
Abstract
Abstract
Purpose:
To determine whether topically applied brimonidine affects the retinal hemodynamic autoregulatory response to posture change in patients with normal tension glaucoma.
Methods:
Six patients with normal tension glaucoma (primary open-angle glaucoma and maximum untreated intraocular pressure <22 mmHg) in each eye were studied. We retrospectively reviewed retinal hemodynamic data acquired when the patients were off and on treatment with brimonidine 0.15% (twice a day, both eyes) during the course of their care. At each testing session, vessel diameter and blood speed at the same site along the inferior temporal retinal artery of 1 eye were measured while sitting, while reclining for 30 min, and again while sitting using a retinal laser Doppler instrument. Blood flow was computed automatically. Brachial artery blood pressure and heart rate were also measured. The Wilcoxon signed rank test was used to assess the statistical significance of the differences in each measured parameter while subjects were on and off brimonidine.
Results:
Off brimonidine, the mean blood flow rate increased by 68.0%±34.3% (range: +17% to +108%) after 30 min in reclined posture compared to baseline-seated measures. On brimonidine, the mean blood flow rate increased by 8.9%±16.8% (range: −9.7 to +28.0%) after 30 min in reclined posture compared to baseline-seated measures. The difference in the posture-induced changes for blood flow rate while on brimonidine compared to off brimonidine was statistically significant (P=0.027).
Conclusions:
Off brimonidine, the patients exhibited marked increases in retinal blood flow while reclining. On brimonidine, the hemodynamic changes were consistent with normal autoregulatory control of retinal blood flow.
Introduction
While it is unclear if co-regulation of intraocular pressure (IOP) and ocular blood flow optimizes POAG management, collectively randomized clinical trial data indicate that lowering IOP with medicine, laser, or surgery slows, but does not completely prevent, conversion to disease or disease progression.2–4 Several investigators have postulated that wide fluctuations in retinal blood flow with positional change may produce ischemia–reperfusion injury to the retina, leading to retinal ganglion cell loss and axonal degeneration, hallmarks of glaucomatous optic neuropathy.5–9 In addition, a link between vascular dysregulation and disc hemorrhage (DH) in POAG has been suggested although the exact mechanism of DHs is not clear. 10 If DH is a marker of vascular dysregulation in POAG, then the evidence that DH is a risk factor for conversion from ocular hypertension to POAG 11 and for progression of pre-existing disease12–16 suggests that normalization of blood flow regulation may reduce glaucomatous progression.
Brimonidine is an alpha2 adrenoceptor agonist that when applied topically in either the 0.15% or 0.2% formulation achieves a vitreous level that interacts with vascular endothelial alpha2 receptors17,18 to produce vasomotor effects. 19 The results from the Low-pressure Glaucoma Treatment Study reported by Krupin et al. 20 showed that twice-daily treatment with topical brimonidine tartrate 0.2% preserves visual field better than treatment with topical timolol maleate 0.5% in open-angle glaucoma patients with statistically normal IOP. The authors concluded that this finding is consistent with a non-IOP-related mechanism of action favoring brimonidine-treated patients.
In this retrospective study, we assessed the effect of brimonidine on retinal vascular autoregulation in 6 patients with normal tension glaucoma (NTG)—1 who converted to glaucoma at an IOP of 10 mmHg and 5 others with progressive disease despite IOP in the mid-teens.
Methods
Patients
The Institutional Review Board at Massachusetts Eye and Ear Infirmary approved this retrospective study. The research followed the tenets of the Declaration of Helsinki. Each patient had been followed at the Glaucoma Service of Massachusetts Eye and Ear Infirmary for NTG by one or another of the authors (L.R.P. or C.L.G.). All had undergone the retinal vascular autoregulation testing protocol described below on 2 occasions, once while untreated (n=4) or treated with agents other than brimonidine (n=2, latanoprost and timolol for one subject and bimatoprost monotherapy for the other), and again while treated with only brimonidine (n=5) or treated with brimonidine added to pre-existing treatment (n=1; latanoprost and timolol). Hemodynamic data on 3 of these 6 patients while not treated with brimonidine had been reported previously 1 : 2 of those subjects were untreated and 1 was treated with bimatoprost. The duration of brimonidine treatment before testing in the 6 patients ranged from 1 month to 5 months. Each patient had no signs of secondary glaucoma on slit lamp examination, open angles on gonioscopy, and a known maximum untreated IOP of <22 mmHg in both eyes using Goldmann applanation tonometry. Table 1 shows the demographic and ocular characteristics for each patient.
