live cells, was the formulation of travoprost containing BAK. The other 2 PGAs, tafluprost and latanoprost, had few surviving cells, with 3% and 2% live cells, respectively. The BAK concentrations exhibited 4%, 3%, and 3% for the 0.01%, 0.015%, and 0.02% concentrations, respectively. The stand-alone sofZia cell survival was 68% of the live control, statistically identical to travoprost with sofZia (72%, P = 23). However, travoprost with BAK had statistically fewer live cells (14%) than travoprost with sofZia (72%, P < 0.0001). The above data is illustrated qualitatively in Figure 2, which shows representative images of the corneal epithelial cells treated with the various test and control solutions.
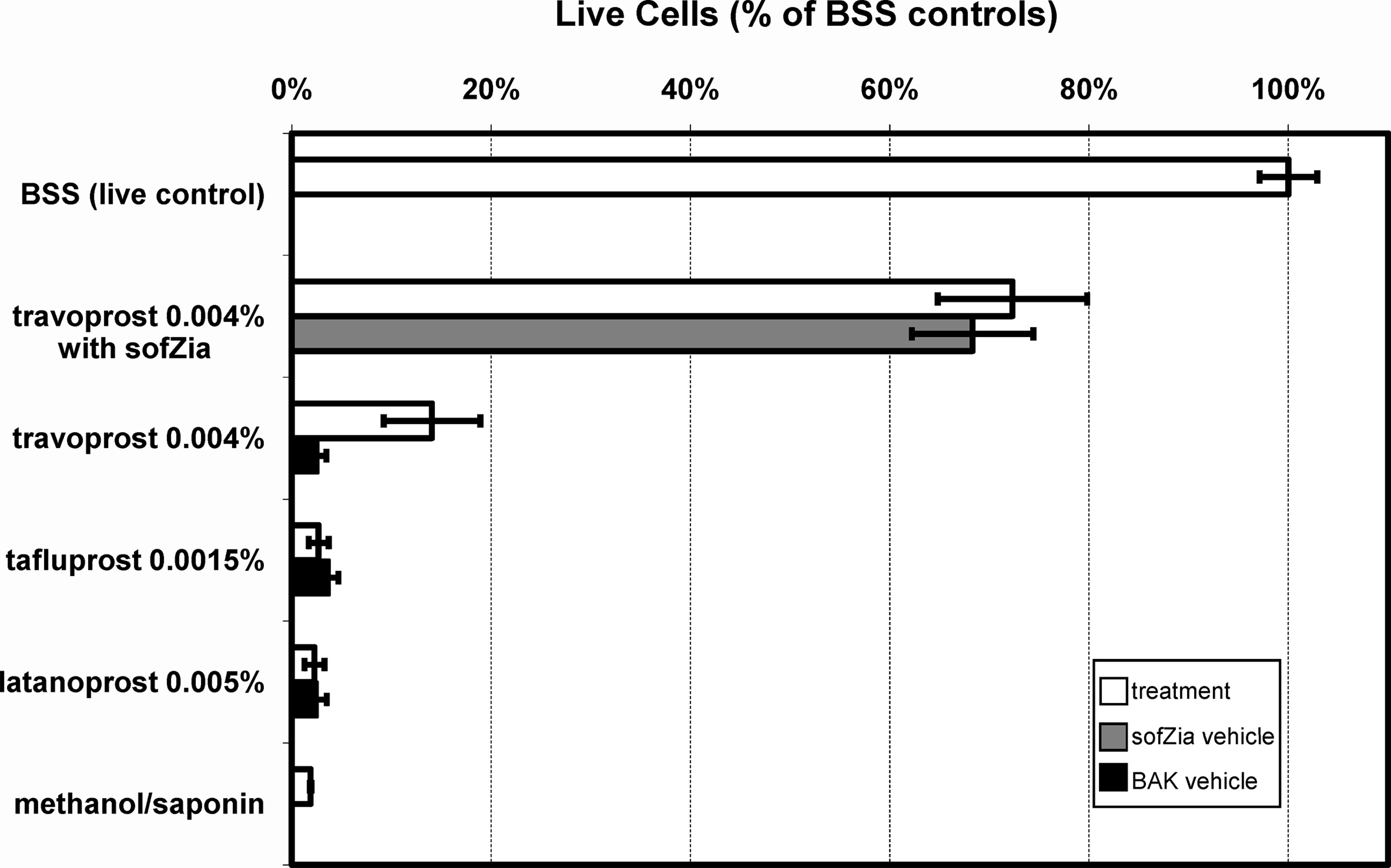
Live cell assay. The percent of live corneal epithelial cells after a 25 min exposure to 4 different topical ocular prostaglandin analogs and control solutions is shown. The number of live cells was normalized to the number of live cells in balanced salt solution (BSS)–treated controls. Data are reported as the mean ± standard deviation of n = 9 replicates.

