
Abstract
Abstract
Purpose:
The purpose of our study was to evaluate the effectiveness of preoperative and postoperative addition of topical diclofenac to chloramphenicol/dexamethasone in patients undergoing uneventful phacoemulsification cataract surgery.
Methods:
Patients were randomized to (1) chloramphenicol 0.5%–dexamethasone 0.1%, 1 drop 4 times a day (n=41), or (2) chloramphenicol 0.5%–dexamethasone 0.1%, 1 drop 4 times a day, plus diclofenac 0.1%, 1 drop 3 times a day (n=38). Patients in the second group also received diclofenac 0.1% for 3 days before surgery. Topical treatment was administered for 28 days after phacoemulsification. On postoperative days 1, 14, and 28, best corrected visual acuity, macular thickness, endothelial cell density, and central corneal thickness (CCT) were measured.
Results:
The 2 groups did not have a statistically significant difference for CCT, endothelial cell density, macular thickness, and visual acuity at the 3 time points of the follow-up period.
Conclusions:
The addition of diclofenac did not seem to offer any additional benefit after uneventful phacoemulsification.
Introduction
Several combinations of postoperative treatment regimens have been evaluated after cataract surgery, including a steroid agent alone,4,8–10,11 a steroid plus an antibiotic,12–16 a nonsteroid drug alone,9,10,11,16,17 a nonsteroid plus an antibiotic, 14 a combination of a nonsteroid plus a steroid agent, 4 or a combination of an antibiotic and a nonsteroid plus a steroid agent. 15 The different treatment regimens have been designed to reduce postoperative inflammation and infection rates after cataract surgery.
Nonsteroid anti-inflammatory drugs (NSAIDs) have been reported to control synthesis of prostaglandins by inhibiting cyclo-oxygenase. In fact, inflammatory mediators, like prostaglandins, are triggered by surgical trauma, leading to disruption of the blood–retinal barrier and inducing cystoids macular edema (CME). In addition, the disruption in blood–aqueous barrier, caused by ocular/surgical trauma, leads to increase of flare and corneal edema. NSAIDs prevented the increase of flare and are more effective than steroids in preventing postoperative inflammation. 18 Diclofenac sodium 0.1% is a nonsteroid anti-inflammatory drug (NSAID) that inhibits the synthesis of prostaglandins and thromboxanes. Unlike other NSAIDs, it not only interferes with the inhibition of the activity of cyclo-oxygenase, but it also modulates the lipoxygenase pathway, decreasing postoperative inflammation. Previous studies have found that diclofenac sodium 0.1% is effective in both prevention and treatment of postoperative CME.5,7,9
Based on these factors, this prospective randomized trial was designed to evaluate the effectiveness of the preoperative and postoperative addition of an NSAID (diclofenac) to an antibiotic/steroid combination, specifically, chloramphenicol/dexamethasone. We compared the corneal and foveal changes as well as visual acuity between 2 groups at 3 time points during follow-up (days 1, 14, and 28 postoperatively) in patients undergoing uneventful phacoemulsification cataract surgery.
Methods
Seventy-nine participants were recruited in the 1st Department of Ophthalmology, University of Athens, Greece. Patient information included age, sex, and affected eye for surgery. Preoperatively, all patients had a complete ophthalmologic examination, including measurement of best corrected visual acuity (BCVA) by means of Snellen charts, intraocular pressure evaluation (IOP) by Goldmann tonometry, slit-lamp examination, and fundus examination. Optical coherence tomography (OCT) examination (Stratus OCT3; Carl Zeiss Meditec, Dublin, CA) and specular microscopy (CSO SP-01 specular microscope; CSO, Firenze, Italy) were performed by an experienced operator, to measure macular thickness and endothelial cell count (ECC), respectively. Central corneal thickness (CCT) was also measured by specular microscopy (CSO SP-01 specular microscope).
All patients underwent phacoemulsification cataract surgery with a standard technique by the same experienced surgeon (M.M.). The duration of the application of ultrasound during phacoemulsification and the duration of the whole operation were recorded.
Exclusion criteria were presence of corneal abnormalities; history of intraocular surgery; preoperative ECC <1,500 cells/mm2; history of uveitis, diabetes, and age-related macular degeneration; regular, systemic use of steroid or NSAIDs during the previous 3 months; and intraoperative complications, such as posterior capsule rupture, vitreous loss, lost nucleus, zonule dehiscence, and wound leak.
