
Abstract
Abstract
Purpose:
To investigate the influence of an eye ointment on functional visual acuity (FVA) and ocular wavefront aberration.
Methods:
In 11 healthy volunteers (6 men and 5 women), visual function parameters, such as FVA, visual maintenance ratios (VMR), and minimal visual acuity (minVA), were assessed by the FVA measurement system before and 2, 5, 10, 20, 30, 40, 50, 60, 90, 120, 180, and 240 min after administration of ofloxacin eye ointment. Ocular aberration was also measured, and the root mean square (RMS) of second-, third-, fourth-, and total higher-order aberrations was determined. The time course of changes in each parameter was statistically analyzed by using repeated-measures analysis of variance and the Dunnett post hoc test, and relationships between visual function and ocular aberration parameters were also analyzed by the Pearson correlation test.
Results:
FVA, VMR, and minVA showed significant deteriorations at 2-, 5-, 10-, and 20 min after administration of eye ointment compared with the baseline values (P<0.05). All components of ocular wavefront aberration such as second-, third-, fourth-, and total higher-order RMS significantly increased at 2- and 5 min after the administration of eye ointment compared with the baseline values (P<0.05). In addition, deteriorations of these visual function parameters were significantly correlated with reduced blink numbers (Pearson's correlation coefficient; r=− 0.76, P=0.017 for FVA, r=0.79, P=0.013 for VMR, and r=−0.62, P=0.040 for minVA), and VMR was significantly related with changes in second-order RMS (r=−0.60, P=0.049).
Conclusions:
Eye ointment significantly reduced visual function for at least 20 min. Especially, minVA was worse than 0.155 logMAR, which is legally required for driving, for 3 h after the administration. In addition, increases in lower-order aberration and low blink rates were associated with the degradation of visual function.
Introduction
There are several disadvantages associated with the use of eye ointments, one of which is the visual impairment caused by the vehicle. The bulk application of ointments can cause persistent blurred vision, resulting in decreased patient satisfaction and restriction of daily activities.10,13 Especially when an ointment is simultaneously applied to both eyes, patients can become handicapped by blurred vision.
Several ointments require multiple applications during the day. For example, acyclovir ointment is one of the most commonly used antiviral drugs for the treatment of herpes simplex keratitis, blepharoconjuntivitis, and iridocyclitis,14–16 and it requires a 5-time daily dosing regimen to maintain an effective drug level due to its very short half life. The frequent application and the resultant long-lasting blurred vision represent an obstacle for patients who follow the prescribed treatment schedule. 17 It has also been reported that ofloxacin eye ointment with a 3-time daily dosing regimen is useful for severe chlamydial conjunctivitis and leads to better curative effectiveness when compared with ofloxacin eye drops. 18
So far, visual impairment has been typically measured using 1-time measures of visual acuity (VA) with high contrast optotypes. Nowadays, however, much attention has been given to the sequential changes in visual function with tear film dynamics, because the changes are not static but dynamic phenomena. Functional visual acuity (FVA) testing has been recently developed for the assessment of dynamic changes of visual functions.19–22 The FVA measurement was initially devised for the detection of masked impairment of visual function in patients with dry eye who complained of decreased visual function despite normal conventional VA.19,20,23,24 Recently, it has been shown that the FVA system is a useful tool in the assessment of dynamic VA changes in mild cataract opacities, 25 posterior capsule opacification after cataract surgery, 26 Stevens–Johnson syndrome, 21 and laser in situ keratomileusis. 27 In addition, a transient and short-term visual deterioration caused by viscous eyedrops was detected with the FVA system. 28 In the current study, we quantitatively assessed dynamic change in VA by performing FVA measurements on subjects receiving eye ointment. Simultaneously, the accompanying changes in ocular aberration were assessed by serial measurements of wavefront aberration.
Subjects and Methods
Eleven healthy volunteers (6 men and 5 women) with best-corrected visual acuity (BCVA) of 20/20 or better and without systemic and ocular diseases (except for refractive errors) were enrolled in this study. They did not have any history of eye surgery or trauma, symptoms of dry eye, and regular use of eye drops and contact lenses. Their ages ranged from 22 to 57 years (37.6±12.0, mean±standard deviation), and manifest refraction was between −5.25 and 0.00 D (−1.94±2.03 D), with refractive astigmatism between −1.50 and 0.00 D (−0.57±0.63 D). Informed consent to participate in the study was obtained after the study protocol had been fully explained. The study adhered to the tenets of the Declaration of Helsinki and was approved by the institutional review board of Tsukuba University Hospital.
