
Abstract
Abstract
Purpose:
The purpose of this study was to evaluate the ocular distribution of intravenously administered colistin in a rabbit uveitis model.
Methods:
Colistin, a polypeptide antibiotic against the multidrug-resistant (MDR) Gram-negative organisms, was given intravenously to rabbits at 5 mg/kg of body weight starting 24 h after induction of uveitis by intravitreal endotoxin injection. Colistin concentrations were determined by high-performance liquid chromatography–mass spectrometry assay in the aqueous humor, vitreous humor, and plasma 0.5, 3, 6, and 24 h after administration of a single dose.
Results:
The maximum colistin concentrations (mean±standard deviation) were found 0.5 h after the end of the intravenous administration and were 9.48±2.0 μg/mL in plasma and 0.62±0.07 μg/mL in the aqueous humor of the inflamed eye. After 24 h, no drug was detectable in the aqueous of the inflamed eyes. Colistin was undetectable in the aqueous of contralateral normal eyes at all time points. Drug concentrations in all the vitreous samples from both inflamed and normal eyes were undetectable, except at the 3-h inflamed eye group, and a colistin concentration of 0.02±0.01 μg/mL was found. Plasma levels of colistin fell to 0.93±0.07 and 0.24±0.08 μg/mL, after 3 and 6 h, respectively, and were not detectable 24 h after the given dose.
Conclusions:
In our model, colistin did not reach therapeutically relevant levels in the aqueous and in the vitreous humor of rabbit eyes. The findings suggest a limited role for intravenously administered colistin in the treatment of Gram-negative bacterial endophthalmitis.
Introduction
A
The common Gram-negative organisms causing endophthalmitis include species of Pseudomonas, Haemophilus, Klebsiella, and Proteus. Intravitreal ceftazidime or amikacin is commonly used for the empiric treatment of Gram-negative organisms in endophthalmitis. In the Endophthalmitis Vitrectomy Study (EVS), 11% of Gram-negative bacteria were resistant to both amikacin and ceftazidime. 6
The management of the growing multidrug-resistant (MDR) Gram-negative organisms is a tough situation. Over the last few years, however, resistance to many other antibiotics and limited development of new antibiotics have resulted in becoming acquainted again with an old antibiotic named “colistin.” Colistin (also known as polymyxin E) is a cationic polypeptide antibiotic belonging to the polymyxin group of antibiotics with activity mainly against the MDR Gram-negative organisms such as Pseudomonas aeruginosa, Klebsiella pneumoniae, and Acinetobacter baumannii.10,11 Colistin is actually administered as a prodrug, colistin methanesulfonate (CMS), and acts on the bacterial cell membrane resulting in increased cell permeability and cell lysis. 12 The use of colistin had almost stopped 3 decades ago due to the high incidence of nephrotoxicity and neurotoxicity. 13 However, in recent studies, colistin has been found to be efficacious with lower toxicity and is increasingly being used as salvage therapy in patients with MDR Gram-negative bacterial infections. 12
The best method to obtain therapeutic amounts of drugs to the posterior segment and to overcome the ocular barriers is the intravitreal administration, which achieves significant concentrations with minimal systemic exposure. However, the intravitreal mode of administration has drawbacks like frequent administration, hemorrhage, retinal detachment, and endophthalmitis.14,15 In addition, retinal photoreceptor cells are sensitive to both offending pathogens and the resulting inflammatory response and to high doses of antimicrobial agents administered locally to treat the infection.16,17 Therefore, based on this issue, systemic administration may be a mode of administration for treating posterior segment diseases in many sight-saving attempts. 18
Detailed knowledge of the pharmacokinetics of colistin in ocular inflammation will provide a base for rational treatment decisions. In the present study, the penetration of colistin into the vitreous humor and aqueous humor of rabbit eyes following intravenous administration was evaluated. For that purpose, liquid chromatography–mass spectrometry (LC-MS) assays for the determination of colistin concentrations in the aqueous humor, vitreous humor, and plasma had to be developed.
Methods
Animals
Twenty adult New Zealand white rabbits weighing between 3.0 and 3.5 kg were used in this study. They were provided by an authorized breeding center and were kept in individual cages under well-defined and standardized conditions. All eyes were initially examined with a handheld slit lamp. Only animals without any signs of ocular inflammation were included. This study was performed at Konya Training and Research Hospital, Department of Ophthalmology, Konya, Turkey. Animals were treated in accordance with the Association for Research in Vision and Ophthalmology's Statement for the Use of Animals in Ophthalmic and Vision Research.
