
Abstract
Abstract
Purpose:
To report the incidence of traumatic lens injuries as a complication of intravitreal injection at 5 high-volume academic centers.
Methods:
We determined in a retrospective, interventional, multicenter case series the consecutive number of the injections between January 5, 2006 and December 22, 2008 from the injection log books. All injections were performed under sterile conditions in a laying position, 3.5–4.0 mm behind the limbus in an oblique fashion. The main outcome measure was the incidence of lens damage.
Results:
A total of 32,318 intravitreal injections were performed, and 3 cases of iatrogenic lens damage were reported during 36 consecutive months. All affected eyes were hyperopic. The overall incidence rate of lens injury was 0.006% (2/32,318) for intravitreal injections and 1 during a paracentesis 0.003 (1/32,318). The rate of phakic eyes determined was 67%, and thus, the incidence rate of lens damage in phakic eyes was 0.009% (2/21,653) (95% confidence interval, 0.00%–0.05%).
Conclusions:
Although there is no agreement regarding the proper intravitreal injection technique, the incidence of traumatic injuries to the crystalline lens was very low in a large series of injected patients in a community setting. The incidence compares favorably with that reported in clinical trials in which much more extensive preinjection preparation was mandated. A good preparation of the surgical incision with proper anesthesia and detailed information of the patient, as well as good anatomical skills of the treating physician, are mandatory to prevent this rare adverse event.
Introduction
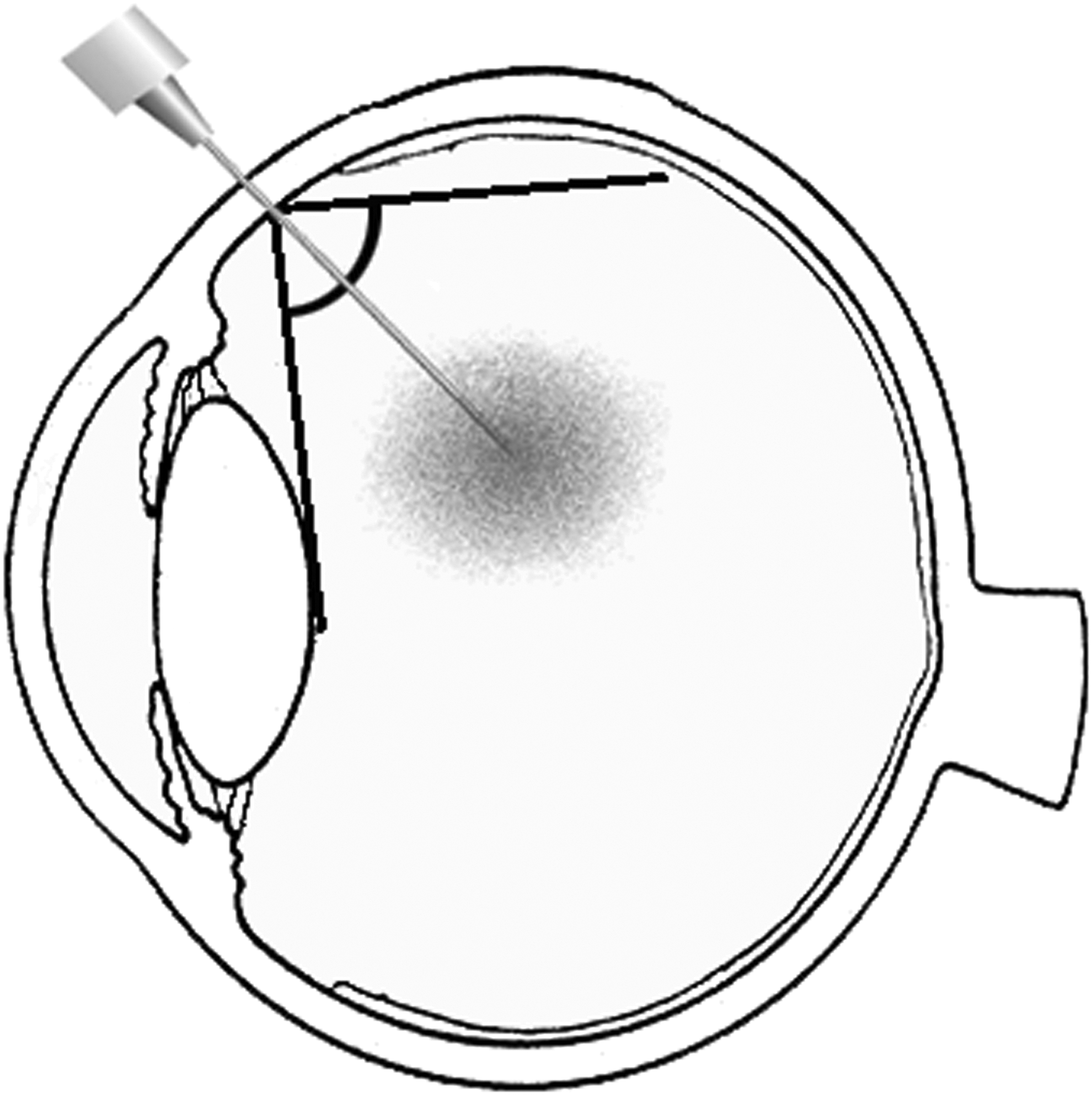
Schematic drawing of the ocular anatomy in a normal Gullstrand eye, demonstrating a presumed angle of ∼90° between the posterior capsule of the crystalline lens and the retinal surface.