The FVA measurement system (SSC-350; Nidek, Aichi, Japan) was used to examine the changes in the continuous VA over time. This system has been described in detail elsewhere.19–23 In brief, the device is composed of 3 parts: a hard disk, a monitor to display optotypes, and a joystick for responding to optotypes. Landolt optotypes are presented on the monitor starting with the baseline BCVA. The test was performed monocularly with best spectacle correction at baseline. Subjects delineate the direction of the automatically presented Landolt rings by handling the joystick, and the size of optotypes changes by 1 step depending on the responses. They enlarge when the response is incorrect and become smaller when it is correct. If there is no response within 2 s, the answer is judged as an error and the optotype then becomes bigger. This testing is continuously performed for 60 s under natural blinking. When each testing is completed, the result is recorded as a line graph, which is made up of points joining the correct answers only. The outcome parameters of this system included logMAR FVA, visual maintenance ratio (VMR), minimal visual acuity (minVA), and blink numbers during the 60-s measurement session. FVA is defined as the average of VAs measured during the testing period. This average of all VA values measured over time reflects daily vision more efficiently than measuring VA at one specific time point. VMR is determined as the ratio of FVA divided by the baseline VA and calculated according to the following formula: VMR=decimal notation of FVA/decimal notation of baseline VA=(lowest logMAR VA−logMAR FVA)/(lowest logMAR VA−baseline logMAR VA). 21 With this index, the statistical comparison for groups with different baseline VAs becomes possible.21,22 MinVA is defined as the worst VA during the 60-s testing period. 29 The number of blinks during the 60-s measurement session was manually recorded by the examiner conducting the FVA examination.
Ocular wavefront aberration was measured under natural pupil dilation (i.e., no cycloplegic drugs were given) in a dim room using the newly developed Hartmann–Shack wavefront aberrometer (KR-1W; Topcon Corp., Tokyo, Japan) equipped with an automated function of measuring and recording sequential wavefront aberrations every second. This system has been described in detail elsewhere.30,31 Ten serial images were obtained at 1-s intervals from 1 to 10 s after a blink. The subjects were instructed to keep their eyelids open during the image capture. The acquired data sets were expanded with the normalized Zernike polynomials. From the Zernike coefficients, the root mean square (RMS) was calculated for second-, third-, fourth-, and total higher-order aberrations in the central 4-mm diameter. The second-order aberration corresponds to conventional refractive error (sphere and cylinder), which can be corrected by spherocylindrical lenses, whereas the third- and higher-order aberrations cannot. Therefore, third- and greater-order aberrations are identified as higher-order aberrations. The RMS of third-order Zernike coefficients was used to represent coma-like aberration, and the RMS of fourth-order Zernike coefficients was used to denote spherical-like aberrations. Total higher-order aberrations were calculated as the RMS of third- and fourth-order Zernike coefficients. The obtained data for 10 s (10 serial measurements) were averaged for each eye and used for the following analyses. In addition, 2 quantitative indices such as fluctuation index (FI) and stability index (SI) of the second- and total higher-order aberrations were calculated from the sequential changes in ocular aberrations over time according to the study of Koh et al.30,31 The FI was defined as the standard deviation of the aberration components obtained during the serial measurements for 10 s, which reflects the fluctuations in each aberration during the measurements. SI was calculated as the slope of the linear regression line of the obtained aberration components, which represents the trend of the sequential changes in each aberration during the measurement.
After the baseline measurements, we applied 0.05 g of 0.3% ofloxacin eye ointment (Tarivid® ophthalmic ointment; Santen Pharmaceutical, Osaka, Japan) on a glass rod, along a length of 1 cm measured by a calibrated grid, and then, we placed the ointment in the inferior cul-de-sac. The ointment consists of 0.3% ofloxacin, liquid paraffin, white petrolatum, and purified lanolin as its base. The eyes were closed for 30 s, and the eyelids were then wiped only once to remove the ointment that spilled onto the eyelid skin. Subjects were instructed not to wipe their eyelids after this. The measurements just obtained were repeated 2, 5, 10, 20, 30, 40, 50, 60, 90, 120, 180, and 240 min after the administration. All measurements were conducted on the same day at the Tsukuba University Hospital in a room in which the temperature was maintained at 19.8°C±0.8°C and the humidity was 38.8%±0.8%.