Anesthesia
Proparacaine hydrochloride 0.5% (Alcaine, Alcon) eye drops were used for topical anesthesia. Animals were sedated by intramuscular injection of 35 mg/kg ketamine hydrochloride (Ketalar; Pfizer) and 10 mg/kg xylazine (Xylazinbio; Bioveta).
Induction of experimental uveitis
After performing topical anesthesia, 100 ng of lipopolysaccharide from Escherichia coli (Sigma Aldrich; L4391) diluted in 10 μL of sterile saline solution was injected through the sclera into the midvitreous using a 30-gauge (G) needle connected to a Hamilton syringe. The injection was performed in the right eye of each animal, taking care to avoid damage to the lens. The left eyes were control groups. Inflammation was evaluated by clinical observation of the iris and conjunctival hyperemia.
Preparation of the antibiotic for intravenous injection
Colistin (Colymycin; Kocak Pharma) was reconstituted in sterile 0.9% sodium chloride to a concentration of 1.5 mg/mL and stored in a refrigerator between 2°C and 8°C. Twenty-four hours after induction of uveitis, 20 rabbits were sedated and given 5 mg/kg colistin over 30 min intravenously with an infusion pump through the left marginal ear vein. The dose was selected according to former studies in animals.19,20
Sample collection
Five animals per time point were euthanatized and the aqueous humor, vitreous humor, and blood samples were collected at 30 min, 3 h, 6 h, and 24 h after infusion of the drug. Blood was collected by puncture of the marginal right ear artery and centrifuged to obtain plasma (0.2 mL). Aqueous humor (0.2 mL) was drawn from the eyes with a tuberculin syringe using a 30G needle. Vitreous humor (0.2 mL) was obtained by a 15G needle mounted on a 5-mL syringe, introduced at 3.0 mm of the limbus, and directed toward the center of the globe, as previously described. 21 Samples were immediately stored at −80°C until analysis.
Analytical procedures
A sensitive and selective liquid chromatography–mass spectrometry (Shimadzu, LCMS-8030 Triple Quadrupole Liquid Chromatograph–Mass Spectrometer) method for determination of colistin in rabbit plasma, aqueous and vitreous humor was developed. The mass spectrometer was operated in the positive-ion mode. Ions were analyzed by multiple reaction monitoring. Colistin sulfate (1267.6 g/mol) standard was obtained from Sigma Aldrich (C4461-100 mg). Sample preparation: after thawing at room temperature (22°C), 200 μL of the sample was diluted with 600 μL of acetonitrile, followed by vortex mixing and centrifuged for 5 min at 10,000 g. The supernatants were transferred to clean tubes. The supernatants were evaporated to dryness under a gentle nitrogen stream in a heating block at 45°C, and the residues were redissolved in 200 μL of formic acid 0.1% (vol/vol) in water and analyzed by LC-MS/MS. The flow rate was 0.2 mL/min, and the injection volume was 20 μL. The calibration curve ranged from 0.012 to 15 μg/mL, with a lower limit of quantitation of 0.012 μg/mL.
Statistical analysis
Statistical analysis of the data was performed using commercial software (Statistical Package for Social Science, version 15.0; SPSS, Inc.). Correlations between concentrations in the aqueous humor or vitreous and those of plasma were performed by linear regression analysis. Statistical significance was considered when P<0.05. Results are represented as mean±standard deviation (SD) and median values together with the minimum and maximum concentrations.
Results
Concentrations of colistin in the aqueous humor, vitreous humor, and blood over time from the end of drug administration are shown in Table 1. The maximum concentrations were found within 0.5 h after the end of the intravenously given colistin and were 9.48±2.0 μg/mL in plasma and 0.62±0.07 μg/mL in the aqueous humor of the inflamed eye. A positive correlation was found between concentrations in the aqueous humor and those of plasma (rs=+0.490; P=0.001); however, no correlation was found between plasma and vitreous humor (rs=0.057; P=0.309). Three and 6 h after intravenous injection of a single dose of 5 mg/kg colistin, the mean drug concentration in the aqueous of the inflamed eye was 0.45±0.05 and 0.38±0.08 μg/mL, respectively. After 24 h, no drug was detectable in the aqueous of the inflamed eyes. Colistin was undetectable in the aqueous of contralateral normal eyes at all time points (Fig. 1).