C, Caucasian; AA, African American; OS, left eye; OD, right eye; VA, Snellen Visual Acuity; C/D ratio, Cup-to-Disc ratio; MD, Humphrey 24–2 full-threshold visual field mean deviation; PSD, Humphrey 24–2 full-threshold visual field pattern standard deviation.
Testing protocol
The testing procedures were the same as those we have described previously. 1 On the day of the testing visit, we measured IOP in both eyes by Goldmann applanation tonometry or by using a Tono-Pen XL applanation tonometer (Medtronic, Jacksonville, FL). Mydriasis was achieved by instilling 1 drop of tropicamide 1% in the study eye. A baseline measurement of the brachial artery blood pressure in the left arm along with the heart rate (HR) was made using a Keller Vital Signs Monitor (Keller Medical Specialties, Antioch, IL) after the subject was seated for 15 min. Baseline OPP was estimated using the standard formula: OPP=2/3 mean brachial arterial blood pressure (MAP) −IOP. The factor two-thirds adjusts for the decline in blood pressure between the brachial and ophthalmic artery with the subject sitting. 21 The Canon CLBF 100 Laser Blood Flowmeter (Canon, Inc., Tokyo, Japan) allowed us to measure the arterial blood column diameter and centerline blood speed. 22 The blood flow rate is automatically calculated as the product of the cross-sectional area of the artery at the measurement site and the average blood speed, assuming a circular arterial cross section. 22 We selected a vascular segment from the inferior temporal retinal artery just below the optic disc margin for baseline measurements. This measurement site was chosen because evidence suggests that the inferior neuroretinal rim often is involved in early glaucoma. 23
As we previously described, 1 after the baseline measurements in the seated position, the subjects reclined on their right side with their head supported by a wedge making a 24° angle with the horizontal. Subjects maintained this position for approximately 30 min while blood pressure and HR were measured automatically in the left arm at 5-min intervals. In this position, OPP was estimated using the experimentally derived formula: OPP=MAPreclining −IOPreclining, where MAPreclining is the mean brachial artery blood pressure measured in the left arm with the subject reclining on the right side. 24 As in our previous study, 1 we estimated that IOPreclining was 3 mm Hg higher than the IOP measured at baseline with the patients seated. We obtained laser Doppler measurements from the same artery selected for the baseline measurements after approximately 15 and 30 min in the right lateral decubitus position using a specially designed headrest. We elected to maintain patients in this position for 30 min to make certain that hemodynamics were measured during an equilibrium state. Prior work21,25 indicates that at least 5 to 8 min are needed for the retinal vasculature to adjust to an altered OPP. Finally, we repeated measures of blood pressure, HR, and laser Doppler measurements approximately 20 min after the patients arose to the sitting position. Each testing visit began at approximately 10:00 AM.
Statistical analysis
Results obtained after approximately 30 min of reclining were used for comparisons with the baseline seated measurements. The Wilcoxon signed rank test was used to assess the statistical significance of the differences in each measured parameter while subjects were treated with brimonidine compared to while untreated or treated with agents other than brimonidine.
Results
As shown in Table 2, there were no significant differences in IOP, OPP, MAP, or HR in the patient group measured at baseline with the subjects seated while treated with brimonidine compared to while untreated or treated with agents other than brimonidine. Table 3 shows the baseline values of the diameter of the inferior temporal retinal artery, the average blood speed in the artery, and the blood flow rate through the artery in each subject while seated, both off and on brimonidine. As indicated in the table, there were no significant differences in these parameters with patients on brimonidine compared to off brimonidine.
Wilcoxon signed rank test.