In this study, only the right eye was used for the measurements, because it has been shown that aberration patterns are generally symmetric between left and right eyes of the same subject.32,33 The obtained data were analyzed by using repeated-measures analysis of variance (ANOVA) to assess the time course of changes in each parameter over 4 h. If significant differences were observed, the Dunnett post hoc test for multiple comparisons was performed to find time points showing significant difference from the baseline value. In addition, the relationships between ocular aberration and visual function parameters were assessed by using the Pearson correlation test. All statistical analyses were performed using SPSS version 15.0J software (SPSS, Inc., Chicago, IL).
Results
There was a significant time course of changes in FVA, VMR, and minVA during the 4-h study period (all P<0.001, repeated-measures ANOVA). Multiple comparison analysis showed that these visual function parameters significantly deteriorated at 2-, 5-, 10-, and 20 min after administration of eye ointment in comparison with the baseline values (P<0.001, P<0.001, P<0.001, and P=0.011, respectively, for FVA; P<0.001, P<0.001, P<0.001, and P=0.011, respectively, for VMR; and P<0.001, P<0.001, P=0.001, and P=0.011, respectively, for minVA, Dunnett post hoc test). They gradually returned toward the preadministration level after this (Figs. 1–3). No significant time course of changes in blink numbers was observed over the study period (P=0.595, repeated-measures ANOVA; Fig. 4).
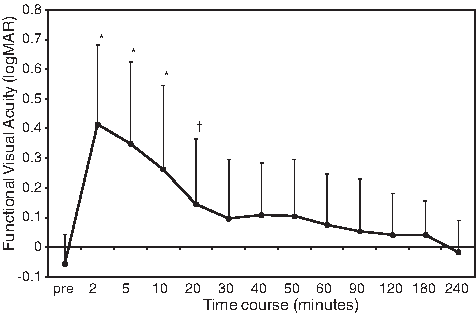
Time course of changes in functional visual acuity (FVA) after administration of eye ointment. FVA significantly deteriorated at 2-, 5-, 10-, and 20 min after administration of eye ointment, and returned toward the preadministration level after that. *P<0.001, †P=0.011 (Dunnett post hoc test): significant differences in comparison with the baseline value. Graphs are expressed as the mean±standard deviation (SD).
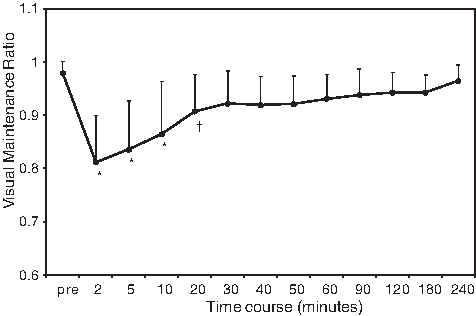
Time course of changes in visual maintenance ratio (VMR) after administration of eye ointment. VMR deteriorated at 2-, 5-, 10-, and 20 min after administration of eye ointment, and returned to the baseline level after that. *P<0.001, †P=0.011 (Dunnett post hoc test): significant differences in comparison with the baseline value. Graphs are expressed as the mean±SD.
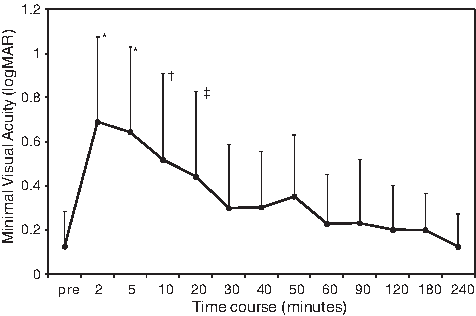
Time course of changes in minimal visual acuity (minVA) after administration of eye ointment. MinVA significantly deteriorated at 2-, 5-, 10-, and 20 min after administration of eye ointment, and gradually returned to the baseline level after that. *P<0.001, †P=0.001, ‡P=0.011 (Dunnett post hoc test): significant differences in comparison with the baseline value. Graphs are expressed as the mean±SD.
