
Abstract
Abstract
Purpose:
To assess the effect and safety of using single intravitreal bevacizumab (IVB) versus intravitreal triamcinolone acetonide (IVTA) and grid laser photocoagulation (GLP), or a combination of IVB and IVTA for treatment of retinal vein occlusion (RVO)-associated macular edema, mainly exploring its effects on visual acuity (VA) and central macular thickness (CMT).
Methods:
Eligible studies were identified via searching databases, including Medline (PubMed), Web of Science, and the Cochrane Library, without status or other limits up to June 2012.
Selection Criteria:
We include randomized clinical control trials comparing 1.25 mg IVB injection with other treatment strategies, including a 4 mg IVTA injection or GLP or a combination of 1.25 mg IVB and 2 mg IVTA injection, for patients with RVO-associated macular edema. Eligible studies should report both VA and CMT outcomes, and with a minimum follow-up of 4 weeks.
Results:
Two authors assessed the trial quality and extracted data independently.
Main Results:
Four studies were included in this study. Comparing to IVTA and GLP, IVB was more effective in improving VA at 1 month (weighted mean difference [WMD], −0.07; 95% confidence interval [CI], −0.10 to −0.05; P<0.00001), 3 months (WMD, −0.24; 95% CI, −0.28 to −0.20; P<0.00001), and 6 months during the follow-up (WMD, −0.17; 95% CI, −0.21 to −0.13; P<0.00001) in patients with RVO-associated macular edema. There was no statistical significance in reducing CMT values throughout the periods. Compared with IVB/IVTA combination, VA improvement became statistically significant at 3 months of follow-up (WMD, −0.26; 95% CI, −0.29 to −0.23; P<0.00001), while no statistical significance was found in both VA values at 1 month of follow-up and CMT values throughout the periods. The occurrence of intraocular pressure (IOP) was much lower in IVB groups.
Conclusions:
IVB is effective in treating patients with RVO-associated macular edema; especially if it has distinct effects, of which, VA could be improved to the utmost extent as well as by the earliest of time. IVB is also effective in decreasing CMT, but without any significant advantages over IVTA or GLP. Furthermore, IVB seems to be safer than IVTA in consideration of IOP increase.
Introduction
Based upon the type of the vascular damage associated with the occlusion, visual loss is primarily due to the development of a series of complications, including macular edema, retinal hemorrhage involving the fovea, and neovascular glaucoma. Persistent macular edema is the main cause for the loss of central vision.5,6
Despite the existence of numerous potential therapeutic options (such as laser photocoagulation and intravitreal corticosteroids), many patients with RVO suffer irreversible visual loss due to not entirely satisfactory therapeutics7,8 Fortunately, the recent introduction of antivascular endothelial growth factor (VEGF) agents, such as ranibizumab (Lucentis®, Genentech, South San Francisco, CA) and bevacizumab (Avastin®, Genentech, San Francisco, CA), offers a potentially new treatment approach for this disorder. 9
Among all the anti-VEGF agents, bevacizumab is a full-length humanized monoclonal antibody directed against all biologically active forms of VEGF, which has been reported to be effective in decreasing retinal thickness and improving visual acuity (VA) when injected intravitreally for the treatment of RVO.10,11
However, the beneficial effects of intravitreal bevacizumab (IVB) have been reported to be time-limited with the need for re-injections. 8 In addition, the ophthalmologist's decision making in choosing bevacizumab for the treatment of RVO-associated macular edema would be affected considering its potential side effects when used in patients with concurrent cardiovascular conditions. 12 Therefore, formal evaluation of the safety and efficacy of IVB in the treatment of RVO-associated macular edema is warranted. Thus, we conducted a systematic review of randomized clinical control trials (RCCTs) evaluating the effect and safety of IVB versus generally acknowledged treatment strategies, including grid laser photocoagulation (GLP) and intravitreal triamcinolone acetonide (IVTA), as well as a combination of IVB and IVTA for management of RVO-associated macular edema.