IOP, intraocular pressure; MAP, mean brachial arterial pressure; OPP, ocular perfusion pressure; HR, heart rate; SD, standard deviation.
Wilcoxon signed rank test.
Figure 1 shows the percentage changes from baseline while seated in both OPP and in blood flow rate for Patient No. 6 during the course of the 2 testing sessions. During the first session, while untreated, OPP increased by 24% when the patient reclined for 30 min. The patient was then treated with brimonidine 0.15% (twice a day, both eyes) and returned 2 months later. During this second session, the change in OPP was similar, an increase of 30% while the patient was again reclining for 30 min. While untreated, the blood flow rate in the inferior temporal retinal artery of the left eye increased by 106% when the patient reclined for 30 min. As shown, while treated with brimonidine, the blood flow rate at the same measurement site remained essentially constant, increasing by only 3%, while the patient was again reclining for 30 min.
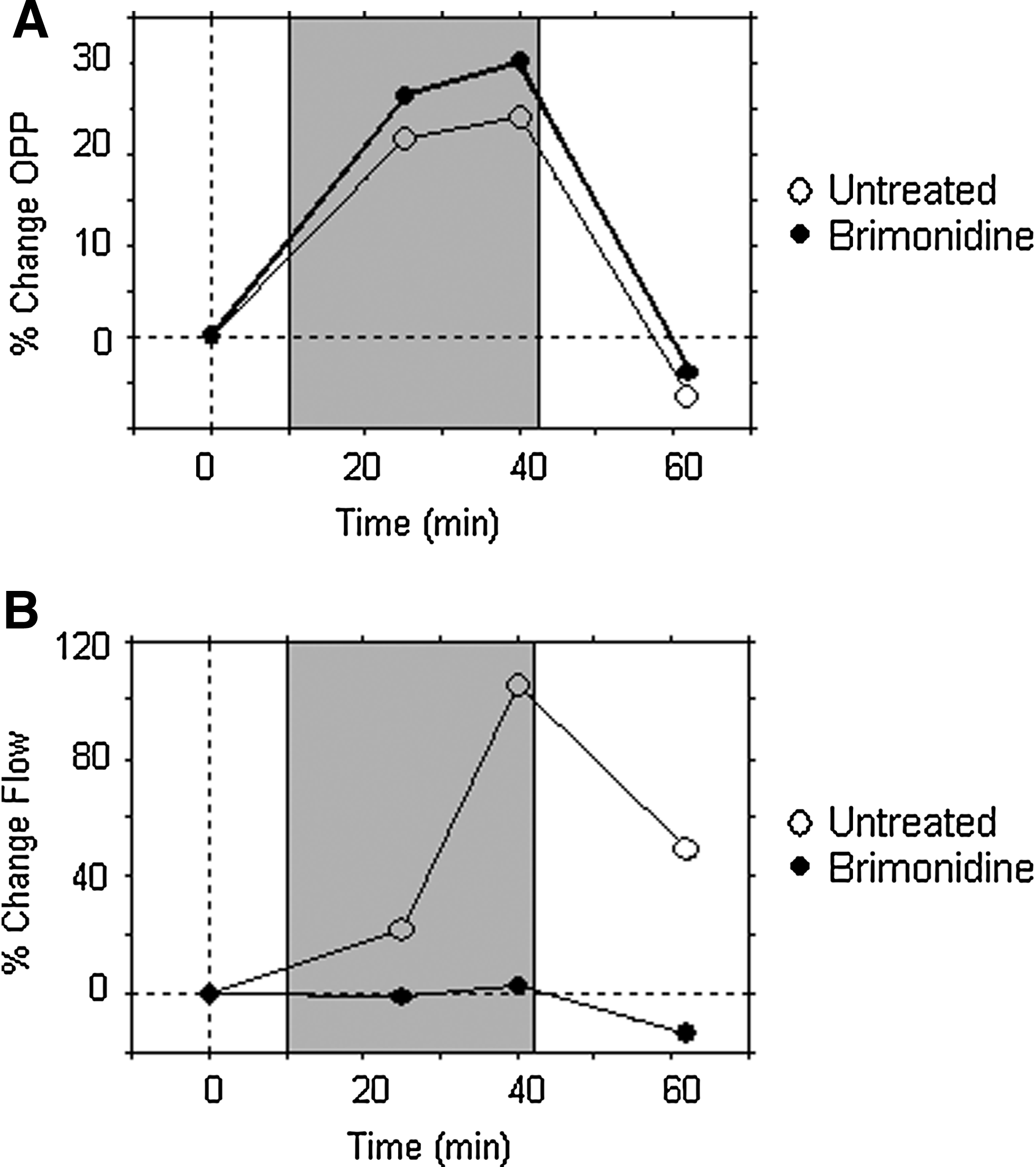
The percentage change from baseline seated in the ocular perfusion pressure
Off brimonidine, the mean seated baseline retinal blood flow in the 6 patients was 7.8±2.4 μL/min (mean±standard deviation). The blood flow while reclining after 30 min was 12.7±3.6 μL/min. The average increase in OPP was 15.7%±9.4%. The difference between the baseline seated blood flow and the blood flow while reclining was significant (P=0.028). With the patients on brimonidine, the blood flow at baseline seated was also 7.8±1.9 μL/min. The blood flow while lying down after 30 min, however, was 8.4±2.0 μL/min. This difference between seated and reclined values while on brimonidine was not significant (P=0.25). The average increase in OPP while reclining with the patients on brimonidine was 28.1%±26.7%, which was not significantly different (P=0.46) from the increase while off brimonidine.
Table 4 shows the percentage changes in the diameter of the inferior temporal retinal artery, the blood speed in the artery, and the blood flow rate through the artery in each of the 6 patients while reclining compared to sitting while off and on brimonidine. The percentage changes in both blood speed and blood flow rate decreased while on brimonidine compared to off brimonidine in each subject. Treatment with brimonidine resulted in a significant (P=0.027) decrease in the changes in both blood speed and blood flow rate while reclining compared to sitting.
Wilcoxon signed rank test.
Discussion