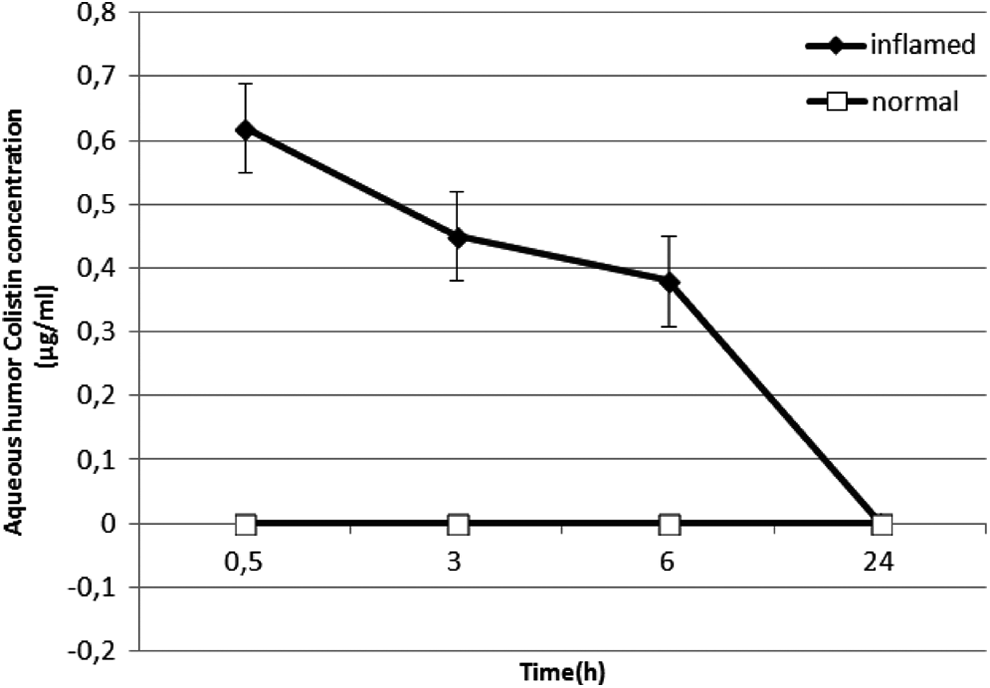
Mean (±SD) colistin concentration over time in the aqueous of rabbits given a single intravenous dose of colistin at 5 mg/kg of body weight.
Time (h), after the end of the infusion.
Values expressed as mean±standard deviation (median) [minimum–maximum concentrations].
Under LC-MS detection levels.
Drug concentrations in all the vitreous samples from both inflamed and normal eyes were undetectable with one exception; in one inflamed eye, a colistin concentration of 0.02±0.01 μg/mL was found at 3 h.
Thirty minutes after administration of colistin, the mean drug concentration in plasma was 9.48±2.0 μg/mL. It fell to 0.93±0.07 and 0.24±0.08 μg/mL, after 3 and 6 h, respectively. The plasma level of the drug was not detectable 24 h after the colistin dose (Fig. 2).
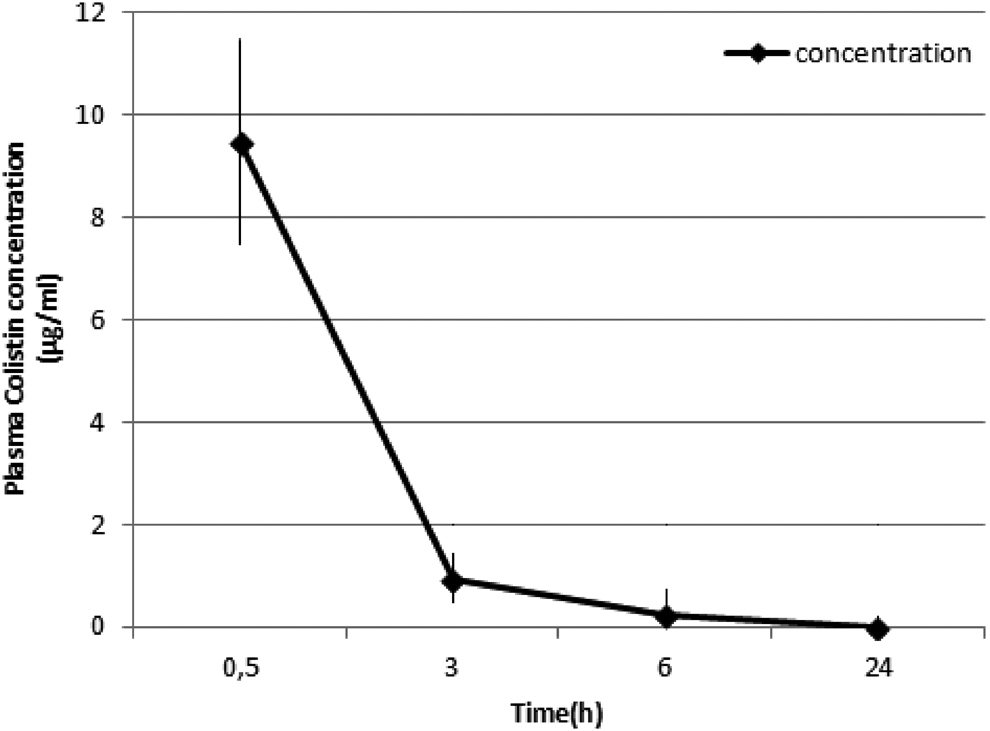
Mean (±SD) colistin concentration over time in plasma of rabbits given a single intravenous dose of colistin at 5 mg/kg of body weight.