Although there are some anecdotal reports of iatrogenic lens damage, the exact incidence rate remains unknown. Larger safety surveys such as the Pan-American Collaborative Retina Study Group reported no lens damage after 4,303 injections during a period of 12 months in 1,310 eyes. 9 An online survey by Fung et al. mentioned one lens injury among 7,113 reported intravitreal injections, 10 whereas the VISION-study observed 5 lens injuries during 7,545 injections (0.06%). 11
The primary goal of this paper was to report selected cases of injuries to the crystalline lens during intravitreal drug applications. The secondary outcome measures were to determine possible risk factors and to calculate the incidence of this event over a 36-month period among 5 high-volume centers performing this procedure on a frequent basis.
Methods
The total number of intravitreal injections given from January 5, 2006 to December 22, 2008 at the 5 centers was retrospectively determined by reviewing billing records and injection logs. Additional telephone feedback from referring physicians was obtained, and conversations were arranged with other vitreoretinal groups in the area to query for possible unknown lens damage not documented in this initial review; however, no missing cases were detected. All case notes were evaluated for documented evidence of lens damage. The medical records of all affected patients were systematically analyzed to determine specific risk factors for this adverse event. The following information was collected for each affected patient: age, gender, retinal disease, spherical equivalent, axial length of the globe, number of previously received injections, and presence of prominent eye brows or small lid margins, as well as subjective fear or pain sensation [(0/10) no pain, (10/10) severe pain] of the patient during the procedure. In addition, we determined the surgical experience of the injecting physicians and their cumulative number of uneventful injections previously performed.
The injection procedure was the same at all 5 centers: all patients received the intravitreal injections as a standardized procedure performed under sterile conditions in a supine position. Before each injection, topical proparacaine and 4% lidocaine anesthetic drops were instilled into the eye, followed by 5% povidone iodine solution applied to the eyelid skin, eyelashes, and lid margin, as well as the ocular surface. All surgeons inserted a sterile wire speculum and cover sheet on all procedure eyes. A microscope and sitting chair for the surgeon was used depending on their personal discretion. The distance of 3.5–4.0 mm was meticulously marked from the limbus using a caliper to reduce the misjudgment. At the determined injection site, the tip of the needle was gently inserted through the conjunctiva and adjacent sclera in an oblique fashion toward the center of the optic nerve. 12
The mean incidence of phakic and pseudophakic eyes among all injected eyes was randomly calculated on a representative sample of 100 charts at each center. Based on the number of reports of lens damage, as well as the presence of phakic and pseudophakic eyes, we calculated the incidence for all intravitreal injections as well as for pseudophakic eyes in particular.
Statistical methods
The main outcome measure was the incidence of iatrogenic lens damage during intravitreal injections. The tabulated data were examined with descriptive and frequency analysis. The CIs were calculated with exact binomial methods given the low incidence of the main outcome measure.
Results
A total of 32,318 intravitreal injections were performed between January 5, 2006 and December 22, 2008 at the 5 study centers. During this consecutive 36-month study interval, 3 cases of lens damage were reported 1–4 days after the injection. There was no accumulation of cases in any one center. The overall incidence rate of lens injury was 0.006% (2/32,318) for intravitreal injections and 1 during a paracentesis 0.003 (1/32,318). The mean rate of phakic eyes was determined to be 67%, and thus, the incidence rate of lens damage in phakic eyes was 0.009% (2/21,653; 95% CI, 0.00%–0.05%). No affected patients had signs of prominent eye brows or small lid margins. Ocular anesthesia was adequate, and the patients reported no pain during the procedure. The 2 affected eyes were hyperopic with an axial length <22 mm. Further evaluations regarding possible risk factors on the patient's or physician's side are summarized in Table 1.
