
Abstract
Abstract
Purpose:
The purpose of this study was to evaluate the orally administered combination of flavonoids desmin and troxerutin with Centella asiatica and Melilotus for the treatment of diabetic cystoid macular edema (CME) without macular thickening.
Methods:
In this prospective, interventional, controlled study, 40 consecutive patients with type 2 diabetes and CME without macular thickening at optical coherence tomography were randomized into 2 groups of 20 subjects each (treatment and control groups). The treatment group received an oral combination of desmin (300 mg/day) and troxerutin (300 mg/day) with C. asiatica (30 mg/die) and Melilotus (160 mg/die) for 14 months. Best collected visual acuity, central retinal thickness at optical coherence tomography, retinal sensitivity (RS), and stability of fixation at microperimetry were measured at baseline and monthly for 14 months.
Results:
In both groups, mean best collected visual acuity, central retinal thickness, and stability of fixation did not show differences during follow-up (P > 0.05). At month 14, the RS was greater in the treated group (P = 0.01) and was significantly reduced in the control group only (P < 0.001). Five eyes in the study group showed disappearance of the intraretinal cysts after a mean time of 3.5 ± 0.3 months, which persisted in the following months. These 5 eyes presented a greater RS at each follow-up visit when compared with the control group (P < 0.05). Anatomic improvement was never reported in the control group.
Conclusions:
The orally administered combination of flavonoids, C. asiatica, and Melilotus could be beneficial in preserving RS in diabetic CME without macular thickening.
Introduction
Methods
In this prospective, interventional, controlled study, 40 consecutive patients with type 2 diabetes and CME without macular thickening at OCT were randomized into 2 groups of 20 subjects each (treatment and control groups). Informed consent was obtained from all the patients. The study was approved by the eye clinic's ethics committee at the University Federico II of Naples and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. Inclusion criteria were absence of clinically significant macular edema at clinical examination, presence of nonischemic CME, normal central retinal thickness (CRT) and normal foveal contour at OCT examination, and absence of any previous treatment for diabetic retinopathy in the 6 months preceding first examination. Exclusion criteria were coexisting ocular pathologies and significant media opacities that precluded fundus examination.
In the treatment group, an oral combination of desmin (300 mg/day) and troxerutin (300 mg/day) with C. asiatica (30 mg/day) and Melilotus (160 mg/day) was administered for 14 months.
All patients included in the study were evaluated at baseline and monthly for 12 months. At each visit, investigations included best corrected visual acuity (BCVA) after refraction using the ETDRS letters scale, slit-lamp examination, funduscopy and stereofundus photography, OCT, and central microperimetry (MP). Fluorescein angiography was performed at baseline to exclude ischemic macular edema. Mean value of glycosylated hemoglobin (HbA1c) and blood pressure were monitored at baseline and every 3 months. Normal HbA1c values were considered to be between 4% and 6%. Blood hypertension was classified as normal tension (<120/80), prehypertension (120–139/80–89), stage 1 (140–159 systolic or 90–99 diastolic), and stage 2 (≥160 systolic or ≥100 diastolic). 8
To evaluate CRT, a spectral domain scanning laser ophthalmoscope/OCT device (SD-SLO/OCT; Ophthalmic Technologies, Toronto, Canada) was used. CRT was considered as the thickness in the central 1-mm disc, representing the foveal area. An upper limit of 280 μm for normal CRT was chosen according to the previously reported normal retinal thickness values as measured with SD-SLO/OCT. 9 Normal foveal contour was determined by the presence of a well-formed U-shaped foveal depression without marked steepening, flattening, or asymmetry. Intraretinal cysts were identified as well-circumscribed hyporeflective spaces within the fovea, measuring at least 10 μm in diameter. 2 Fundus-related MP was performed using the SD-SLO/OCT. A 4-2-1 double staircase strategy was used and results were reported in decibels. The recorded fixation pattern was classified according to the Fujii classification. 10 Retinal sensitivity in the 8° central area and stability of fixation were measured at each visit.
Statistical analysis was performed using the Statistical Package for Social Sciences (version 17.0; SPSS, Chicago, IL). Intragroup changes were compared by repeated measures analysis of variance with Dunnett correction for multiple comparisons. Fisher's exact test was used to compare the retinal sensitivity (RS) between eyes that showed an anatomical improvement and the control group at each follow-up visit. Results were considered significant if the P value was <0.05. Data at baseline, month 3, month 6, and month 14 are presented.