The results of this study show that IOP, MAP, OPP, HR, as well as retinal arterial diameter, blood speed, and blood flow rate measured in the study patients while they were seated were not significantly different while under treatment with brimonidine compared to while untreated or under treatment with agents other than brimonidine. However, while the subjects were reclining, substantial differences in blood speed and blood flow were noted when the patients were under brimonidine treatment compared to no treatment or treatment with agents other than brimonidine. Off brimonidine, there was, on average, a substantial increase in the retinal blood speed while reclining (65.0%±28.0%); yet, while on brimonidine, the increase in blood speed was significantly less (22.8%±23.1%, P=0.027). The change in retinal blood velocity while reclining for 30 min when using brimonidine was comparable to the change we previously reported in untreated healthy subjects (24.6%±10.8%). 1 Finally, off brimonidine, the blood flow rate itself increased by 68.0%±34.3% while reclining, indicating a lack of blood flow autoregulation in the retinal vasculature. On brimonidine, the increase in blood flow rate while reclining compared to sitting was only 8.9%±16.8%, significantly less (P=0.027) than the value obtained off brimonidine, and again similar to that previously measured in untreated healthy subjects (6.5%±12.0%). 1 These results thus suggest that brimonidine normalizes the retinal vascular autoregulatory response to increased OPP due to posture change.
In a healthy retinal vasculature, an arterial constriction in response to a locally elevated blood pressure is expected. The brimonidine-related constriction of 5.3%±5.8% is not only similar to our earlier finding in healthy subjects (7.5%±3.4%), but also to the constriction of 6.6%±2.8% reported by Tachibana et al., 26 who also studied a group of healthy subjects while reclining on their right side compared with sitting. The lack of constriction while reclining while not using brimonidine indicates an altered myogenic tone in the retinal vasculature. 27 The mechanisms by which brimonidine restores myogenic tone are not known. It has been shown experimentally, however, that brimonidine can produce either retinal arteriolar dilation or constriction, and that the magnitude of vasoconstriction increases with increasing brimonidine concentration. 19 Furthermore, Kent et al.17,18 have shown that clinical dosing of the topical formulation of brimonidine results in concentrations in the human vitreous that are sufficient for pharmacologic activity at alpha-2 adrenergic receptors.