The study was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the institutional review board of our hospital. Written informed consent was obtained from all patients.
Patients were randomized (through random number generation) to 1 of the 2 postoperative treatment arms: (1) chloramphenicol 0.5%/dexamethasone sodium phosphate 0.1% (Dispersadron®; Novartis Hellas, Athens, Greece), 1 drop 4 times a day (chloramphenicol/dexamethasone [CD] group, n=41), or (2) a combination of chloramphenicol 0.5%/dexamethasone sodium phosphate 0.1% (Dispersadron; Novartis), 1 drop 4 times a day, plus diclofenac sodium 0.1% (Denaclof®; Novartis), 1 drop 3 times a day (chloramphenicol/dexamethasone plus diclofenac [CD-D] group, n=38). Patients in the CD-D group were treated with Denaclof (1 drop 3 times a day) for 3 days before surgery. Both groups also received brimonidine 0.1% (Alphagan®; Allergan, Irvine, CA) 1 drop twice a day. The topical treatment was administered for 28 days after phacoemulsification.
Three follow-up visits on postoperative days 1, 14, and 28 were scheduled for all patients. A thorough ophthalmologic examination, including BCVA measurement, slit-lamp examination, IOP measurement, funduscopy, OCT scan, ECC measurement, and CCT measurement, was performed at all follow-up visits by the same ophthalmologist.
The Gaussian distribution assumption was tested using the Kolmogorov–Smirnov test. None of the variables (age, BCVA, CCT, total operation duration, and ultrasound duration) succeeded in passing the normality test, except for ECC and macular thickness. The differences in baseline characteristics and outcomes between the 2 groups were compared by the Mann–Whitney–Wilcoxon test for independent samples (referred to as MWW for brevity), as appropriate. The Student's t-test was used to compare ECC and macular thickness between the 2 groups because they followed the normal distribution. Given that 4 comparisons (day 0, 1, 14, and 28) were assessed, the Bonferroni correction for multiple comparisons was adopted; as a result the threshold of statistical significance for P values was set to 0.05/4=0.0125. For BCVA, the descriptive statistics of the log of the minimum angle of resolution (logMAR) were computed as appropriate. 19 Statistical analysis was performed with STATA 11.0 statistical software (StataCorp, College Station, TX).
Results
The demographic and intraoperative characteristics of the 2 groups are shown in Table 1. The groups had no statistically significant differences for age, gender, BCVA, ECC, CCT, and macular thickness. Intraoperatively, the 2 groups had no statistically significant difference in the duration of the ultrasound application (P=0.513, MWW) nor in the total operation time (P=0.274, MWW).
CD, chloramphenicol/dexamethasone; CD-D, chloramphenicol/dexamethasone plus diclofenac; BCVA, best corrected visual acuity; ECC, endothelial cell count; CCT, central corneal thickness; U/S, ultrasound; MWW, Mann–Whitney–Wilcoxon test; T, Student's t-test; C, χ2-test.
The CCT did not differ statistically between the 2 groups at the 3 time points of follow-up (for CD and CD-D groups, respectively: 590.5±45.1 μm vs. 595.5±42.5 μm on day 1, P=0.617, MWW; 568.9±45.0 μm vs. 585.6±41.6 μm on day 14, P=0.073, MWW; 555.0±42.5 μm vs. 578.4±41.8 μm on day 28, P=0.013, MWW; Fig. 1).