Abbreviations: OD, right eye; OS, left eye; sup-temp, superotemporal; inf-temp, inferotemporal.
Case 1
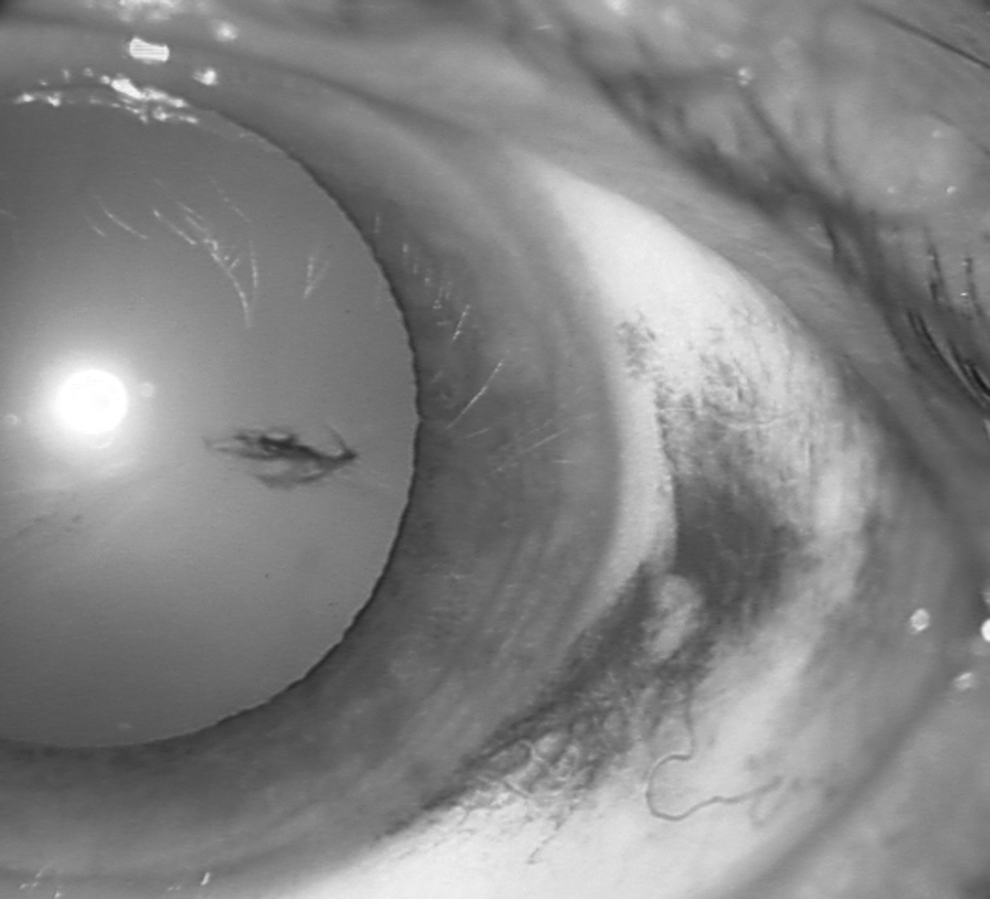
An 84-year-old lady with vascular age-related macular degeneration (AMD) in her right eye (OD) complained of decreased visual acuity 4 days after a second intravitreal injection. Her best-corrected visual acuity (BCVA) declined from 20/200 to 20/800 OD. Slit-lamp examination determined the development of a novel posterior lens opacification, adjacent to a tunneled perforation site of the posterior capsule (Fig. 2). After phacoemulsification and implantation of an intraocular lens in the sulcus, her BCVA improved to 20/100 at 2 months follow up. The patient's medical history was significant for hyperopia. The spherical equivalent was +4 dpt, and biometry revealed an axial length of 21.5 mm.

A crystalline lens 2 days after an iatrogenic penetration during an intravitreal injection. The channel of the insertion site is still visible, and there is an adjacent feather-like opacification at the posterior pole of the lens.