Methods
We identified relevant publications in PubMed, Web of Science, and the Cochrane Library up to June 2012. Search terms included “macular edema/oedema” and “RVO” combined with “bevacizumab” or “avastin”. The titles and abstracts were scanned to exclude any clearly irrelevant studies, such as case reports, mechanism studies, or animal experiments. The full texts of the remaining articles were read to determine whether they contained information on the topic of interest.
Eligible studies met the following criteria: (1) RCCTs published as original articles; (2) articles reported in English between 1985 and June 2012; (3) studies comparing the intervention of 1.25 mg/0.05 mL of IVB injection with GLP, IVTA, or IVTA/IVB combination for the treatment of RVO-associated macular edema; (4) studies indicated VA and central macular thickness (CMT) as the main outcome measures; and (5) trial measured patients with at least 4 weeks of follow-up. In studies with overlapping patients or controls, only the latest or the most complete was included. Any study with inconsistent or erroneous data was excluded. Meeting abstracts with insufficient data or unpublished reports were not considered. No studies were excluded based on the number of study subjects, country of origin, or status of publication.
Information from the included studies was extracted by 2 researchers (Yi Lu and Li Su) using a standardized form independently. Conflicting evaluations were resolved by discussion. If a consensus could not be reached still, the senior investigator (Xun Xu) made the final decision. Pertinent data included study population characteristics (age, gender, number of patients and eyes in study, and location), intervention groups, comparison groups, outcome variables, and duration of follow-up. 13
A Jadad quality assessment was conducted for assessing their methodological quality of the included trials. In this assessment, quality was based upon 7 questions, with a score range of 0–5, with higher scores indicating a higher study quality. 14
