
Abstract
Abstract
Purpose:
To determine the vitreous and aqueous concentrations of brimonidine after topical application of the ophthalmic solution 0.1%.
Methods:
The prospective observational case series included patients with an idiopathic epiretinal membrane or macular hole who were scheduled for a pars plana vitrectomy. Brimonidine tartrate ophthalmic solution 0.1% was topically administered twice daily for 1 week preoperatively. Vitreous and aqueous humor was collected before vitrectomy, and then, the brimonidine concentration was measured with liquid chromatography tandem spectrometry (LC/MS/MS).
Results:
Twenty-four patients (19 phakic eyes and 5 pseudophakic eyes) were enrolled. The mean concentrations in the aqueous humor and vitreous were 336.0±276.2 and 4.8±3.2 nM, respectively. A significant relationship was observed between the vitreous and aqueous samples (P=0.034, R2=0.22). Nineteen (79%) of the 24 eyes showed more than 2 nM of brimonidine tartrate concentration in the vitreous. In the phakic eyes, the mean concentration of brimonidine in the vitreous was 4.9±3.3 nM, while the mean concentration in the pseudophakic eyes was 4.1±2.4 nM, demonstrating no significant difference between pseudophakic and phakic eyes (P=0.59).
Conclusions:
After 1 week of dosing, in most of the patients who topically received brimonidine tartrate 0.1%, the concentration in the vitreous of the molecule was above 2 nM, which is known to activate neuroprotective α-2 receptors in animal retina. The drug penetration into the vitreous seems to be independent of lens status.
Introduction
G
Brimonidine has a high selective affinity for the α2-adrenergic receptor, lowering IOP by 2 mechanisms: the suppression of aqueous humor production and the promotion of uveoscleral outflow. In addition, several experimental studies demonstrated that brimonidine attenuates the neurodegenerative pathway. For instance, brimonidine significantly protects optic nerve degeneration in a rat optic nerve crush model and in an acute ischemic model.6,7 A randomized trial of brimonidine versus timolol (the Low-Pressure Glaucoma Treatment Study) showed that the brimonidine 0.2%-treated group showed less progression of visual field loss than the timolol-treated group. 2 Moreover, brimonidine tartrate ophthalmic solution 0.15% significantly improves retinal vascular autoregulation in normal-tension glaucoma patients. 8
To confirm whether the concentration of brimonidine in the vitreous is enough to exhibit neuroprotection in the retina, quantitative measurement of the drug in ocular media has been carried out after the topical administration of brimonidine tartrate 0.2% and 0.15%.9,10 Most of the brimonidine tartrate-administered eyes showed the concentration of more than 2 nM in the vitreous, which is known to activate neuroprotective α-2 receptors in animal retina. 11 However, the concentrations of the human aqueous humor or vitreous after the topical administration of ophthalmic solution 0.1% have not been evaluated. In this study, we topically applied brimonidine tartrate ophthalmic solution 0.1% to Japanese volunteers and measured its concentrations in the aqueous humor and vitreous.
Subjects and Methods
This clinical observational study was approved by the University of Fukui Institutional Review Board (IRB) and complied with the tenets of the Declaration of Helsinki. The protocol and the possible risks and benefits of the interventions were explained to all participants before enrollment. All patients provided written informed consent. This study was registered with the University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR) of Japan (ID UMIN000009982; date of access and registration, February 10, 2013).
Patients who were scheduled for a pars plana vitrectomy to treat idiopathic epiretinal membrane or macular hole were invited to participate in this study. All patients were older than 20 years. Exclusion criteria were intraocular inflammation; vitreous hemorrhage; proliferative diabetic retinopathy; corneal epithelial disorder; a history of hypersensitivity or side effects, including conjunctivitis, punctate keratitis, and blepharitis following treatment with α2 stimulants; and determination by a physician that participation would be inappropriate.