The presence of elevated retinal blood speed and blood flow rate while off brimonidine is also indicative of altered myogenic tone in arterioles distal to our measurement sites. A healthy retinal vasculature constricts just enough to maintain a steady blood flow rate in the face of an increase in the local blood pressure. The mechanisms underlying this autoregulatory response are under study. Experimental evidence has shown that the vascular dysregulation in glaucoma patients extends outside of the eye 28 and involves systemic abnormalities in vascular endothelial function,29–36 and autonomic function.37–39
Our finding that baseline values of the inferior temporal retinal artery diameter, average retinal arterial blood speed, and arterial blood flow rate while seated were not significantly different with or without brimonidine treatment are consistent with earlier reports. Both Schmidt et al. 40 and Inan et al. 41 used color Doppler ultrasound and reported no differences in the circulatory parameters in the central retinal artery in POAG patients before and after brimonidine treatment. Other studies reported that brimonidine treatment did not alter intraretinal circulatory parameters in ocular hypertensive patients 42 or in healthy volunteers. 43
A major question to be addressed is whether the normalization of the retinal vascular autoregulatory response to simple posture changes in glaucoma patients translates to preserved visual function. The results of the Low-pressure Glaucoma Treatment Study 20 suggest that this may indeed be the case. Those results showed that patients randomized to monotherapy with brimonidine were statistically less likely to have progressive visual field loss than patients randomized to monotherapy with timolol, even though both treatments had similar IOP lowering effects. Furthermore, there are other reports suggesting improvements in visual field 44 and in contrast sensitivity 45 in glaucomatous eyes after brimonidine treatment.
The limitations of this study are its retrospective nature, the small sample size, the wide range of glaucoma damage exhibited by our patients, and the nonuniform range in the duration of brimonidine treatment before testing. Nevertheless, each patient served as their own control and the results were statistically significant. We need to point out, however, that while we found no statistically significant differences in MAP and OPP in the patients off and on brimonidine, it is likely that the 5.3% decrease in MAP while on brimonidine might be significant in a larger group of patients. Brimonidine is known to decrease systemic blood pressure. 46 A decrease in MAP, if sufficiently large, also decreases the OPP. As recently reviewed by Leske, 47 population-based epidemiologic studies have found strong relationships between low OPP and the prevalence and incidence of POAG, and other studies report similar associations between low OPP and POAG progression. Thus, the benefits of improving the retinal hemodynamic autoregulatory response to posture change with brimonidine may be offset by decreased OPP. The Low-Pressure Glaucoma Treatment Study, 20 however, suggests that the benefits associated with an improvement in retinal vascular autoregulation may outweigh any risks associated with decreased OPP on brimonidine treatment. Of course, this assumes that retinal vascular dysregulation would be present in a significant number of patients in that study as well.
In conclusion, we have shown that topically applied brimonidine improves the retinal hemodynamic autoregulatory response to posture change in NTG patients. We cannot rule out, however, that other topical agents may also improve retinal vascular autoregulaton. Venkataraman et al. 48 have reported an improvement in retinal vascular reactivity to hypercapnia after dorzolamide treatment in patients with POAG. It is our intention is to conduct a prospective study of the effect of brimonidine as well as other topical agents on retinal vascular autoregulation in POAG patients.
Footnotes
Acknowledgments
This work was supported by a Research to Prevent Blindness Award and the Margolis Fund (both to Dr. Pasquale) and by the Harvard Glaucoma Center for Excellence. Dr. Pasquale has received research funding from Allergan, Inc. on healthcare economics research, but no pharmaceutical company sponsored this investigator-initiated research. The Glaucoma Service at Massachusetts Eye and Ear Infirmary is a recipient of a Horizon Grant from Allergan, Inc.
Author Disclosure Statement
The authors report no financial or any other conflict of interest related to the contents of the material within this article.