After subgrouping the results according to the comparison—IVB versus the comparison group (IVTA or GLP) or IVB/IVTA combination—pooled summary estimates were calculated for each outcome of interest: VA in logarithm of the minimum angle of resolution (logMAR) units and CMT in micrometers (μm). Weighted mean differences (WMDs) were calculated based on a fixed effects model with a P-value≤0.05 being considered significant (RevMan software version 5.1.7). We chose intraocular pressure (IOP) as the main result indicating the safety of IVB versus the other treatments in this review. All the included trials except Russo's study, 15 reported IOP increase during the follow-up. Beyond that, no other severe ocular, especially infectious endophthalmitis, or systemic adverse events occurred.
Results
Results of the search
Figure 1 is a flow diagram of selection of eligible studies. An extensive literature search revealed 533 articles, 527 of which were excluded after review of titles and/or abstract. Upon full-text examination, 2 of the remaining 6 studies were excluded because they only compared IVB with sham.16,17 As shown in the flow diagram, a total of 4 studies15,18–20 were included in the review. Among them, 2 studies18,20 focused on central retinal vein occlusion (CRVO)-associated macular edema, while the other 2 on branch retinal vein occlusion (BRVO) associated.15,19
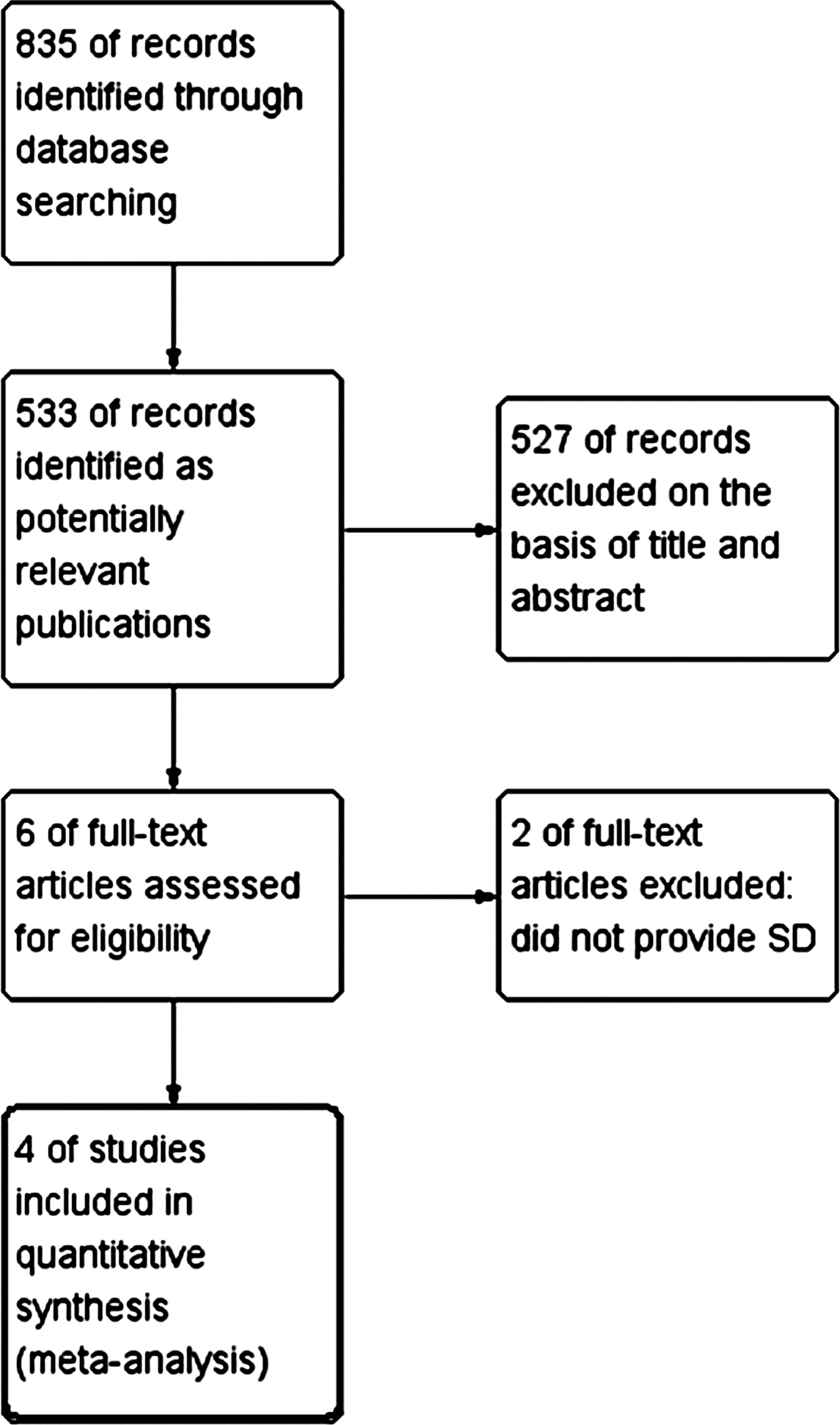
Flow diagram of study selection process. SD, standard deviation.
Included studies
The characteristics of the 4 included studies are outlined in Table 1. Study sample sizes ranged from 30 to 75 patients. Patient characteristics were similar across all trials, with mean ages ranging from 55.16 to 66.5 and gender being male predominantly. All studies used 1.25 mg of IVB as the intervention. The comparison group interventions varied by each study, including GLP, IVTA, and IVB/IVTA combination. The duration of follow-up ranged from 3 to 12 months. The methodological quality of the 4 included studies were assessed based on the Jadad score, and were not in good quality.
N, number; M, male; IVB, intravitreal bevacizumab; IVTA, intravitreal triamcinolone acetonide; GLP, grid laser photocoagulation; N/A, not available; PRN, pro re nata; RVO, retinal vein occlusion; BRVO, branch retinal vein occlusion; CRVO, central retinal vein occlusion.