Case 2
A 74-year-old man with vascular AMD developed an immediate lens opacification after his fourth intravitreal injection in his right eye; there was a sheen-like transparency loss at the posterior aspect of the crystalline lens. Phacoemulsification with anterior vitrectomy and implantation of an intraocular lens in the sulcus was immediately performed in the operating room. The patient's ocular history was significant for hyperopia. The eye was hyperopic with a spherical equivalent of +1.25 dpt, a shallow anterior chamber, and an axial length of 22.9 mm.
Case 3
An 84-year-old man with vascular AMD in his left eye initially received 4 consecutive uneventful ranibizumab injections. His initial VA was 20/100. Six months later, he developed a subretinal hemorrhage, which was treated with a triple injection, using 0.05 mL recombined tissue plasminogen activator (rtPA) (50 μg), 0.3 mL of sulfur hexafluoride gas, and 0.05 mL bevacizumab (1.25 mg). The patient performed a slight head motion during a consecutive anterior chamber paracentesis, resulting in mild damage of the iris stroma and anterior lens capsule. A successful inferior displacement of the subretinal hemorrhage was achieved, and the puncture of the anterior lens capsule appeared constant. The status of the lens clarity was closely followed. However, his cataract formation appeared similar in both eyes, and so far, there has been no visible progression of the lens opacification requiring phacoemulsification. His BCVA was 20/100 at 6 weeks follow up (Fig. 3).
A crystalline lens 2 weeks after an iatrogenic lens touch during anterior chamber paracentesis. There is a mild alteration of the iris stroma with adjacent pigmented debris on the surface of the lens.
Discussion
Intravitreal injections were initially described by Ohm to employ an intravitreal air tamponade in a retinal tear. 13 Each injection can potentially damage the 3 major anatomical structures. (1) A posterior placement may damage the ora serrata or even pass through the neuroretina, inducing a full thickness retinal tear and consecutive development of a rhegmatogenous detachment. (2) An anterior placement may damage the ciliary body, leading to ocular pain or intravitreal bleeding. (3) Finally, the recommended angle at the entry site is limited by the angle between the posterior capsule of the crystalline lens and the retinal surface (Fig. 1).
Extensive clinical experience with intravitreal injections has provided clinicians with an outline of avoidable risks through empirical experience. At present, numerous comprehensive reports have evaluated this technical approach and developed a set of guidelines for intravitreal injections 14 : The potential of inadvertent intraocular damage to the posterior surface of the crystalline lens during intravitreal injections limits access to anterior retinal disease near the ora serrata. The injection needle normally passes through the pars plana into the midvitreous, avoiding damage of adjacent intraocular anatomical structures. Smiddy et al. 14 measured the intraocular distance between the crystalline lens and straight surgical instruments for different locations of the sclerotomy. They demonstrated in phakic eyes that sclerotomy sites 4.0 mm posterior to the limbus were advantageous compared with sclerotomy sites that were further anterior. Injections 3.5 mm posterior to the limbus may substantially narrow the angle, whereas a further posterior insertion may violate the anterior base of vitreous and act as a focus for future intraocular traction and tear formation.
The angle of the incision through the sclera should be oblique, using an oblique or tunneling technique (45°), as rectangular radial incisions (90°) may remain open, inducing vitreous incarceration or drug reflux under the conjunctiva. 15 Previously, we observed persistent unsealed sclerotomies after radial injections using 30-gauge needles. 16
The depth of the insertion should be between 5 and 7 mm, so that the tip of the needle is placed presumably in the center of the vitreous cavity. The drug should be gently introduced into the vitreous cavity, as the jet of a fast-injected drug (e.g., rtPA or antibiotic) may damage the retinal surface, which is frequently seen during careful examination as retinal whitening at the area perpendicular of the trajectory of the injection.
The recommended diameter of the needle should be smaller than 25 gauge to reduce the risk of injury to ocular structures or of wound leakage. Injections with crystalline triamcinolone are frequently applied with 27-gauge needles, whereas most liquid injections are performed with 30-gauge needles. Experimental studies measured almost twice as much mechanical force to penetrate the sclera with a 27-gauge needle compared with smaller needles. 17 Larger needles may not necessarily induce more pain to the patient but apparently more trauma, reflux, subconjunctival hemorrhage, and possible damage to the crystalline lens. 18 In addition, reduced sharpness of the needles, as found in some prefilled syringes, also induces a deeper inpouching and visible indentation of the eye wall, which may narrow the distance between the needle tip and the lens.19,20 All these aspects should be taken into consideration to perform safe injections.