Brimonidine tartrate ophthalmic solution 0.1% (AIPHAGAN® Ophthalmic Solution 0.1%; Senju Pharmaceutical Co., Ltd., Osaka, Japan) was provided to the patients with an idiopathic epiretinal membrane or macular hole, who were instructed to instill the drug to their eyes twice daily, in accordance with the manufacturer's instruction in the package insert, for 1 week until 1 day before surgery. On the operation day, eye drops were carried out in the morning (at 8:00 a.m.) and at ∼2 h before surgery. Two patients served as controls and did not receive the ophthalmic solution. The pars plana vitrectomy was performed under retrobulbar anesthesia with a standard 4-port technique by one surgeon (T.T.). In eyes associated with lens cataract, phacoemulsification and aspiration with intraocular lens implantation were performed during surgery. Samples of aqueous humor (100 μL) and vitreous (500 μL) were obtained from the anterior chamber and vitreous cavity, respectively. To avoid sample dilution, the infusion line was closed until sample collection from the vitreous. Vitreous specimens were obtained from the area near the retina and optic disc using a 25G vitreous cutter, which was directed posteriorly toward the optic head. These samples were stocked in Eppendorf tubes at −80°C. Samples were analyzed at an independent bioanalytical facility (LSI Medience Corporation, Tokyo, Japan) for quantitative determination of brimonidine concentrations using liquid chromatography and tandem mass spectrometry. ACQUITY UPLC and Waters Micromass Quattro Premier (Waters, Milford, MA) were used for the analysis. Gradient chromatography was performed with an ACQUITY UPLC BEH Amide column (2.1×50 mm, 1.7 μm; Waters). 5-Chloro-6-(2-imidazolidinylideneamino) quinoxaline was used as an internal standard (IS). All samples were pretreated with solid-phase extract methods before analysis. The aqueous humor (15 or 25 μL) and vitreous body (120 μL) were separately mixed with methanol and pure water. These solutions were applied to an OASIS HLB μElution 96-well plate (Waters) preconditioned with methanol and pure water. After rinsing with pure water, analytes were eluted using acetonitrile. The injection volume was 10 μL. The flow rate was 0.3 mL/min, and methanol/10 mM ammonium formate (2:3) and acetonitrile were used as the mobile phases. Brimonidine and IS were analyzed in a positive ionization mode with the following multiple reaction monitoring transitions: 292.10→212.20 (brimonidine) and 248.20→205.20 (IS). The lower limits of quantitation were 0.024 ng/mL (aqueous humor) and 0.01 ng/mL (vitreous body).
Statistical analyses were performed using JMP 10 (SAS institute, Inc., Tokyo, Japan). The data are shown as mean±standard deviation. We assessed the statistical significances between groups using the Mann–Whitney U-test. Correlations between the levels of brimonidine in the aqueous humor and vitreous were studied by ordinary least-squares regression analysis. For all statistical tests, the significance was considered to be less than 5% (P<0.05).
Results
Thirty-one patients participated in the study; 7 patients were excluded because they failed to use the ophthalmic solution before surgery. Consequently, 24 patients (66.3±9.1 years old, 5 males, 19 females) were evaluated. Nineteen eyes were phakic and 5 were pseudophakic. Patient demographic data are shown in Table 1. The mean interval between the last administration and the sample collection was 2.2±1.3 h. Two samples from other 2 patients who did not receive the ophthalmic solution (negative controls) showed values below the lower limits of quantitation. The mean concentrations in the aqueous humor and vitreous were 336.0±276.2 and 4.8±3.2 nM, respectively. Nineteen (79%) of the 24 eyes showed more than 2 nM of brimonidine concentration in the vitreous. In the phakic eyes, the mean concentrations in the aqueous humor and vitreous samples were 345.2±283.2 and 4.9±3.3 nM, respectively. In pseudophakic eyes, the mean concentrations in the aqueous and vitreous samples were 304.6±279.5 and 4.1±2.4 nM, respectively. No significant differences of the brimonidine concentrations in the aqueous humor (P=0.78) or vitreous (P=0.59) were found between phakic versus pseudophakic eyes (Fig. 1). There was a significantly positive correlation between the levels of brimonidine in the aqueous humor versus vitreous (P=0.031, R2=0.223, OLS regression analysis) (Fig. 2).