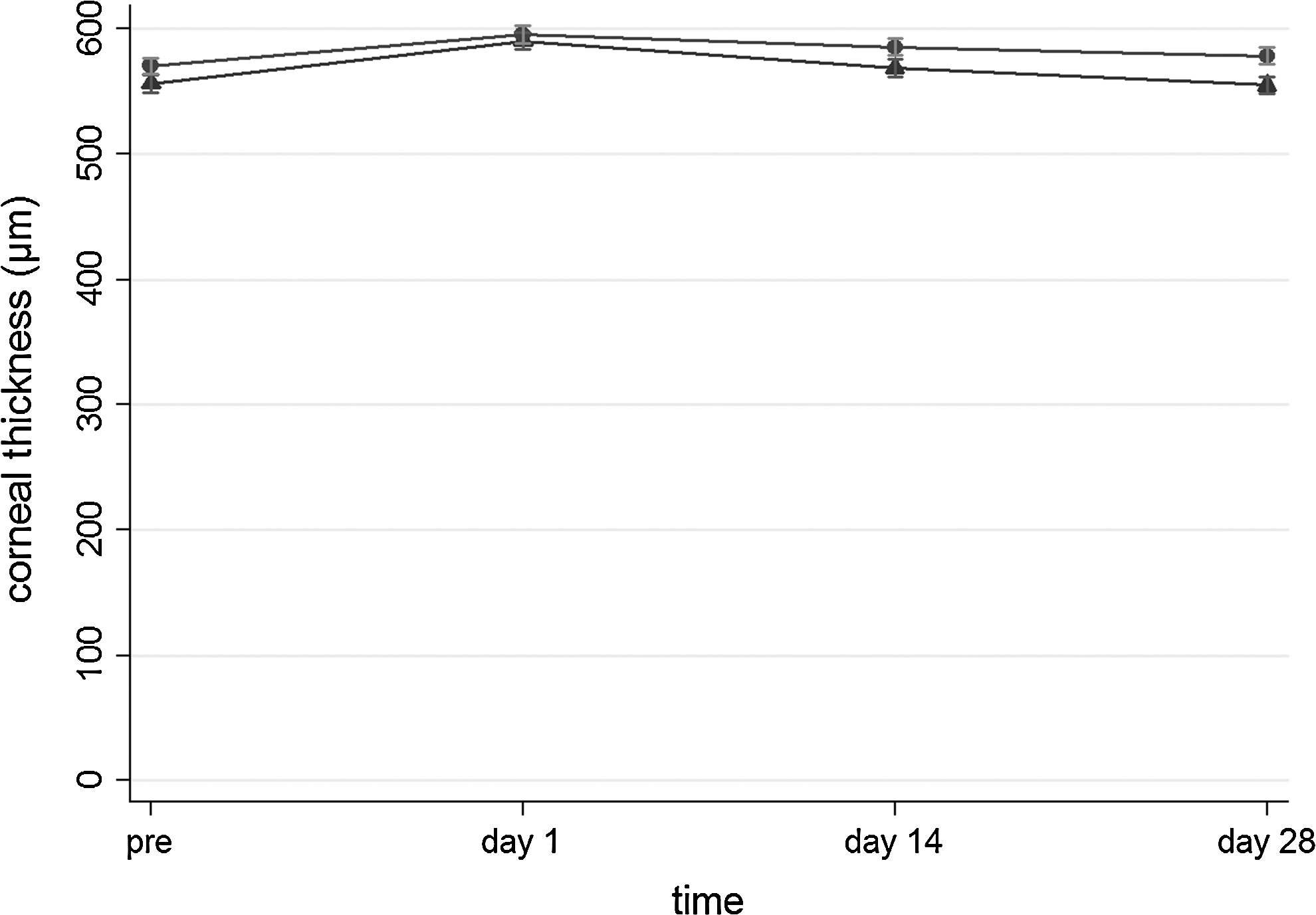
Central corneal thickness (mean±standard error, μm) on postoperative days 0, 1, 14, and 28 in the CD-D group (dots) and CD group (triangles). CD, chloramphenicol/dexamethasone; CD-D, chloramphenicol/dexamethasone plus diclofenac.
Further, no statistically significant difference in ECC was seen between the 2 groups at the 3 follow-up times (for CD and CD-D groups, respectively: 2122.7±526.1 cells/mm2 vs. 1991.8±382.7 cells/mm2 on postoperative day 1, P=0.213, Student's t-test; 2321.9±468.1 cells/mm2 vs. 2085.7±369.4 cells/mm2 on postoperative day 14, P=0.016, Student's t-test; 2395.9±451.1 cells/mm2 vs. 2193.1±387.8 cells/mm2 on postoperative day 28, P=0.036, Student's t-test; Fig. 2).