Effects of interventions
IVB versus IVTA or GLP
Visual acuity: Pooling the results revealed that at 1 month of follow-up, treatment with IVB significantly improved VA as compared to the IVTA or GLP (WMD, −0.07; 95% confidence interval [CI], −0.10 to −0.05; P<0.00001). This improvement in VA persisted into the third (WMD, −0.24; 95% CI, −0.28 to −0.20; P<0.00001), as well as the 6th month of follow-up (WMD, −0.17; 95% CI, −0.21 to −0.13; P<0.00001). (Fig. 2)
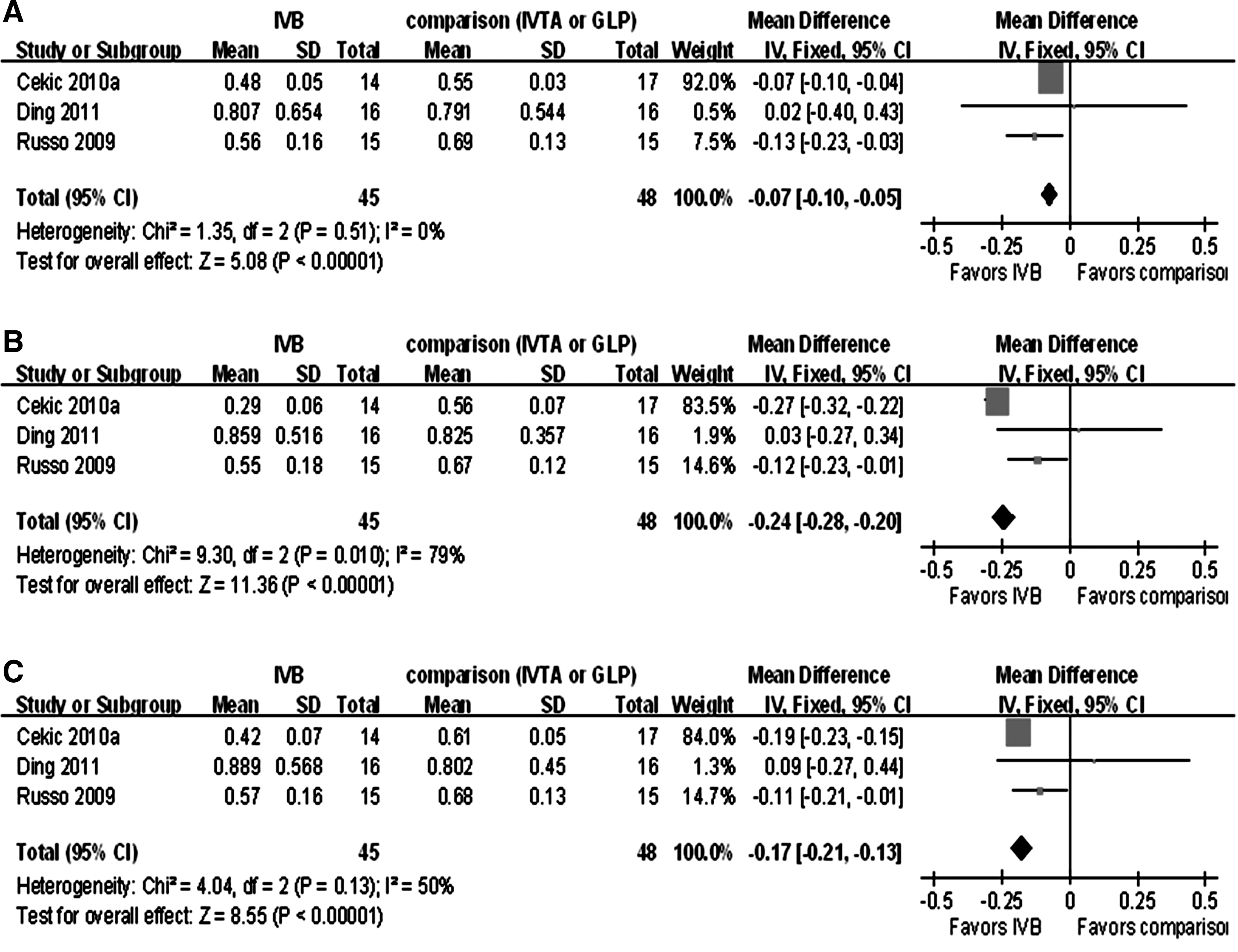
Forest plot displaying pooled summary estimates of VA with IVB treatment versus comparison group, including IVTA or GLP.
