
Abstract
Abstract
Purpose:
To assess the safety and feasibility of a moxifloxacin-loaded punctum plug (MP) in 2 groups of cataract patients.
Methods:
Two prospective, single-arm, Phase I studies were conducted with 20 cataract patients (10 per study) at the Singapore National Eye Center. After cataract surgery, the MP was inserted into the punctum, and follow-up assessments were conducted at 1 h, 24 h, and on days 3, 7, 10, 20, and 30. Study endpoints included MP retention, ease of placement, and moxifloxacin concentrations in the tear fluid. Moxifloxacin concentrations were targeted to be ≥250 ng/mL through 7 days, with detectable levels through day 10. After the course of therapy, the plug would resorb and be absent from the punctum by day 30. Slit lamp evaluations were performed, and intraocular pressure measurements were performed on days 1, 3, 7, 10, 20, and 30. Patients were queried for the presence or absence of several ocular sensations in the operative eye. Due to the variability in tear film antibiotic concentrations observed in the first study, a second study was conducted with more stringent concomitant drop administration and tear sample collection criteria.
Results:
MP retention in the punctum was 95% (19/20) through day 10, and all plugs were absent at day 30. Average moxifloxacin concentrations in the tear film ranged from 155 to 785 ng/mL for Study 1 and 2,465 to 3,236 ng/mL for Study 2 through day 7. These values were above the target of 250 ng/mL for all time points except for day 1 of Study 1. For both studies, moxifloxacin concentrations in the tear film were above detectable levels at day 10. The plugs were well tolerated, and there were no adverse events as defined by the protocol, and no ocular complaints or findings other than normal post-cataract symptoms.
Conclusions:
The MP delivered and maintained moxifloxacin tear fluid concentrations at therapeutic levels above the MIC90 values for common susceptible conjunctivitis pathogens for 7 days (Study 2). The MP also exhibited a favorable safety and tolerability profile and, hence, may be a viable alternative to topical antibiotic drops for the treatment of bacterial conjunctivitis.
Introduction
It is well known that antibiotic treatment shortens the recovery time for bacterial conjunctivitis. 5 Quicker recovery time translates into reduced absence from school for children, and less time off from work for patients and their caregivers. Treatment with antibiotics, such as fourth-generation fluoroquinolones, can reduce contagion in cases of bacterial conjunctivitis, and, thus, the length of exclusion from school to as little as 24 h. 4
Endophthalmitis caused by bacterial contamination is a rare but potentially sight-threatening complication of cataract surgery. There are indications that the rates of endophthalmitis may be higher in the past few years than were reported historically. 6 One survey of the literature found endophthalmitis rates of 0.158% in the 1980s, 0.087% in the 1990s, and 0.265% in the 2000–2003 time period. 6 This increase appears to coincide with the advent of sutureless clear corneal cataract surgery. 6 The 2007 ASCRS survey found that approximately 90% of respondents had an infection rate of 0.1% or lower. 7 However, 10% of the members who responded reported endophthalmitis rates of 0.2% or higher. It appears that Gram-positive bacteria are most often the culprits causing post-cataract endophthalmitis. 8 The use of topical antibiotics such as moxifloxacin and gatifloxacin for surgical prophylaxis and treatment is currently the standard of care, but is off-label.9,10 Due to the large numbers of patients required to demonstrate efficacy for the prevention of endophthalmitis, conducting a clinical trial of this nature is impractical.