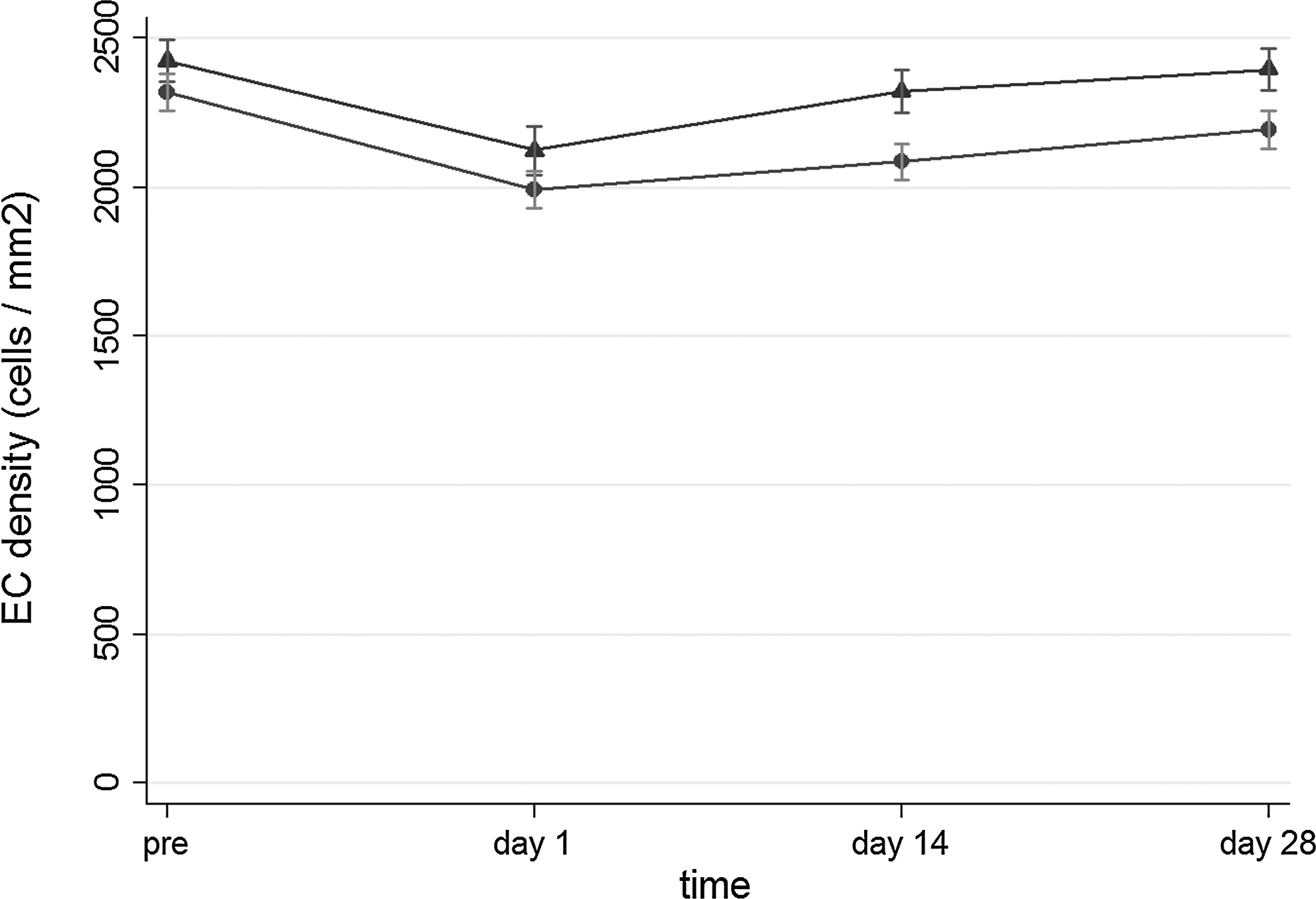
Endothelial cell count (mean±standard error, cells/mm2) on postoperative days 0, 1, 14, and 28 in the CD-D group (dots) and CD group (triangles).
Macular thickness did not differ significantly between the 2 groups at the 3 time points (for CD and CD-D, respectively: 169.6±20.0 μm vs. 164.1±21.8 μm on postoperative day 1, P=0.240, Student's t-test; 158.3±17.7 μm vs. 157.7±21.3 μm on postoperative day 14, P=0.890, Student's t-test; 152.0±16.3 μm vs. 152.3±20.8 μm on postoperative day 28, P=0.926, Student's t-test; Fig. 3).