Central macular thickness: There was no significant difference in CMT values in those treated by IVB compared to those with the other 2 interventions during the 1st month of follow-up (WMD, −9.91; 95% CI, −51.82 to 32.01; P=0.64), and the third and 6th month as well (WMD, −22.52; 95% CI, −54.27 to 9.23; P=0.16; WMD, −21.15; 95% CI, −57.88 to 15.59; P=0.26; respectively). (Fig. 3)
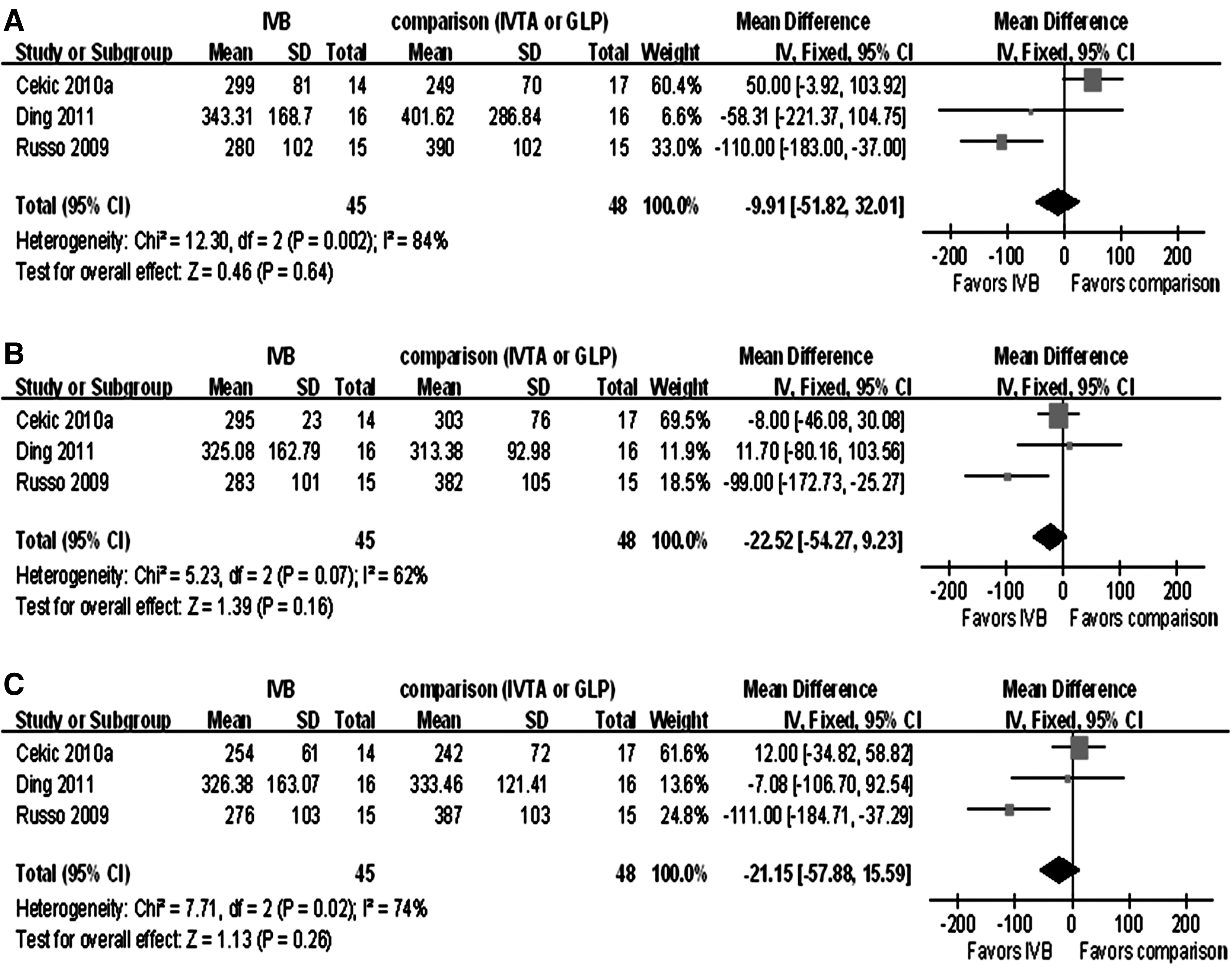
Forest plot displaying pooled summary estimates of central macular thickness with IVB treatment versus comparison group, including IVTA or GLP.