Topical fluoroquinolone drops are the most commonly used form of ocular antibiotics today. 7 The Ocular Trust reported that fluoroquinolones, such as moxifloxacin, have a broad spectrum and excellent antibacterial efficacy against organisms that have been isolated from ocular infections. 11 When applied topically, this antibiotic exhibits excellent penetration into the conjunctiva,12,13 cornea, 14 and aqueous humor.14–19 For instance, peak aqueous humor concentrations for moxifloxacin occur within 1 h. 14 Despite its corneal and conjunctival penetration characteristics, moxifloxacin has been shown to exhibit a favorable tolerability and safety profile. 20 Moxifloxacin therapy has been shown to confer a decreased likelihood of selecting for resistant organisms due to a bulky side chain, which inhibits its efflux from the bacteria cell. 21 It is also hypothesized that 2 simultaneous mutations are required by the bacterial organism in order to produce a resistant mutation. 22
There are some limitations to the use of topical drops for ocular infection prophylaxis and treatment. Human and animals studies have shown that concentrations in the aqueous humor can start to decline within 1–2 h due to the turnover of ocular fluids.14,23 This shortcoming may be compounded by poor patient adherence to prescription regimens due to the multiple doses over several days that are required. Studies have shown that antibiotic concentrations can sometimes fall below the MIC90 values for common bacterial species.13,23
A moxifloxacin-loaded punctum plug (MP) (Ocular Therapeutix, Bedford, MA) has recently been developed for the sustained delivery of the antibiotic for the treatment of bacterial conjunctivitis. The MP is a dried polyethylene glycol hydrogel rod that is embedded with moxifloxacin-encapsulated microspheres, which is designed to provide a sustained drug release over a 10-day period. The MP is placed into the punctum, where it swells on contact with moisture and conforms to each individual punctum to occlude the lumen. The MP degrades and is resorbed within 30 days of application. Two separate studies examined the safety and feasibility of the MP to release a sustained amount of drug into the tear film for a predetermined amount of time in patients undergoing cataract surgery. Due to the variability in tear film antibiotic concentrations observed in the first study, the second study was designed with more stringent concomitant drop administration and tear sample collection criteria.
Methods
Design and objectives
This report comprises 2 prospective, single-center, single-arm studies, each involving 10 overall healthy patients who were previously scheduled to undergo cataract surgery.
The purpose of these studies was to assess the safety and feasibility of the MP designed as a sustained ocular drug delivery system for the treatment of bacterial conjunctivitis. Also evaluated were the ease of placement, retention, and the pharmacokinetic characteristics of the MP. The study schedule is shown in Table 1. These studies were approved by the Centralized Institution Review Board, which is a part of SingHealth (Singapore Health Services Group) in Singapore, and all patients were required to provide informed consent before study participation.
Ocular complaints—for example, stinging, discomfort, excessive tearing, etc.
Flushing of the nasolacrimal duct applied to Study 2 only.
MP, moxifloxacin-loaded punctum plug; IOP, intraocular pressure; X, was conducted at that time point.
Endpoints
Study 1
Three endpoints relating to the feasibility of the MP were evaluated. Product performance success was defined as the MP remaining in the canaliculus for a minimum of 10 days and less than 30 days. The concentration of moxifloxacin in the tear fluid was targeted to be above the highest minimum inhibitory concentration (MIC90=250 ng/mL) cited for susceptible strains of H. influenzae, Sta. epidermidis, Str. pneumoniae, Sta. aureus, or N. gonorrhoeae) through 7 days and above detectable levels through 10 days.19,24,25 The MIC90 refers to the antibiotic concentration that inhibits the growth of 90% of the tested bacterial isolates. 26 In addition, data were collected on the product's ease of use in terms of placement of the MP with forceps. The safety evaluations included slit lamp biomicroscopy, intraocular pressure (IOP), and adverse ocular events within 30 days of surgery.
Study 2
MP retention, ease of MP placement, and adverse ocular events were evaluated as per Study 1. Tear fluid concentrations of moxifloxacin were measured concomitant drop administration at 1 h, and at 1, 3, 7, and 10 days after surgery. Tear samples were taken (preferably before 9:30
Inclusion and exclusion criteria
Patients had to meet all of the following criteria to be eligible for participation: ≥21 years of age; had a cataract and were expected to undergo clear corneal cataract surgery; had been informed of the nature of the study and was able to comply with study requirements, visit schedule, and had provided written, IRB approved informed consent.
Patients were excluded from participation if they presented any of the following symptoms: presence of active inflammation and/or active structural change in the iris or anterior chamber in the study eye; presence of congenital or ocular anomaly in the operative eye including anomalies of the punctum, aniridia, and congenital cataract; any abnormality that prevented reliable Goldmann applanation tonometry in either eye; potential best-corrected visual acuity (BCVA) in fellow eye worse than 20/40; active epiphora; presence of a nasolacrimal duct obstruction or a punctum too small to accept insertion of a 0.5 mm diameter MP; tear fluid production not within normal limits as determined by a Schirmer Test; any systemic or ocular disease or disorder, complicating factors or structural abnormality that would have negatively affected the conduct or outcome of the study; active or history of chronic or recurrent inflammatory eye disease, evidence of acute external ocular infections, intraocular infection, uncontrolled and clinically significant dry eye syndrome, evidence of glaucoma or clinical relevant elevated IOP or corneal dystrophy, known or suspected allergy or hypersensitivity to fluoroquinolones or to any component of the study product; routine use of artificial tears; pregnant or lactating women; any medications that may have interfered with or confounded liquid chromatography-mass spectrometry (LC-MS) results. Patients were also excluded from participation if they were participating in any other clinical trial during the follow-up period that could confound the treatment or outcomes of the study.