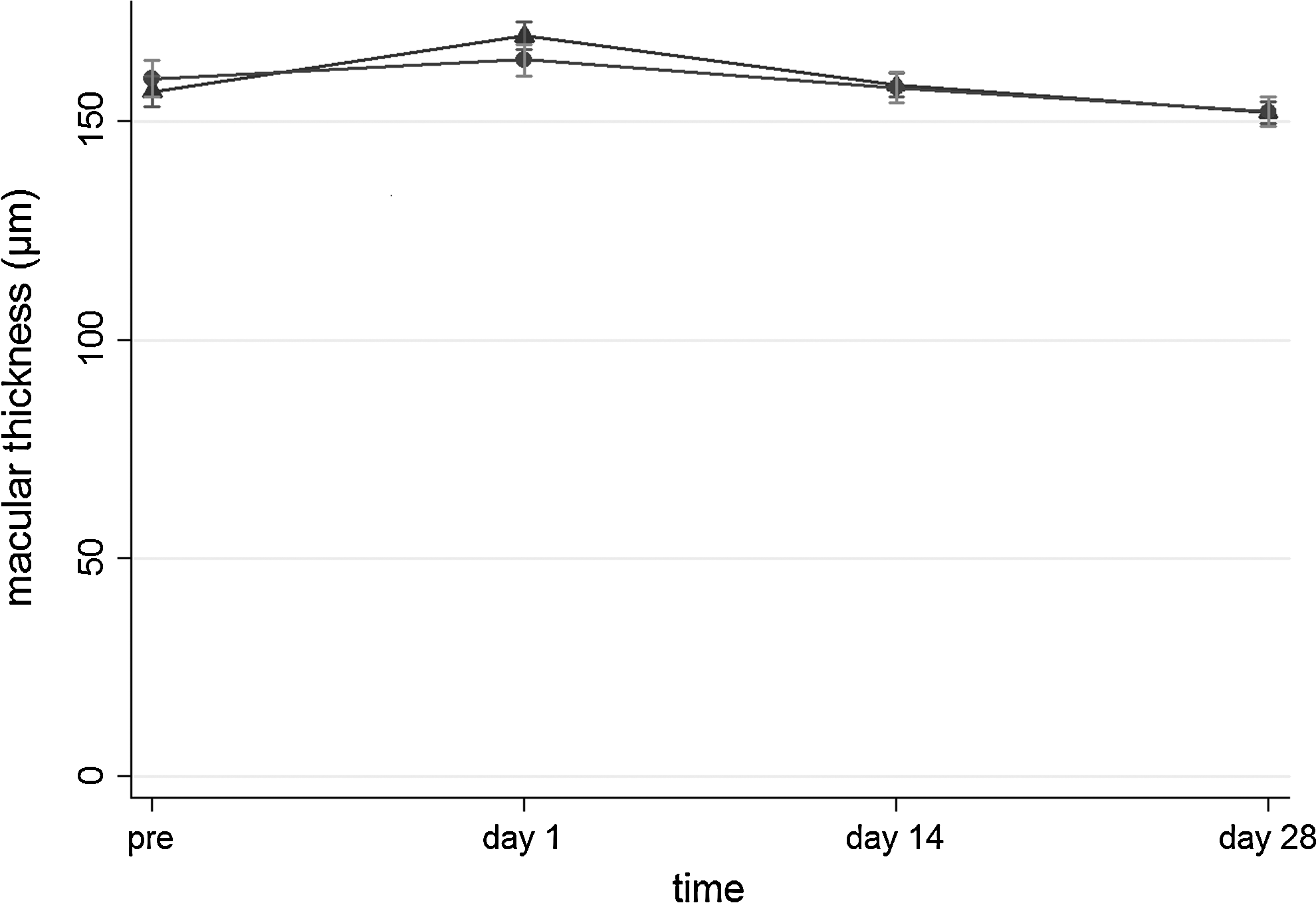
Macular thickness (mean±standard error, μm) on postoperative days 0, 1, 14, and 28 in CD-D group (dots) and CD group (triangles).
BCVA (logMAR) did not differ between the 2 groups at the 3 time points (for CD and CD-D, respectively: 0.19±0.20 vs. 0.18±0.20 on postoperative day 1, P=0.340, MWW; 0.08±0.09 vs. 0.08±0.09 on postoperative day 14, P=0.493, MWW; 0.00±0.01 vs. 0.00±0.01 on postoperative day 28, P=0.957, MWW; Fig. 4).