Discussion
In this study, we aimed to characterize the penetration into ocular compartments of systemically administered colistin in a rabbit uveitis model. Several high-performance liquid chromatography assays for the measurement of colistin concentrations in plasma, urine, and brain tissue have been described in the literature.19,22 No assay for the determination of colistin in ocular tissues has been found.
The present results reveal that systemic administration of colistin in inflamed rabbit eye was accompanied by inefficient penetration in both the aqueous humor and the vitreous humor. The concentrations were below the minimum inhibitory concentrations (MICs) for most causative pathogens of endophthalmitis. Many authorities consider susceptibility to colistin if the respective MIC90 of colistin is a maximum of 2 μg/mL against a variety of Gram-negative bacteria, including E. coli, Klebsiella spp., Enterobacter spp., A. baumannii, and P. aeruginosa. 13
Our findings suggest that colistin does not penetrate the intact blood–eye barrier. With a sensitive LC-MS assay, drug levels were undetectable in the aqueous and vitreous of normal eyes. This may be explained in part by the drugs high molecular weight (1163 g/mol) 23 as the blood–eye barrier is thought to be impermeable for molecules exceeding 500 g/mol. 24 In addition, our model suggests that intraocular penetration of colistin is critically dependent on disruption of the blood–eye barrier. The degree of break down of the blood–eye barrier in inflammation may be critical for the intraocular deposition of antimicrobials. Green et al. reported that the absence of drug in normal rabbit eyes indicated that inflammation of ocular structures was crucial for drug penetration. 25
Romera et al. 26 emphasized that prompt administration of intravenous antibiotic therapy was an important point in the management of endogenous endophthalmitis. Systemic antibiotics treat distant foci of infection and prevent continuing bacteremia; in this way, the risk of the unaffected eye getting infected will be reduced. On the other hand, Ferencz et al. reported that some potentially effective antibiotics (eg, vancomycin) did not penetrate into the vitreous, due to the protective effect of the blood–eye barrier and they concluded that intraocular inflammation increased the permeability of the blood–eye barrier, enhancing penetration of systemic antibiotics into the vitreous cavity. Nevertheless, the intravitreal levels were below the MICs for many ocular pathogens. 27
Many of the drugs used in ophthalmology are less permeable across the blood–eye barrier due to their organic cation nature, so as to achieve necessary therapeutic concentrations at the site of action, large drug doses are required.18,28 Further investigations are needed to determine the mechanisms limiting the blood–eye barrier penetration of colistin so that appropriate measures can be taken to enhance colistin exposure for the treatment of sight-threatening ocular infections.
In established endophthalmitis, vitrectomy is indicated and followed by intravitreal injection of an antimicrobial agent. In cases where vitrectomy has to be delayed or where it may be contraindicated, systemic administration may be a mode of administration for controlling the endophthalmitis. 29 Additionally, in endogenous endophthalmitis that results from hematogenous dissemination, adjunctive systemic treatment is also indicated. 30
When adapting the results of this rabbit model of iatrogenic uveitis to human Gram-negative bacterial endophthalmitis, one must take into account that the disruption of the blood–eye barrier resulting from endotoxin induced uveitis may differ from that found in Gram-negative bacterial endophthalmitis. Therefore, studies in animals with Gram-negative bacterial endophthalmitis are needed to further evaluate the drugs' potential.
The concentration of colistin in plasma declined rapidly over the 3-h period. Additional studies with multiple dosing would be carried on to more clearly identify the potential of colistin to accumulate within the eye. The present study fails to confirm this hypothesis as there are no relevant data found.
In conclusion, this study demonstrated that colistin did not reach therapeutically relevant levels in the aqueous and in the vitreous humor of rabbit eyes. The findings suggest a limited role for intravenously administered colistin in the treatment of Gram-negative bacterial endophthalmitis; therefore, further studies would be required to identify the intravitreal safe and effective dose of colistin by in vitro cell culture and in vivo animal studies.
Footnotes
Acknowledgments
This work was supported by grants from the Konya Training and Research Hospital (KTRH-28), Konya, Turkey.
Author Disclosure Statement
The authors have no financial or proprietary interest in any material or method mentioned. The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.