IVB versus IVB/IVTA combination
Visual acuity: There was no significant difference between single IVB and IVB/IVTA combination in the 1st month of follow-up (WMD, −0.01; 95% CI, −0.04 to 0.02; P=0.41), while the difference became statistically significant after 3 months of follow-up, preferring IVB (WMD, −0.26; 95% CI, −0.29 to −0.23; P<0.00001). (Fig. 4)
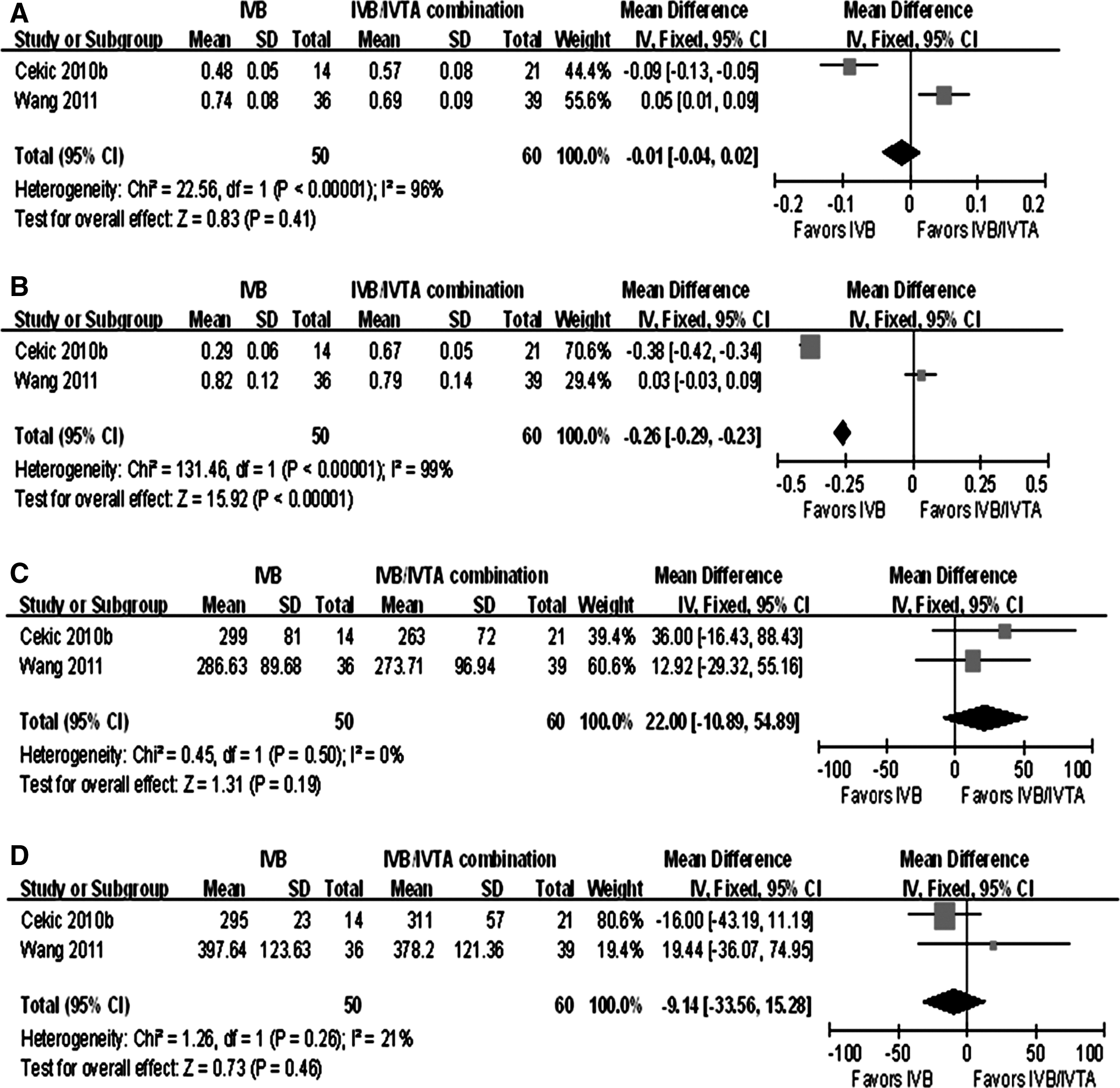
Forest plot displaying pooled summary estimates of VA and CMT with IVB treatment versus IVB/IVTA combination.
Central macular thickness: There was no significant difference in CMT of those treated in the IVB group when compared to those with combined treatment (WMD, 22.00; 95% CI, −10.89 to 54.89; P=0.19; and WMD, −9.14; 95% CI, −33.56 to 15.28; P=0.46; respectively), both after 1 and 3 months. (Fig. 4)
IOP changes of the interventions
High IOP is known to be one of the main side effects affecting the clinical use of both IVB and IVTA. Thus, we calculated related information about IOP changes in all the 4 included studies in this review. As mentioned above, all studies reported occurrence of IOP increase other than Russo's study. 15 In Wang's study, 18 5 patients (13.89%) in the IVB group and 6 patients (15.38%) in the IVB/IVTA group showed transient high IOP. In Ding's study, 20 no patient in the IVB group had elevated IOP, while 6 patients (37.5%) in the IVTA group did. Moreover, Cekic et al. 19 reported that the average IOP change from baseline was significantly higher in the IVTA group at 1 month after injection (1.4±0.8 [±SEM], P=0.03), while those of the IVB and IVB/IVTA combination groups were not different (−0.1±0.2, P=0.26 and 0.5±0.2, P=0.07, respectively).