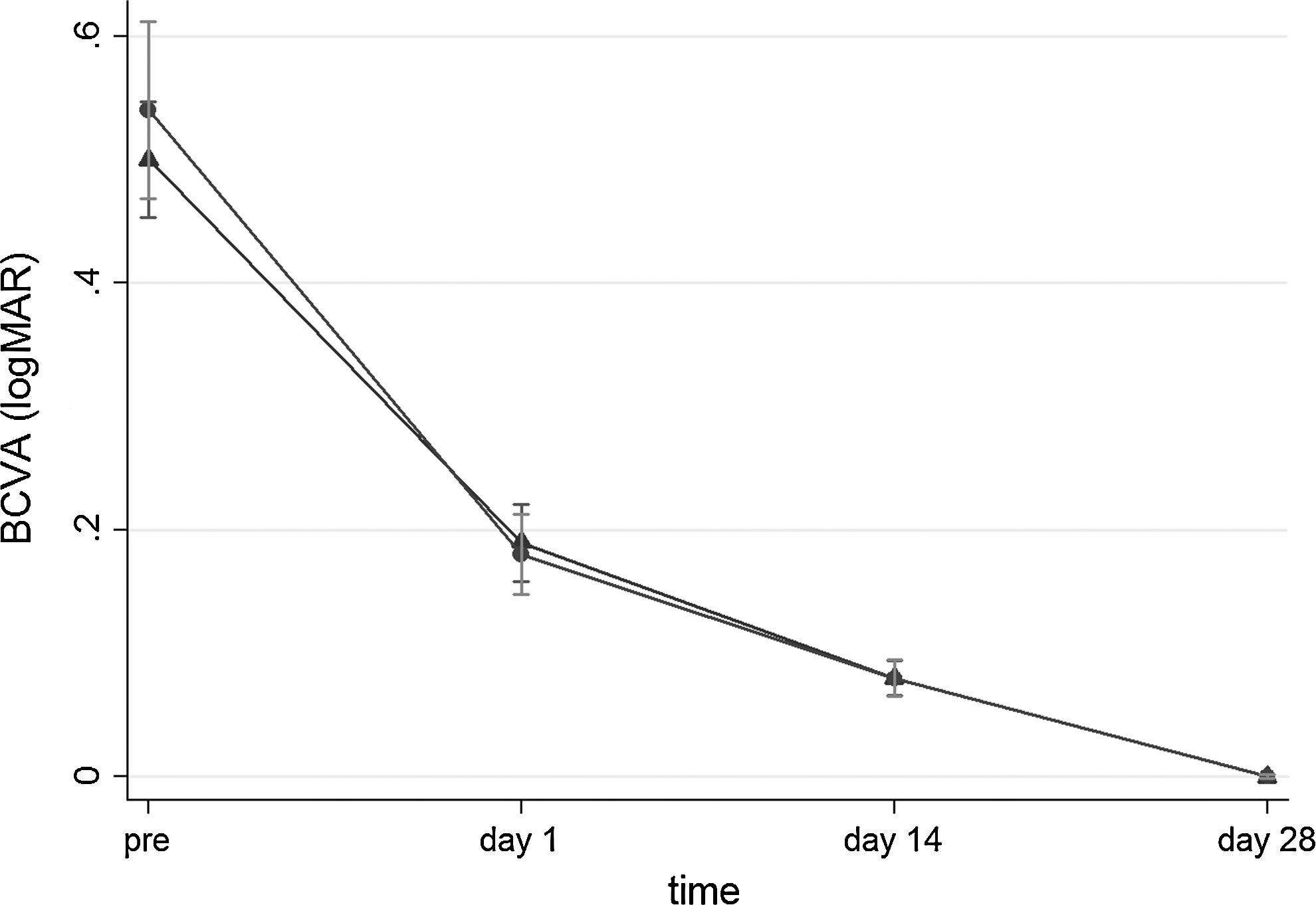
Best corrected visual acuity (mean±standard error, logMAR) on postoperative days 0, 1, 14, and 28 in CD-D group (dots) and CD group (triangles); logMAR, log of the minimum angle of resolution. BCVA, best corrected visual acuity.
A post hoc power calculation was performed at the completion of the study (day 28), as this time point may reflect the clinical performance of diclofenac.