Qualitative representation of data presented in Fig. 1. Corneal epithelial cells are labeled in green (live) or red (dead). Increasing concentrations of benzalkonium chloride (BAK) increase the number of dead cells. Compared to travoprost + BAK, travoprost + sofZia results in significantly more live corneal epithelial cells.
Discussion
The current study uses an assay that distinguishes living cells by their ability to hydrolyze the cell-permeable (but nonfluorescent) Calcein-AM into the nonpermeable but strongly fluorescent green Calcein dye. Similarly, the leaky plasma and nuclear membranes of dead cells allow the entry of the red nuclear stain Eth-1. We used this live/dead cell assay to determine the effects of 4 PGA formulations on cornea cells in vitro. The respective preservative from each medication was also independently evaluated. Latanoprost and tafluprost were nearly indistinguishable from dead controls, with nearly 100% toxicity of the human corneal epithelial cells. Travoprost with sofZia had the highest percentage of live cells, followed by the original BAK-containing formulation of travoprost. The preservative systems performed similarly to their respective PGA. This, to our knowledge, is the first study to demonstrate the stand-alone effects of sofZia on cultured human corneal epithelial cells. Our results are consistent with previous publications showing that travoprost with sofZia produces fewer ocular surface changes than other PGAs, and the current data indicate that the preservative systems are the likely culprit for the observed differences.3,7,9–14
BAK is the most common preservative used in topical ophthalmic medications and is believed to be a major cause of toxicity noted with PGA formulations.15–24 BAK is a quaternary ammonium compound that acts as a detergent, disrupting bacterial cell membranes and ultimately leading to bacterial cell death. Similar effects for BAK have been noted in numerous in vitro studies on human corneal and conjunctival epithelium and stroma.15,21–24 Alternative preservative systems such as the oxidizing preservative sofZia have been developed to potentially diminish the deleterious effects on epithelial cells after chronic exposures while still protecting multidose bottles from pathogen contamination. Oxidizing preservatives cause oxidative damage in bacteria and subsequent death due to the lack of oxidases and catalases in these organisms. Human cells possess these enzymes and are thus not similarly harmed.
This study compares the toxicity of travoprost with 2 different preservatives, a head-to-head comparison since the active ingredient is the same. This study appears to support the fact that oxidizing preservatives, in this case sofZia, are less toxic than common concentrations of BAK. It is important to emphasize that the clinical significance of the toxicity differences observed among the 4 PGA formulations has not yet been firmly established. In short-term studies, all 4 PGA formulations show little to no adverse effects on the ocular surface.25–28 However, since glaucoma is a chronic condition, the safety of the long-term use of these agents is of critical importance. Clinical studies involving patients on chronic topical glaucoma therapy show a link between various ocular surface disease metrics and increasing number of topical drops.29,30 Still, the majority of clinical studies fail to show a direct dose-related effect of BAK on ocular surface health matching the plethora of available in vitro data.4,5 This is likely a result of the poor metrics we currently have available to us for in vivo studies. Further studies are needed to better understand how in vitro findings correlate with clinical observations from once daily dosing with each of these medications.
Footnotes
Author Disclosure Statement
Research support was received from Alcon Laboratories, Inc., for this study. Dr. Kahook is a consultant for Alcon Laboratories, Inc., Allergan, and Merck.