Discussion
The current medical literature reveals disparate levels of IVB effects when considering clinically relevant outcomes, such as VA and CMT. Additionally, there is no clear consensus on the ideal dosage and treatment regimen. Based on the results of Yilmaz's study, 21 we chose 1.25 mg of an IVB injection as our targeting dosage in our review.
Considering IVTA and GLP as the well acknowledged treatment for RVO-associated macular edema, we first compared the efficacy of IVB with these 2 treatments. Our analysis showed the improvement of VA using IVB was significantly better than the comparison group. Moreover, it began in the early stage of treatment (1 month), and persisted at least untill the 6th month, which was considered to be a long-term period in our analysis. However, the CMT values had no significant difference between the 2 groups during the period considered in this review, although they were all reduced significantly compared to the baseline. There might be several factors to this asynchronous phenomenon between VA and CMT: first, no consensus has been reached for the debate on the relationship between the VA improvement and the CMT reduction, and actually, they may not be time-synchronous; second, even the change of VA and CMT were closely time related, no one could deny the possibility that IVB was superior to IVTA and GLP, functionally other than anatomically, in treating the macular edema secondary to RVO; third, the result of a longer period such as 9 or 12 months was not mentioned in our analysis because of the shortage of data and the small sample size; thus, a large and long-term clinical trial is warranted to further explore this confusion.