MP insertion
The MP was placed in the canaliculus at the conclusion of cataract surgery according to the following procedures. The area of the punctum was anesthetized with 2 drops of Minims Tetracaine Hydrochloride 0.5% (Chauvin Pharmaceuticals Ltd., Kingston-Upon-Thames, UK) instilled into the conjunctival sac. If necessary, the punctum was dilated to accept the 0.5 mm diameter MP. Using sterile forceps, the MP was aligned with the punctum opening, gently inserted through the punctum, and pushed into the vertical canaliculus. On exposure with moisture, the MP rapidly hydrates and expands to fill the vertical canalicular cavity. If required, the eye was gently irrigated with balanced salt solution (BSS) solution until the plug was adequately hydrated.
Cataract surgery
Patients were prepared for cataract surgery following standard operative techniques. The cataract surgery was performed according to the standard practice of the investigator. At the end of surgery, and after MP insertion, gatifloxacin was administered into the operative eye. According to routine standard of care, topical steroids and nonsteroidal anti-inflammatory drugs (NSAIDs) were administered. In addition, gatifloxacin drops were prescribed and patient-administered per the investigator's instructions throughout the course of the study. No drops were to be administered within 1 h before tear fluid sampling in Study 1. In Study 2, patients were not allowed to administer concomitant drops after midnight and until after the first tear fluid collection in the morning. Topical moxifloxacin was not allowed during the studies. MP retention was monitored using B scan ultrasound on days 1, 3, 7, 10, 20, and 30. At any point during the study, if the subject was experiencing discomfort due to the MP or if the hydrogel plug was still present at the day 30 visit, the plug could be flushed out.
Tear sample collection
A polyester rod was placed in the inferior lateral conjunctival fornix to collect the volume of tears required for analysis. During tear sampling, care was taken to avoid irritating the ocular surface and eyelid margin. Ambient light was used to stimulate tear production. Tears were collected for approximately 1 min. Samples were immediately frozen on collection and shipped frozen for analysis. Tear samples were evaluated for moxifloxacin using LC-MS. An internal interference validation study was conducted to confirm that gatifloxacin did not interfere with the moxifloxacin assessment by LC-MS/MS in human tear fluid.
Solicited postoperative ocular queries
At each follow-up study visit, patients were queried for the presence or absence of each of the following sensations in the operative eye: excessive tearing, photophobia, foreign body sensation, stinging/burning, itching, discomfort, and others. Positive responses to the standardized queries were not reported as adverse ocular events unless (1) the event met the criteria of a specific event as described in the protocol, (2) was outside of normal limits for the post-cataract surgical period observed, (3) did not respond to standard medical therapy (eg, medication change), or (4) was associated with clinical sequelae (eg, adverse slit lamp examination findings).
Statistical analyses
Study data were documented using summary tables and patient data listings. Continuous variables were summarized using descriptive statistics, specifically the mean, median, standard deviation, minimum, and maximum. Categorical variables were summarized by frequencies and percentages. No formal sample size estimations were performed, as these were feasibility studies. Statistical analysis of the data was performed using Microsoft Excel.
Results
Demographics and punctum characteristics
The majority of patients were men of Chinese ethnicity (Table 2). The average punctum size was 0.6 mm for both studies (Table 3). The MP was placed in either the inferior or superior punctum of the operative eye.
SD, standard deviation.
MP retention and ease of use
MP retention was 95% (19/20) through day 10 (Table 4). All plugs were absent at day 30 for both studies. In the first study, ultrasound analysis indicated that the plug was still present at day 30 in 2 patients. However, on flushing, it was determined that the plugs were actually absent. In the second study, B-scan ultrasonography could not detect 1 plug on days 7 and 10. However, tear fluid testing showed that moxifloxacin was still being delivered to the tear film during that time, indicating that the plug was still present. On completion of the 2 studies, it was determined that B-scan ultrasonography was not a reliable method for determining whether the plugs were present or absent.
Based on the ultrasound assessment, in 1 patient starting at the day 7 visit, the MP was not present. However, based on the moxifloxacin levels detected in the tear samples for this subject, it was demonstrated that the MP was present for this subject at the day 7 and day 10 visit.