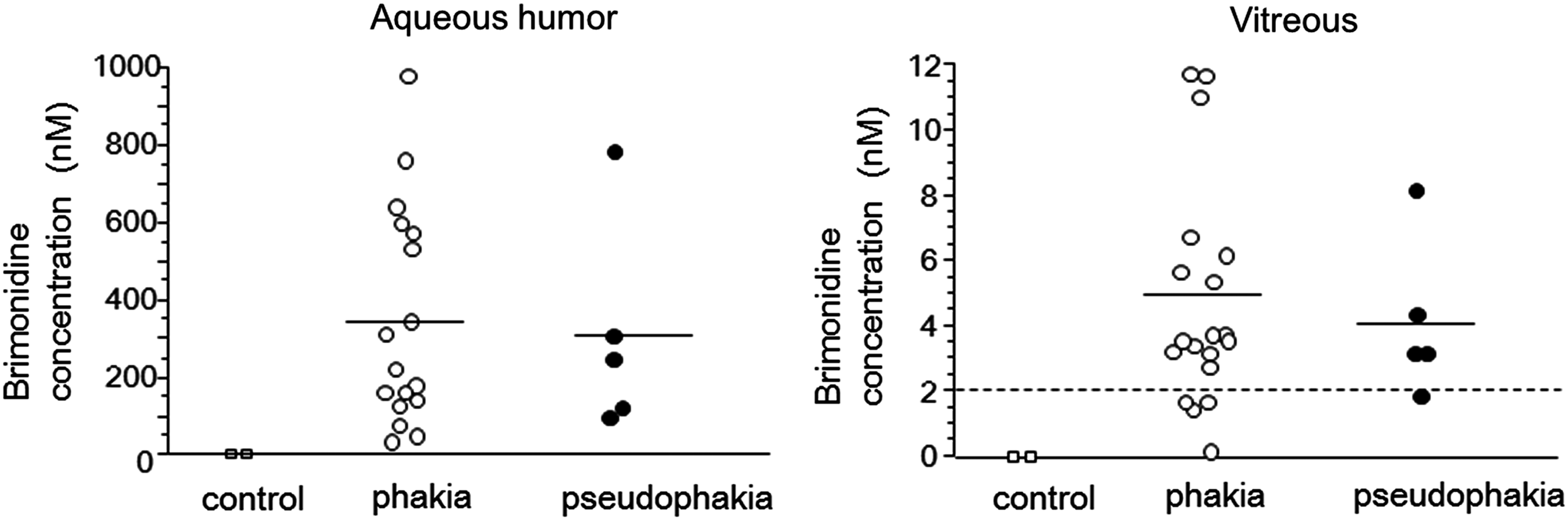
Scatterplot of brimonidine concentrations in the aqueous humor and vitreous of controls (no eye drops instilled) and patients with phakia and pseudophakia. The solid horizontal line in each column indicates the mean of the included data points, and the dotted line horizontal to the x-axis denotes the 2 nM brimonidine concentration shown to be neuroprotective in animals. There was no significant difference in the levels of brimonidine between the phakic and pseudophakic eyes (P<0.05, the Mann–Whitney U-test). Open and filled circles indicate phakic and pseudophakic eyes, respectively.
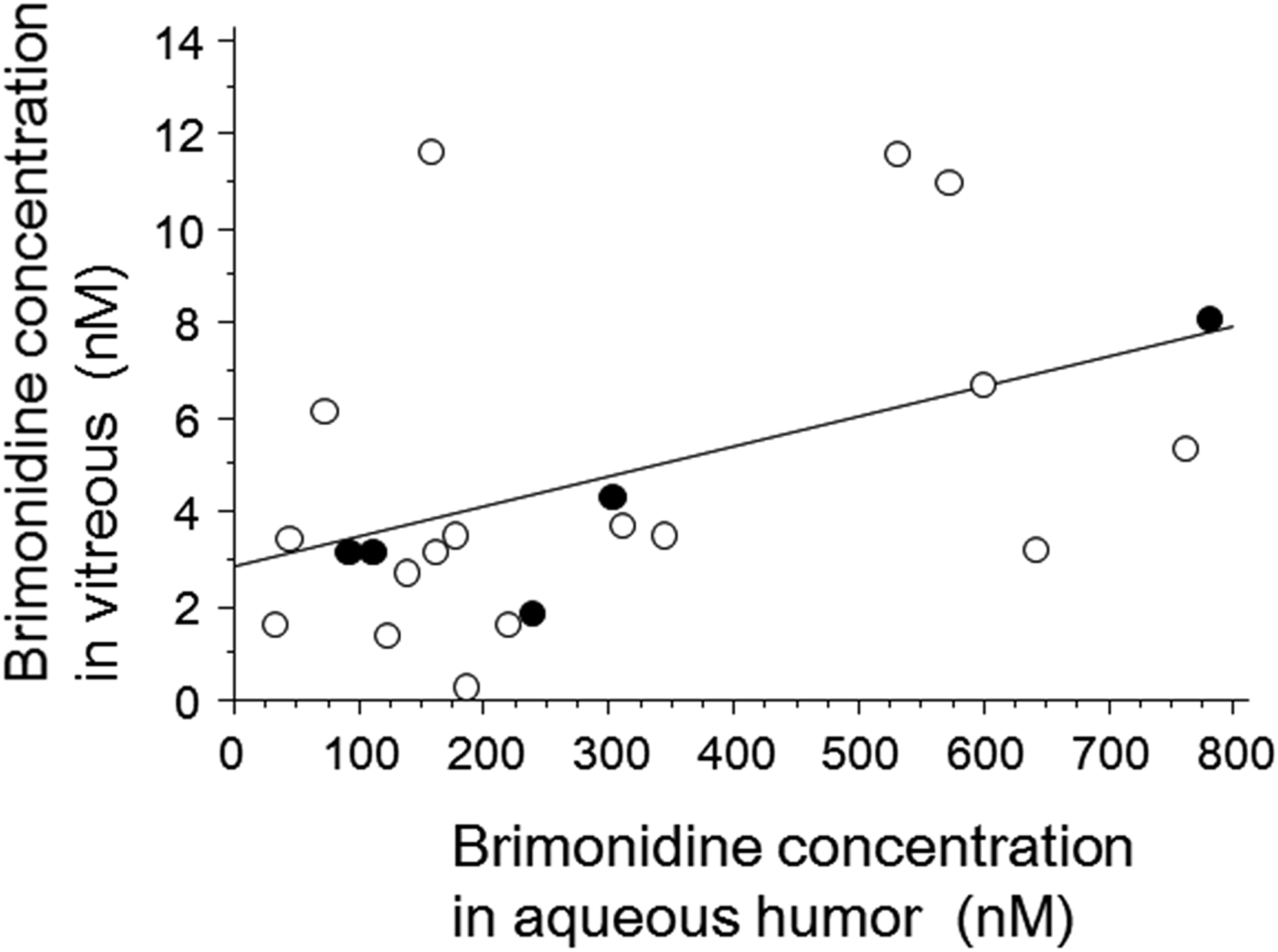
Linear correlation between brimonidine levels in the aqueous humor and those in the vitreous. The relationship is significant (R2=0.223, P=0.031, ordinary least-squares regression analysis). Open and filled circles indicate phakic and pseudophakic eyes, respectively.
No cases encountered major postoperative complications such as infectious endophthalmitis, vitreous hemorrhage, or retinal detachment. Blood pressure (BP; systolic/diastolic) before the beginning of administration and just before surgery was 137.5±15.7/83.7±10.9 and 127.3±21.0/73.8±8.7 mmHg, respectively. The average pulse rates before the beginning of administration and just before surgery were 70.2±21.2 and 74.3±7.8, respectively. The differences between these time points were not significant (systolic BP, P=0.23; diastolic BP, P=0.34; pulse, P=0.24).
Discussion
Before conducting a clinical trial whether the drug has a neuroprotective effect for glaucoma optic neuropathy, the following 3 criteria are required: (1) the target receptors for the drug exist in the retina, (2) the drug exhibits a neuroprotective activity in laboratory studies and promotes the survival of retinal ganglion cells, and (3) the concentration of the drug in the retinal tissue is enough to activate the receptors.9,12 Brimonidine satisfies these 3 criteria. First, immunohistochemical studies have shown that the α2-adrenergic receptors exist in the human retina. 13 Immunoreactivity is observed in the ganglion cell layers of the rat retina. 14 Second, brimonidine promotes the survival of retinal ganglion cells in a rat high IOP model 15 as well as in rat retinal ischemia. 16 Third, the vitreous after the topical administration of the brimonidine tartrate ophthalmic solution 0.2% and 0.15% showed the concentration of more than 2 nM, which is known to activate the neuroprotective α-2 receptors in animal retina. 11 The purpose of our study is whether brimonidine tartrate ophthalmic solution 0.1% satisfies the third criterion. Our present study demonstrated that most of the vitreous samples contained more than 2 nM brimonidine concentration after the topical administration.