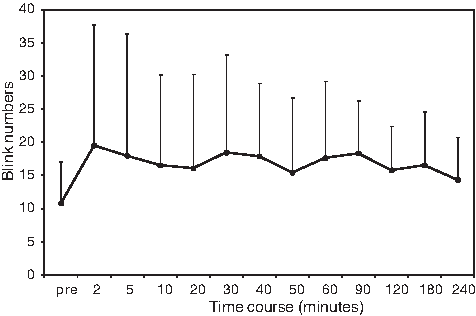
Time course of changes in blink numbers during a 60-s testing period after administration of eye ointment. No significant time course of changes in blink numbers was observed over the study period (P=0.595, repeated-measures analysis of variance). Graphs are expressed as the mean±SD.
All components of ocular wavefront aberration such as second-, third-, fourth-, and total higher-order RMS significantly changed during the study period (all P<0.001, repeated-measures ANOVA). A multiple comparison analysis revealed that each component significantly increased at 2- and 5 min after administration of eye ointment in comparison with the baseline values (P<0.001 and P=0.012 for second-order RMA, both P<0.001 for third-order RMS, P<0.001 and P=0.001 for fourth-order RMS, and both P<0.001 for total higher-order RMS, Dunnett post hoc test). All aberrations returned to the preadministration level after that.
There was a significant time course of changes in FI during the study period (P<0.001 for FI of second-order RMS and P=0.001 for FI of total higher-order RMS, repeated-measures ANOVA). The FIs significantly increased at 2- and 5 min after administration (P=0.002 and P=0.011 for FI of second-order RMS, and P=0.014 and P=0.002 for FI of total higher-order RMS, Dunnett post hoc test), and returned to the preadministration level after that. No significant changes were observed in SI over the study period after administration of eye ointment (P=0.419 for SI of second-order RMS and P=0.960 for SI of total higher-order RMS, repeated-measures ANOVA).
Furthermore, visual function parameters such as VMR, FVR, and minVA were analyzed in relation to ocular aberration parameters and blink numbers at 2 min after the application of eye ointment, in which both visual function and ocular aberration severely deteriorated. As a result, all visual function parameters were significantly correlated with blink numbers (Pearson's correlation coefficient; r=− 0.76, P=0.017 for FVA, r=0.79, P=0.013 for VMR, and r=−0.62, P=0.040 for minVA), and VMR showed a significant correlation with changes in second-order RMS (r=−0.60, P=0.049; Table 1).
Significant correlation by the Pearson correlation test.
FI, fluctuation index; SI, stability index; FVA, functional visual acuity; VMR, visual maintenance ratio; minVA, minimal visual acuity; RMS, root-mean-square.
Discussion
In Asia, ofloxacin eye ointment is one of the most frequently used eye ointments,10,18,34–37 so it was employed as a representative drug in this study. As shown in the results, visual function parameters such as FVA, VMR, and minVA significantly deteriorated for 20 min after the administration, and gradually returned toward the baseline levels after that. Although not statistically significant, the mean value at each time point was still worse for several hours, and FVA did not completely reach the baseline value even at the end of the 4-h study period. These findings apparently imply that eye ointment severely affects visual function. In addition, the mean FVA up to 10 min after administration of eye ointment was worse than 0.155 logMAR (=the decimal VA of 0.7) that is required to drive in Japan. This means that actual VA during10 min after the administration of eye ointment is not adequate for driving. Surprisingly, in minVA, the mean value was worse than 0.155 logMAR until 180 min after administration of eye ointment. That is, patients having an eye ointment treatment cannot continuously maintain a stable VA marking better than 0.155 logMAR during 3 h. Therefore, the result suggests that patients should not drive during 3 h after the eye ointment administration. We have to emphasize that the present results were obtained from normal volunteers with originally good VA. If subjects have some ocular diseases such as cataract, glaucoma, corneal opacity, and vitreoretinal abnormality, their VAs easily fall below the critical level and the reduction may last longer. Hence, practitioners should take account of such influences before prescription.
As for ocular aberration, all components such as second-, third-, fourth-, and total higher-order RMS significantly increased during 5 min after administration of eye ointment, and then returned to the preadministration level. FIs of second-order and total higher-order RMS also increased during 5 min after administration. These results mean that eye ointments considerably influence not only higher-order aberrations but also lower-order aberrations, and both aberrations become unstable in the early phase after the administration. In order to examine how these deteriorations of ocular optical quality affect visual function, we investigated the relationship between optical quality parameters and visual function parameters. As a result, VMR was significantly associated with changes in second-order RMS. FVR and minVA also tended to deteriorate with increases in second-order RMS, although there were no statistical significances. No other relationships especially between visual function parameters and higher-order aberrations were found. It is reasonable that the visual function parameter was affected by lower-order aberration, because the FVA testing system employed 100% contrast optotypes. On the other hand, it is known that increases in higher-order aberration are well associated with reduction in contrast sensitivity function and low contrast acuity in eyes with various pathologic conditions. This may be the reason that higher-order aberrations did not significantly affect visual function parameters which were assessed by high contrast optotypes in the present study. Further research with contrast sensitivity testing may clarify the influences of higher-order aberrations on visual function after administration of eye ointment.