Based on the ultrasound assessment, in 2 cases at the day 30 visit, the plug was present. However, on flushing, it was demonstrated that the plug was no longer present for these 2 cases.
For Study 1, the investigator rated the product as “easy” to use for 50% (5/10) and as “difficult” to use in 50% (5/10) of the cases. In Study 2, the investigator rated the MP as “easy” to use for 90% (9/10) of cases and as “difficult” to use in 10% (1/10) of the cases. For the one case rated “difficult,” the first MP had to be discarded due to an unsuccessful insertion attempt, primarily due to the subject's punctum anatomy, and a second MP had to be used.
Moxifloxacin tear fluid concentrations
The average concentrations of moxifloxacin for Study 1 were above 250 ng/mL at 1 h, day 3, and at day 7 (Table 5; Fig. 1). The average and median concentrations of moxifloxacin for Study 2 far exceeded the target of 250 ng/mL for all times points up to and including day 10 (Table 6; Figs. 2 and 3). Moxifloxacin concentrations were below detectable limits for both studies on day 20 and day 30.
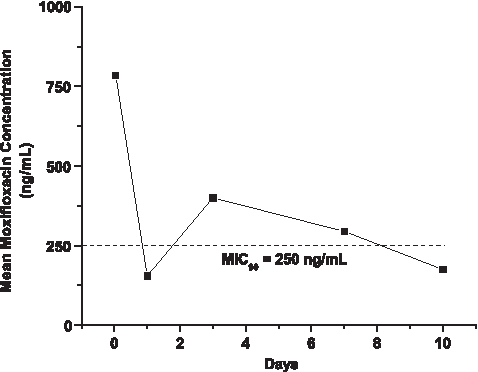
Mean moxifloxacin tear fluid concentrations for Study 1. The dashed line represents the target MIC90 concentration of 250 ng/mL. Time points were 1 h, day 1, day 3, day 7, and day 10. MIC, minimum inhibitory concentration.
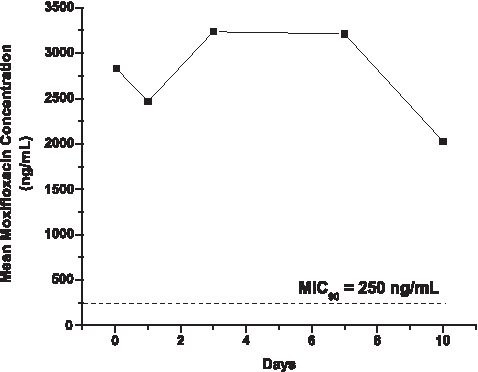
Mean moxifloxacin tear fluid concentrations for Study 2. The dashed line represents the target MIC90 concentration of 250 ng/mL. Time points were 1 h, day 1, day 3, day 7, and day 10.
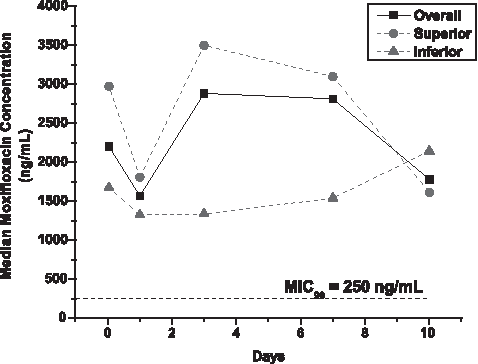
Median moxifloxacin tear fluid concentrations for Study 2. The dashed line represents the target MIC90 concentration of 250 ng/mL. Time points were 1 h, day 1, day 3, day 7, and day 10.
LOQ was defined as 1 ng/mL.
Safety results, IOP results, slit lamp examination findings, and ocular query results
There were no adverse events reported for either study. No deaths, serious adverse ocular events, or other significant adverse ocular events were reported for either study (as defined in the protocol). Mean IOP values ranged from 13.6 to 17.1 mm Hg for Study 1 and 12 to 16 mm Hg for Study 2 (Table 7). The most common findings on slit lamp examination for both studies were aqueous chamber cells and corneal staining/erosion, both of which were determined to be related to cataract surgery (Table 8). All of the findings were graded as trace to mild with 1 exception (1 moderate grade of aqueous chamber cells on day 3 of Study 1). The most common sensations (also cataract surgery-related) reported by patients were itching, foreign body sensation, and excessive tearing (Table 9). None of the canaliculi that had received the MP developed a canalicular/nasolacrimal duct obstruction during the study period.