Outside of prospective clinical trials, no additional studies currently exist investigating the incidence of lens damage related to intravitreal injections. Although it is difficult to compare data regarding lens injuries associated with intravitreal injections or a paracentesis, it is thought that the overall incidence is low according to Jager et al. 2 The VISION-Study used a 27-gauge needle, which is larger than the conventional needle used for antivascular endothelial growth factor agents. In the VISION-study, involving 890 patients and a total of 7,545 injections, 5 subjects developed iatrogenic traumatic cataracts (0.06%) during the first 54 weeks of the study. 11 There was a contact or penetration of the lens with the injection needle in 4 patients; 2 of these events occurred on the same day at the same clinical site by the same investigator. In the fifth subject, the needle punctured the anterior lens capsule during an additional anterior chamber paracentesis. There were no cases of lens damage in the ANCHOR trial, whereas the MARINA trial reported one incident of iatrogenic lens damage among a total of 10,443 injections.21,22 The protocol of these prospective clinical trials included the evaluation of cataract progression, thus it is unlikely that any case of lens injury may be missed.
Numerous groups have evaluated the usefulness of a paracentesis to reduce a temporarily elevated IOP and have concluded that a routinely applied paracentesis is not mandatory, as the IOP returns to normal limits within minutes. 1 However, triple injections with 0.05 mL rtPA, 0.3 mL sulfur hexafluoride gas, and 0.05 mL bevacizumab induce a subsequent elevated IOP, requiring an anterior chamber paracentesis. 23 Although an increased volume in the vitreous cavity may narrow the anterior chamber, pain and fear of the patient during the maneuver can lead to an unexpected eye or head movement, possibly triggering a touch of an adjacent ocular tissue by the needle. 24 A good preparation of the patient with a proper explanation, solid anesthesia, and gentle fixation of the globe and head may help avoid this iatrogenic damage.
Our consecutive, multicenter case series included a large sample size, thus allowing us to delineate a presumed range in which we are confident that the approximate rate of lens damage lies. Specifically, we were interested in the highest end of the 95% CI, as this level represents the rate below which we are confident that the true incidence would be. Based on our exact binomial 95% CIs, we calculated an incidence for damaged crystalline lens >1 per 16,159 injections and an overall rate of 0.006% (95% CI: 0.00%–0.05%).
Our series has some inherent limitations as a retrospective, noncomparative case series after treatment for various retinal diseases. We retrospectively identified the total number of injections and lens damages among 5 centers. The chance to miss additional lens damages was reduced, as (1) all patients were monthly evaluated by their injecting physician for at least 3 months after each injection. (2) Patients were instructed to immediately call the hospital if symptoms of decreased VA, redness of the eye, or pain occur. (3) Most referring physicians have no facility to treat endophthalmitis, iatrogenic lens damages, or retinal detachments. This was additionally confirmed by a telephone feedback and conversations with referring physicians to meet our primary goal to report all apparent cases of iatrogenic lens damages. We must confess that our secondary outcome measure, to calculate the incidence of this event, relies on the assumption that there was an equal distribution of injections among phakic and pseudophakic eyes. A representative study estimated the incidence of phakic and pseudophakic eyes at each center and calculated a mean rate of 67% phakic eyes. However, we do not know whether these phakic eyes received also an equal total number of injections. Thus, we have to acknowledge that phakic eyes may even receive fewer injections than pseudophakic eyes. Nevertheless, we included a large consecutive number of eyes over a 3-year period, allowing us to comment on the incidence of lens damage at 5 centers in Europe and South America. In spite of these limitations, our retrospective study showed that intravitreal injection has a very low risk of lens damage under routine conditions, lower than that shown in previous clinical trials. The difference in the calculated rate of iatrogenic lens damages was only moderate for all eyes (0.006%) and phakic eyes (0.009%), thus we can convince our patients that the risk to develop an iatrogenic lens damage is <1 after 11,000–16,000 injections.
Conclusion
The risk to develop an iatrogenic lens injury is <1 in 11,000 intravitreal injections. A good preparation of the surgical incision with proper anesthesia and head fixation and detailed information of the patient, as well as good anatomical skills of the treating physician, are essential to avoid this rare complication.
Footnotes
Acknowledgments
The work was presented in parts at the World Ophthalmology Congress (WOC) 2010 in Berlin, Germany. This work was supported by FAPESP—Fundação de Amparo à Pesquisa do Estado de São Paulo, the Pan-American Association of Ophthalmology/Pan-American Ophthalmologic Foundation, and Fehr Foundation Marburg.
Author Disclosure Statement
No competing financial interests exist.