In comparison to the report of Kent et al., 9 we measured a relatively lower concentration of brimonidine in the vitreous, ∼40% and 21% in phakic and pseudophakic eyes, respectively. This may be due to the different concentrations of brimonidine tartrate in the 2 studies: 0.2% versus 0.1%. A second possible reason for the difference is that the number of daily administrations may have affected the brimonidine concentration in eyes. In our present study, the ophthalmic solution was administered twice daily for 1 week, while 62% of eyes in their previous report had the ophthalmic solution 3 times daily for 4–14 days before surgery and 4 times on the day of surgery. More frequent and longer duration of the administration may have resulted in the higher concentration in the vitreous. A third possible reason is the difference of races. The eyes of pigmented rabbits show rapid brimonidine elimination from the aqueous humor, whereas the pigmented iris and ciliary body have a higher concentration of brimonidine than the eyes of albino rabbits. 17 Therefore, a higher affinity of brimonidine to melanin may have affected its concentrations in the vitreous of Japanese. As a fourth reason, the difference of the duration between the last eye drop and the sample collection in the surgery may influence the amount of brimonidine in the vitreous. We obtained the samples from all patients at 2 h after the last eye drop, whereas Kent et al. obtained at various time points (2–12 h). Their report showed that the peak was noticed at 2 h after instillation. In their data, it seems that the values of brimonidine decreased time dependently after instillation: those obtained at 2 h were more than 100 nM and those obtained at 12 h were less than 100 nM.
We showed that the amount of brimonidine in the vitreous mostly reached significant levels (above 2 nM), however, the vitreous and retina are not in the same compartment. Thus, the levels of brimonidine in the retina may be different in comparison to that in the vitreous. The data using the animal model demonstrated that the concentrations of brimonidine in the vitreous were extremely lower than that in the retina and choroid. 11 Therefore, it is probable that brimonidine presents more abundantly in the retina than in the vitreous after instillation.
A previous report showed a higher concentration of brimonidine in the vitreous of pseudophakic eyes than in that of phakic eyes although the difference between the 2 groups in their study was not significant. 9 Our present study includes a larger sample size and less variation in each group. A higher concentration of brimonidine in the vitreous of the pseudophakic eyes shown by the previous report seems to be due to a small sample size: In Kent's report, the number of the samples collected at 2, 4, or 6 h after the last instillation was 2 and 3 in phakic and pseudophakic eyes, respectively. Besides, in Kent's report, they collected the samples at different time points, and it may result in unfair comparison between the phakic and pseudophakic eyes. In our data, the samples were obtained at the same time point, and this strengthens the reliability of our finding, that is, no significant difference in the levels of brimonidine between the phakic and pseudophakic eyes. The possible pathway of brimonidine tartrate to the vitreous may be through the periocular tissues or uveoscleral tissues and not through the lens.
Similar to the previous reports using brimonidine tartrate ophthalmic solution 0.2% or 0.15%,9,12 some patients exhibited the concentration of brimonidine less than 2 nM in the vitreous. These findings suggest that the posterior penetration of the topically administered brimonidine tartrate depends on the individuals. Although we cannot determine which factors are involved in the variation, the neuroprotective effect through the activation of α-2 receptors may also depend on individuals.
In conclusion, after the 7-day topical administration of brimonidine tartrate ophthalmic solution 0.1%, most of the Japanese vitreous samples contained the concentration of more than 2 nM shown in animal retinas to activate the α-2 receptor. Lens status did not affect the concentration in the vitreous. Further study is required to reveal the pathway of brimonidine penetration into the vitreous.
Footnotes
Author Disclosure Statement
Y.T. and M.I. received grants, technical support, and provision of information about the measurement method of sample from Senju Pharmaceutical Co. Ltd. S.K. works in Senju Pharmaceutical Co., Ltd.