The 1-fold beneficial effect of bevacizumab or triamcinolone acetonide on macular edema caused by both CRVO 18 and BRVO 19 has been shown in several studies, making bevacizumab and triamcinolone acetonide the 2 popular drugs being used increasingly for treating RVO-associated macular edema. Furthermore, recent studies have suggested that bevacizumab should be combined with triamcinolone acetonide for the treatment of macular edema secondary to other retinal vascular disorders such as diabetic retinopathy. Wang et al. had also administered this combination method for exudative age-related macular degeneration (AMD) and diabetic retinopathy, and most of these patients showed significant improvement in vascular leakage and macular edema. 18 Thus, we compared the beneficial effects of IVB and IVB/IVTA combination, discussing the difference between 1-fold application of IVB and the combination modality. The results were similar to those compared to IVTA and GLP, which again revealed that VA and CMT might change asynchronously and IVB might be a good choice to ameliorate patient's condition, at least, functionally.
It is well known that the use of systemic bevacizumab can increase cardiovascular and cerebrovascular events.22,23 While a recent randomized clinical trial evaluating the use of IVB for AMD revealed that there was no increased risk for death, myocardial infarction, or stroke compared to ranibizumab. 24 However, the uncertain risks of cardiovascular and other potential systemic events associated with IVB should be thoroughly considered in such therapeutic decision making. 25 It is noteworthy that all the 4 included studies did not demonstrate a severe adverse event of IVB. Compared with IVTA, the occurrence of IOP increase was lower when using IVB, which in fact was one of the main concerns about the use of IVB as well as IVTA. Moreover, IVB might decrease the risk of high IOP occurrence of IVTA when applied as a combined treating modality. Despite the findings of this analysis, triamcinolone acetonide seemed to cause more adverse events, including cataract,26,27 premacular membrane formation,16,19 and adverse effects of preservatives. 28
However, limitations to this review should be taken into account. First, all of the 4 included studies varied on many levels, particularly in the collection of baseline characteristics. Each study neglected to include information about attrition rates. Furthermore, none of the studies provided information regarding lens status, which is an important factor affecting the results, since those with pseudophakic eyes may have had an underestimation in adverse event rates, that is, cataract formation and/or IOP increase. The duration of RVO-associated macular edema also varied along with initial VA and CMT values and the intervals of IVB injection. Last, we did not differentiate between BRVO and CRVO, and all the 4 included studies did not differentiate between ischemic RVOs and nonischemic RVOs, which might be one of the major causes of bias.
The Jadad quality assessment scores for these studies varied between 0 and 2. The quality of the included studies is poor. The major limitations of these studies are summarized as follows: their unblinded nature, small sample sizes, imbalance of baseline VA and CMT values, unmeasured confounding variables, and lack of subgroup analyses of disparate baseline BRVO or CRVO types. Other than Russo's study, 15 no article addressed the issue of withdrawals or dropouts (i.e., attrition rates) from their respective trials, which could result in underestimating the occurrence incidence of adverse events.
Considering all the above, this review should be regarded as an indicator that IVB is effective in treating patients with RVO-associated macular edema, especially if it has distinct effects, of which, VA could be improved to the utmost extent as well as by the earliest of time. IVB is also effective in decreasing CMT, but without any significant advantages over IVTA or GLP. Furthermore, IVB seems to be safer than IVTA in consideration of IOP increase. This review is to serve as evidence for potential use of IVB as one of the therapeutic choices.
Authors' Contributions
YL: conception and design, analysis and interpretation of data, drafting the article and final approval of the version to be published. LS: design, analysis and interpretation of data and revising it critically for important intellectual content. XX: conception and design, analysis and interpretation of data, and final approval of the version to be published.
Footnotes
Acknowledgment
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.