At each study follow-up visit, patients were queried for the presence or absence of each of the following sensations in the operative eye. Total number of patients for each study was 10.
Discussion
Moxifloxacin is a potent fluoroquinolone antibiotic that possesses a broad spectrum of activity against bacterial species such as those known to cause conjunctivitis.1,9,11,27,28 The efficacy of this agent has been demonstrated in both in vitro and in vivo model systems. For example, moxifloxacin achieved a 3-log reduction in bacterial counts at 2 h for cultured Str. pneumoniae and 15 min for H. influenzae from bacterial conjunctivitis isolates. 29 Moxifloxacin is also shown to inhibit bacterial growth in large zones on culture plates containing Sta. aureus. 30 This antibiotic was found to be effective for prophylaxis and treatment of bacterial keratitis in rabbit models.31,32 Moxifloxacin also prevented Sta. aureus and methicillin resistant Sta. aureus experimental endophthalmitis in rabbits.33–35 However, it should be noted that resistance to moxifloxacin, and other fluoroquinolones can occur through mutations in genes such as gyrA, gyrB, and parC.36,37
Human clinical trials have demonstrated the efficacy of topical moxifloxacin 0.5% for the treatment of bacterial conjunctivitis. Two randomized, double-masked, multicenter, Phase III studies reported clinical cure rates on day 5–6 of 66%–69%. 9 Another multicenter study was conducted to evaluate the speed of clinical efficacy of topical moxifloxacin for the treatment of bacterial conjunctivitis. 38 The majority of eyes (81%, 35/43) obtained a clinical cure, defined as the complete resolution of all ocular signs and symptoms, by 48 h. Only 2.3% (1/43) of the eyes treated with moxifloxacin did not respond within this same time period.
The on-label course of therapy for treatment of bacterial conjunctivitis is moxifloxacin 0.5% solution administered thrice a day for 7 days. 9 The Moxifloxacin Punctum Plug, once in position, is designed to provide an initial “burst” of moxifloxacin, followed by a sustained release of the drug over the course of 10 days. This provides an advantage in terms of reducing the complexity of the therapeutic regimen and eliminates the chance of missed doses.
The pharmacokinetic profile of moxifloxacin delivered from the hydrogel punctum plug was measured in a canine model. 39 The MP was placed in the vertical canaliculus, and tear samples were taken over a period of 15 days. Moxifloxacin concentrations were analyzed by high-performance liquid chromatography/MS. This study demonstrated both the immediate and sustained release of moxifloxacin following administration of the punctum plug. The antibiotic concentrations found in the tear fluid exceeded the measured in vitro activity against many clinical ocular isolates. 27 The sustained release of moxifloxacin from the plug provided both elevated drug concentrations and time above the MIC90 values, which are necessary to achieve bacterial kill for organisms such as susceptible Sta. aureus, Str. pneumoniae, and Haemophilus sp.26,40
The human clinical trials found that the punctum plug was rated “as easy to use” much more frequently in Study 2 than for Study 1. This may have been due to the investigator's increased experience with inserting the MP as the dimensions, insertion method, and other study parameters remained the same in both studies.
The retention of the Moxifloxacin Punctal Plug was high at day 10 (95% 19/20) in the 2 studies. Therefore, the plug was in the proper position to deliver moxifloxacin to the tear film over the course of 10 days. As previously mentioned, the B scan ultrasonography assessment indicated the MP was still present in 2 patients at the day 30 visit. However, on flushing, it was demonstrated that the plugs were in fact absent for these 2 cases. Therefore, resorption of the MP was considered to be complete in 100% (20/20) of patients at day 30. These results demonstrated that the punctum plug was retained in the canaliculus for the desired period of time.
Study 1 indicated that moxifloxacin concentrations were sustained in the tear film over the course of 10 days. Study 2, which was designed with more stringent criteria in regard to concomitant drop administration and tear collection, showed higher mean concentrations of moxifloxacin than Study 1. In addition, the moxifloxacin levels were less variable in Study 2. The tear film concentrations found in the current studies were similar to those found in healthy human volunteers (1,000–4,000 ng/mL 1–8 h after dosing). 41 Overall, the concentrations found in the tear film were comparable or higher than those found in the aqueous humor after topical dosing,14–17,42 or the administration of collagen shields soaked in moxifloxacin43–45 (Table 10). The moxifloxacin tear film concentration results from the current study suggest that, given the favorable penetration characteristics of this antibiotic, therapeutic concentrations could also be delivered to the aqueous humor. However, aqueous taps would be necessary to determine actual moxifloxacin levels in the anterior chamber.