Results
In the treatment group, the 20 patients (9 women and 11 men; 20 eyes) had a mean age of 63.6 ± 3.1 years. In the control group, the 20 patients (9 women and 11 men; 20 eyes) had a mean age of 62.2 ± 3.4 years. The characteristics of the 40 patients in the 2 groups at baseline are given in Table 1. No differences were present at baseline between the 2 groups with respect to sex, age, mean duration of diabetes, actual HbA1c percentage and HbA1c percentage in the last 5 years, microalbuminuria, and blood pressure.
SD, standard deviation; Hb
During follow-up, no statistically significant difference was present between the 2 groups with respect to HbA1c percentage, blood pressure, and microalbuminuria (Table 2).
BCVA, best corrected visual acuity; ETDRS, early treatment diabetic retinopathy study; CRT, central retinal thickness; MP, microperimetry; ΔP, statistical significance compared with baseline; Δ2P, statistical significance compared with the treatment group.
In the treated group, BCVA and mean RS reduced during follow-up, but without statistical significance (P > 0.05 at months 3, 6, and 14). Five eyes (25%) showed disappearance of the retinal cysts after a mean time of 3.5 ± 0.3 months, and the anatomic improvement persisted during the following months (Figure 1). When compared with the control group, these 5 eyes showed no statistically different mean BCVA (76.78 ± 4.1 at baseline, P = 0.9; 76.11 ± 4.1 at month 3, P = 0.8; 76.78 ± 4.5 at month 6, P = 0.8; 76.15 ± 5.2 at month 14, P = 0.6) but an improved mean RS (16.24 ± 0.31 at baseline, P = 0.8; 16.24 ± 0.49 at month 3, P = 0.01; 16.32 ± 0.46 at month 6, P < 0.001; 16.43 ± 0.39 at month 14, P < 0.001). Two eyes (10%) showed an increase of retinal edema during follow-up, associated with visual loss and reduction of RS (P > 0.05). In the remaining 13 eyes (65%), BCVA, CRT, and RS did not show any significant change during follow-up (P > 0.05).
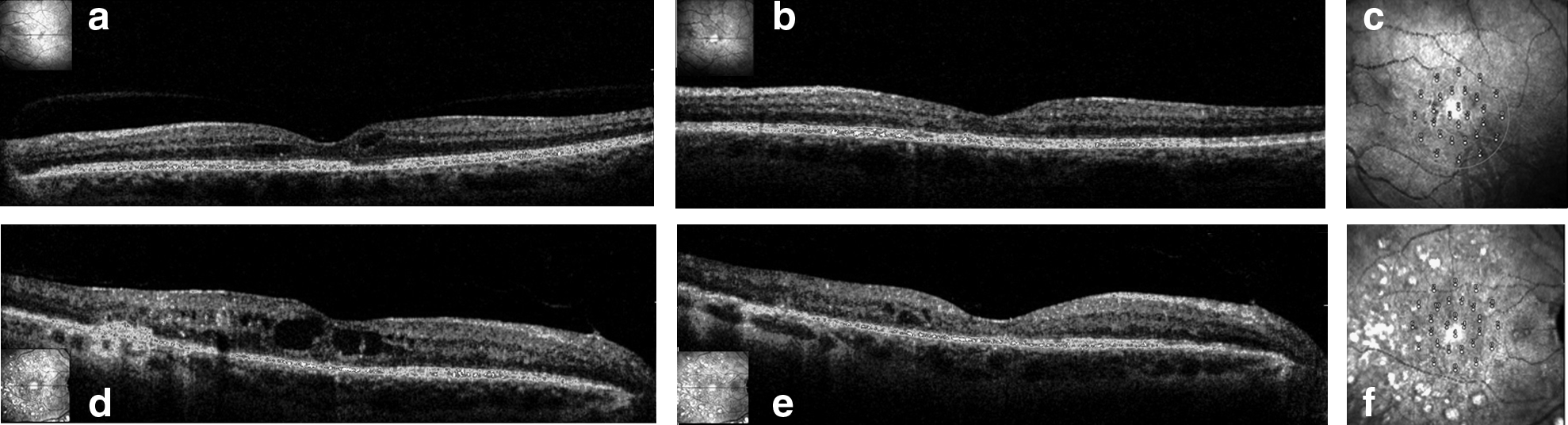
Diabetic CME without macular thickening treated with an orally administered combination of flavonoids, Centella asiatica, and Melilotus. At baseline,
In the control group, no improvement of BCVA and CRT was observed during follow-up, worsening was observed in 5 eyes (25%, P > 0.05), and stabilization was observed in the remaining 15 eyes (75%). Mean RS showed a reduction during follow-up (P = 0.08 at month 3; P < 0.001 at months 6 and 14).