BCVA was not included in the power calculations, as the latter were not feasible in light of the equal mean values (logMAR=0) in both groups.
The estimated power was relatively satisfactory regarding CCT (69.4%) and ECC (57.4%). On the other hand, the post hoc estimated power concerning macular thickness was only 5.1%; nevertheless, this artificially low power may probably be due to the underlying lack of difference as reflected upon the comparison basis of the calculation (152.0±16.3 vs. 152.3±20.8). Indeed, the optimal power of 80% would necessitate a theoretical study encompassing 60,902 patients in each group to reach a significant conclusion; in other words, the lack of difference seems rather warranted. Taken as a whole, despite the relatively small study sample, the conclusions drawn seem rather valid and substantiated as far as the notion of statistical power is concerned.
Discussion
The principal message of this study is that the addition of an NSAID (diclofenac) after uneventful phacoemulsification surgery did not seem to offer any additional benefit in terms of CCT, ECC, macular thickness, and BCVA when compared with the antibiotic/steroid group.
The damage of the corneal endothelium can be evaluated by measuring the decrease in CCT and ECC after surgery. Adult human corneal endothelium is considered a nonreplicative tissue and a natural decrease in EC density occurs with age. 20 In addition to this, corneal thickness increases when the pump and barrier functions of the endothelium are damaged, affecting the clarity of the cornea. If there is a certain decrease in ECs and an increase in corneal thickness, corneal edema appears. 6 In our study, CCT and EEC did not differ between the 2 groups and reached normal ranges postoperatively. It is worth mentioning that at postoperative day 28 none of the patients presented with corneal edema, indicating that both treatment arms were equally effective in preventing postoperative corneal edema and, therefore, inflammation.
Previously anti-inflammatory treatment after extracapsular cataract extraction was necessary because lens epithelial cells remained in the capsular bag. 10 Currently, the development of phacoemulsification has reduced BAB damage, postoperative inflammation, and CME. The rationale for the addition of an NSAID to a topical steroid after uneventful phacoemulsification pertains to the prevention of CME and remains controversial. 4 Asano et al. found that diclofenac was more effective than betamethasone in preventing CME in modern cataract surgery, 9 in accordance with other studies, which also recommended NSAIDs for postoperative treatment.4,7,11,21,22
In contrast, Laurell and Zetterstrom suggested that dexamethasone and diclofenac are equally effective in preventing postoperative inflammation and CME, 10 in line with other studies that found no differences between the use of steroid agents and NSAIDs postoperatively.15,17,23 In our series no case of CME appeared, as evaluated through funduscopy and OCT. Macular thickness did not differ significantly between the 2 groups and reached normal ranges preoperatively and postoperatively in both groups. The incidence of acute CME after uneventful phacoemulsification reaches its peak at 4 to 6 postoperative weeks; importantly, the majority of cases resolve spontaneously. 24 As a result, the cost-to-benefit ratio of treatment with NSAIDs remains obscure, given the low incidence (as in our study) and self-limited nature of CME.
Diclofenac did not affect the postoperative outcome of BCVA compared with that in the chloramphenicol/dexamethasone group. Patients in both groups presented with excellent BCVA on postoperative day 28, suggesting that uneventful phacoemulsification cataract surgery is beneficial for patients' visual acuity.
A limitation of our study is that the assessment of inflammation through laser flare measurement could have yielded more sensitive, objective results. However, we have evaluated corneal edema, as an inflammation-related sign, in an objective way by measuring CCT and ECC. Also, slit-lamp examination did not reveal any inflammatory signs on postoperative day 28. Another meaningful limitation that should be declared pertains to the interesting notion of clinically significant CME. The incidence of the latter is extremely low ranging between 0.1% and 2% in various series of uneventful phacoemulsification.11,24 Given the small sample size of the present study, the examination of CME and any differences between the 2 groups was precluded. It should be, however, stressed that no cases of CME were observed in either of the examined group.
In conclusion, the results of the present study are in line with skepticism about the need for an NSAID in the context of uneventful phacoemulsification. The addition of diclofenac after cataract surgery did not seem to offer any additional benefit for treating postoperative inflammation and CME when compared with using an antibiotic/steroid because corneal and foveal changes did not differ between the 2 groups.
Footnotes
Author Disclosure Statement
No competing financial interests exist.