Overall, the moxifloxacin concentration remained above the target MIC90 value for susceptible organisms (≥250 ng/mL) for 7 days, with the exception of day 1 for Study 1. Study 2 provided average and median tear film concentrations well above the MIC90 values for all of the aforementioned susceptible species for 10 days. The Ocular Trust (2008) reported that most recent moxifloxacin MIC90 value for Str. pneumoniae was 120 ng/mL. 11 Other MIC90 values from bacterial conjunctivitis, 26 keratitis, 46 and endophthalmitis isolates 28 for moxifloxacin are included in Table 11. Study 1 showed average moxifloxacin tear film concentrations that, with the exception of some species from keratitis isolates at some time points, remained above the MICs for 10 days.
Denotes MIC50 values.
MIC, minimum inhibitory concentration.
Moxifloxacin has exhibited a favorable safety and tolerability profile in a number of preclinical and clinical studies. Studies with rabbits and nonhuman primates found a high margin of safety to the ocular and nonocular tissues for the compound when administered at concentrations up to 3% (using regimens and durations in excess of those prescribed in the label). 47 Another preclinical rabbit model reported that corneal epithelial integrity and tight junction organization were maintained with moxifloxacin. 48 In a human clinical study with normal patients, moxifloxacin produced no significant toxicity to the corneal epithelium or endothelium as assessed by confocal microscopy. 49 Topically administered moxifloxacin has a proven safety and tolerability record in humans.9,50 Clinical studies with patients undergoing cataract surgery indicate that this compound is even safe for intracameral use (an off-label use of the product).51–53
These 2 studies report a favorable safety profile for the Moxifloxacin Punctum Plug. There were no adverse events, serious or otherwise, reported for either study. Mean IOP values were stable over the course of the study. The most common ocular findings for both studies on slit lamp examination were aqueous chamber cells and corneal staining/erosion. All of these findings were graded as trace to mild with 1 exception (1 moderate grade of aqueous chamber cells on day 3 for Study 1). The most common sensations reported by patients in the ocular queries were itching, foreign body sensation, and excessive tearing. The investigator determined that these findings and sensations were probably related to cataract surgery. 54 This beneficial tolerability profile may translate into greater adherence than that observed with topical drops administered several times a day over the course of several days. For patients diagnosed with bacterial conjunctivitis, this could be particularly advantageous, as the MP could potentially eliminate the need for topical antibiotic regimens. Cataract patients were chosen for the pilot study due to ease of access to the subject population; however, future studies may target patients diagnosed with bacterial conjunctivitis to further test efficacy.
Due to the nature of these pilot studies, the sample sizes were small and performed in healthy volunteers. Limitations to the current studies could affect their ability to predict punctum plug performance in the general population. Further studies are necessary in patients diagnosed with bacterial conjunctivitis to determine actual cure rates, and aqueous humor and conjunctival concentrations of moxifloxacin should be measured to ascertain whether drug concentrations in those compartments achieved therapeutic levels.
Conclusions
The Moxifloxacin Punctum Plug delivered and maintained moxifloxacin tear fluid concentrations at concentrations above the MIC90 values for the common, fluoroquinolone susceptible pathogens that cause bacterial conjunctivitis. The Moxifloxacin Punctum Plug possesses a favorable safety and tolerability profile, which could provide an adherence advantage for patients. A therapeutic concentration of antibiotic could be delivered over the entire course of therapy with a single application of the drug. The results of these 2 studies suggest that the Moxifloxacin Punctum Plugs may be a viable alternative to topical antibiotic drops for the treatment of bacterial conjunctivitis. These feasibility studies support the initiation of further clinical trials in larger groups of patients to measure the safety and efficacy of the Moxifloxacin Punctum Plug.
Footnotes
Acknowledgments
The author would like to thank Julie Crider, Ph.D., for medical writing contributions. This medical writing assistance was funded by Ocular Therapeutix, Inc. This study was supported by Ocular Therapeutix (Bedford, MA).
Author Disclosure Statement
Professor Chee is a consultant for Bausch and Lomb.