As described earlier, the deterioration of visual function after administration of eye ointment is partially justified by the increases in lower-order aberrations. However, the pattern and trend of the time-wise changes were somewhat different between ocular aberration and visual function parameters. For example, the duration of the deterioration was longer in visual function parameters than in ocular aberration parameters. Thus, there is a possibility that other unexamined factors such as light scattering and pupil size also contribute to the deterioration of visual function. Unfortunately, we did not examine these factors in this study. Further studies with additional optical quality parameters should be conducted to elucidate the mechanism underlying visual degradation after administration of eye ointment in more detail.
We previously investigated the influence of the same eye ointment (Tarivid) on wavefront aberration over a 12-h study period, and found that ocular aberration returned to the baseline levels after prominent increases at 5 min, but fluctuated for several hours and slightly increased again around 6 h after application of eye ointment. 38 The exact reason for the fluctuation and re-increase of ocular aberration during 6 h is still unknown. We speculated that the ointment adhered especially to the eyelid, which spilled over from the palpebral space immediately after its instillation into the conjunctival sac, gradually melted and moved onto the ocular surface accompanied by blinks, and, finally, mixed again with tears. Consequently, this process deteriorated the regularity and stability of tear film after some intervals. If the subjects were instructed not to wipe their eyelid margins throughout the study in the present study as well as the previous one, ocular aberration would fluctuate and re-increase by re-inflow and re-distribution of ointment on the ocular surface, and this would complicate the interpretation of obtained data. Therefore, in the present study, the eyelids were wiped only once, 30 s after the administration, to remove the ointment that spilled onto the eyelid. As expected, the fluctuation and re-increase of ocular aberration were not found during the study period in the present investigation, and this was very helpful to simply understand that the influence of eye ointment remained in the conjunctival sac on ocular aberration.
There were also significant correlations between visual function parameters and blink numbers in the present study. In other words, the higher the blink rate was, the better the visual function parameters were. Although the true reason for this relationship is unclear, it should be noted that SI of second-order aberration showed an upward curve at 2 min after administration of eye ointment. This implies that lower-order aberrations tended to increase while the eyes were kept open. Therefore, frequent blinks appeared to work well to inhibit the increases in lower-order aberrations during the eye opening. This may explain the reason that patients with higher blink rates achieved better visual function in this study.
One of the drawbacks of this study is that the FVA testing and wavefront aberrometry were separately performed. To our knowledge, no instrument that is able to simultaneously measure both of these parameters is available. Although we assessed FVA immediately after wavefront aberrometry, there was a lag of approximately 30 s between the measurements. A simultaneous dynamic evaluation method of ocular wavefront aberration and FVA measurements should be developed to provide further relationships between these parameters. Another weakness of our study is the small sample size. All parameters examined in this study showed a large standard deviation. Such individual variations may also contribute to the present results that demonstrated relatively poor associations between visual function and optical quality parameters. The current results should be confirmed in a larger study population.
In conclusion, we elucidated for the first time the influence of eye ointment on dynamic changes in visual function using the FVA measurement system, which was quite useful in evaluating unstable vision of eyes receiving eye ointment. All visual parameters were significantly reduced for 20 min after administration of eye ointment. Surprisingly, the minVA during the testing period was worse than 0.155 logMAR, which is the threshold required for driving purposes, until 180 min after administration of eye ointment. On the basis of the current findings, driving or any other procedures requiring a high quality of vision is not recommended for several hours after the administration. Especially in those cases in which the frequent use of eye ointment is required, it is probable that the visual degradation becomes severe. It is, thus, crucial for practitioners to definitely inform patients of such impact when prescribing eye ointments. In addition, increases in lower-order aberration and low blink rates were associated with the declines in FVA. However, the observed impairments in visual function could not be explained only by these factors. The mechanism leading to the visual deterioration after administration of eye ointments should be further studied.
Footnotes
Author Disclosure Statement
The authors have no commercial or proprietary interest in any of the companies, products, or methods described in this article.