No differences in BCVA, mean CRT, and stability of fixation between the 2 groups were observed during follow-up (P > 0.05), whereas a greater RS was present in the treated group at month 14 (P = 0.01).
Discussion
In this prospective, interventional, controlled study, we evaluated the effects of the orally administered combination of flavonoids, C. asiatica, and Melilotus on diabetic CME without macular thickening during 14 months of follow-up. To our knowledge, no previous reports have focused on this issue. CME without macular thickening has been recently reported by Jun et al. in 5.6% of eyes of 653 patients affected by different retinal pathologies. 2 Among them, nonproliferative diabetic retinopathy without significant macular edema was present in 27% of cases.
While mean BCVA, CRT and fixation stability did not show significant differences between the 2 groups during follow up, at 14-month follow up visit the treated group showed a greater RS (P = 0.01). Reduction of RS was significant in the control group only, at month-6 and at month-14 (P < 0.001). Moreover, 5 eyes in the treated group showed a disappearance of the intraretinal cysts, which persisted during follow up and was associated with a significant improvement in RS at each follow up visit when compared to control group. On the other hand, no eye in the control group showed an anatomical improvement. Anatomic and functional improvement in the treated group could reflect the beneficial effects of the treatment, mostly in consideration that no significant differences were observed between the 2 groups as concerns changes of HbA1c percentage, microalbuminuria and blood pressure during follow up. Flavonoids have showed to improve endothelial cells function, to have an antivascular endothelial growth factor effect and to increase release of fibrinolytic agents.3–5,11 In a prospective controlled evaluation of patients with retinal vein occlusion, Glacet-Bernard et al. showed that troxerutin could improve visual acuity, retinal circulation times and macular edema. 12 Flavonoids act by inhibiting leukocyte activation, rolling, adhesion, and migration.13–15 The fresh Melilotus plant contains a glycoside (melilotoside) which releases glucose and coumaric acid during the drying process. From the latter 0.4%–0.9% is transformed into coumarin. Previous studies showed that coumarin has anti-inflammatory properties by suppressing the phosphorylation of protein kinase B. 16 The beneficial effects on RS and the disappearance of intraretinal cysts could be related to the combination of anti-inflammatory effect and reduction of endothelial cells permeability.
Despite the beneficial effects on RS, the treated group did not show significant differences with the control group with respect to BCVA and fixation stability. Visual acuity depends on the foveal area, whereas MP tests the RS in a larger area surrounding the fovea. Focal alterations may affect visual acuity and light sensitivity reduction more than diffuse edema,17,18 as they block the light from photoreceptors even before establishment of a structural damage to the retina. Therefore, intraretinal cystoid spaces could determine a functional impairment even in the absence of retinal thickening. Small anatomic changes due to disappearance of the retinal cysts could more easily reflect in an improvement of RS rather than in a gross improvement of visual acuity.
A limitation of this study is the relatively small sample size in the 2 groups, mainly because of the prospective design. On the other hand, major strengths are the prospective nature, standardization of data collection, and length and high rate of follow-up. In view of the unexpected functional benefits in the treated group, this study represents a pilot study for a much larger trial aiming to definitely address whether a combination of flavonoids, C. asiatica, and Melilotus is beneficial in preserving RS in diabetic CME without macular thickening.
In conclusion, diabetic CME without retinal thickening showed to affect RS in the long term, with no significant visual and anatomic changes detected. Therefore, MP could represent a better diagnostic tool than visual acuity alone to detect functional changes during follow-up. This prospective pilot study suggests a beneficial role of the orally administered combination of flavonoids, C. asiatica, and Melilotus for functional preservation in case of diabetic CME without retinal thickening.
Footnotes
Acknowledgment
A grant was received by Aesculapius-Bs S.r.l. in support of this study.
Author Disclosure Statement
Proprietary interest: none.