
Abstract
Abstract
Purpose:
The aim of this study is to report the results of 18 months of follow-up after treatment with accelerated (18 mW/cm2) corneal cross-linking in patients with progressive keratoconus.
Methods:
Forty-two eyes of 42 patients with progressive keratoconus were included in this retrospective study. All patients underwent accelerated corneal cross-linking at an irradiance of 18 mW/cm2 for 5 min (total surface dose 5.4 J/cm2). Visual acuity, topographic findings (Kflat, Ksteep, Kaverage, and apical keratometry), and central corneal thickness were evaluated during the 18-month follow-up period.
Results:
The mean ± standard deviation age of the 16 female and 26 male patients was 24.28 ± 6.32 years (range 14–36). Uncorrected distance visual acuity improved clinically significant from 0.52 ± 0.31 to 0.44 ± 0.25 logMAR (P = 0.031), and corrected distance visual acuity improved clinically significant from 0.34 ± 0.21 to 0.28 ± 0.19 logMAR (P = 0.018). At the last examination during the follow-up period, the flat keratometry (Kflat) decreased from a baseline of 45.65 ± 2.71 to 45.41 ± 2.72 diopters (D) (P = 0.001), the steep keratometry (Ksteep) decreased from 49.20 ± 3.54 to 48.96 ± 3.43 D (P = 0.023), and apical keratometry decreased from 56.62 ± 6.43 to 55.19 ± 5.69 D (P = 0.001), all of them were clinically significant at the 18-month visit. The preoperative values of central corneal thickness changed from 458.95 ± 38.79 to 461.85 ± 41.36 μm 18 months after the operation (P = 0.476).
Conclusion:
The accelerated corneal cross-linking was found to be effective for the stabilization of progressive keratoconus during the 18 months of follow-up visits.
Introduction
K
Corneal collagen cross-linking (CXL) using a combination of riboflavin and ultraviolet A (UVA) was first described by Wollensak et al. This technique halts or slows the progression of the disease by causing the formation of additional covalent bonds within collagen fibrils using photopolymerization, thus increasing the biomechanical stiffening and the biochemical resistance of the cornea.7–13 The conventional procedure for the CXL treatment modality is performed by administering a solution of 0.1% riboflavin and 20% dextran for 30 min in deepithelialized corneas followed by 30 min of 365-nm UVA illumination at 3 mW/cm2 (5.4 J/cm2 dose).1,14,15
Recently, accelerated CXL has been used as a new alternative procedure to conventional CXL. According to the Bunsen–Roscoe law of reciprocity, the solution's biological efficacy in the cornea is similar to that of conventional CXL when higher irradiance UVA light is used in a shorter period of time as they both deliver the same total UVA energy.16–18 There are several accelerated CXL procedures with irradiances between 3 and 30 mW/cm2 and illumination times between 30 s and 3 min.19–24 In the literature, there are a few studies on accelerated CXL with 5 min of illumination at 18 mW/cm2.25,26 The present study evaluated the 18-month results of a protocol for accelerated corneal cross-linking (5 min UVA at 18 mW/cm2) in progressive keratoconus patients.
Methods
Study design and participants
This retrospective study was organized at the Refractive Surgery Department of Beyoglu Eye Research and Education Hospital to assess the efficacy of accelerated CXL in the treatment of progressive keratoconus in 18 months of follow-up visits. The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Local Ethics Committee of the Beyoglu Eye Research and Education Hospital. Written informed consent about the risks and benefits of the treatment was obtained from all patients (or their parents in the case of minors) included in the study.
Forty-two eyes of 42 patients (16 female, 26 male) diagnosed with stage 1 and 2 keratoconus, which shows progression, were included in this study. Progressive keratoconus was described as a maximum keratometry (Kmax) increase of 1 diopter (D) or more, corneal astigmatism increase of 1 D or more, and subjective loss of 1 or more lines in corrected distance visual acuity (CDVA) over a period of at least 6 months. Patients were excluded if they had a history of corneal surgery, connective tissue disease, apical corneal scarring or hydrops, residual or active ocular disease, a history of herpetic keratitis, corneal thickness (with epithelium less than 400 μm), Kmax greater than 65 D, or a history of pregnancy.
Examination protocols
Uncorrected distance visual acuity (UDVA), CDVA, manifest refraction, slit-lamp biomicroscopy, Goldmann applanation tonometry, and funduscopic examinations were performed in the preoperative period and at 1, 6, 12, and 18 months after the operation. All patients were evaluated with a Sirius corneal topography and pachymetry system (Costruzione Strumenti Oftalmici).
Accelerated CXL technique
All procedures were performed under sterile conditions. After topical anesthesia was achieved with 0.5% proxymetacaine hydrochloride eye drops (Alcaine; Alcon Laboratories, Inc.), the central 9 mm of the corneal epithelium was removed using a blunt spatula. Riboflavin (0.1% solution VibeX; Avedro, Inc.) was applied to the corneal bed with a frequency of 1 drop every 2 min for 20 min. After the installation of the riboflavin photosensitizer, the central cornea over a 9-mm diameter was exposed to 365-nm UVA light (Peschke; Meditrade CCL-Vario system) at an irradiance of 18 mW/cm2 (5.4 J/cm2) for 5 min.
At the end of the treatment, the eye was washed with a balanced salt solution, and antibiotic eye drops were applied (moxifloxacin 0.5%, Vigamox©; Alcon Co., Inc.). Then, a silicon-hydrogel bandage contact lens with a 14.0-mm diameter, 8.6-mm base curvature, and an oxygen permeability of 140 barrers (Lotrafilcon B; Air Optix) was worn until the full reepithelialization of the cornea was complete (about between 2 and 5 days). After the treatment, the following medications were prescribed: 0.5% moxifloxacin eye drops (4 times per day for 1 week; Vigamox; Alcon Co., Inc.), artificial tears (4 times per day for 1 month), and Flarex© eye drops (4 times per day 2 weeks after epithelial healing; 0.1% fluorometholone acetate; Alcon Co., Inc.).
Main outcome measures
The following were analyzed to evaluate the effects of accelerated CXL treatment: changes in simulated keratometric values [the flattest meridian (Kflat), the steepest meridian (Ksteep), mean keratometry (Kaverage), and apex keratometry (Kapex)], topographic astigmatism, central corneal thickness, and visual acuity.
Statistical analysis
Statistical evaluation was performed using SPSS software version 20.0 (IBM Corp.). After assessment of normality of all data using the Kolmogorov–Smirnov test, a paired t-test was used to compare the changes between preoperative and postoperative values. A P-value less than 0.05 was considered statistically significant.
Results
Demographic results
Forty-two eyes of 42 patients (16 female, 26 male) were included in this study. The mean age of patients was 24.28 ± 6.32 years (range 14–36).
Visual acuity outcomes
The baseline and postoperative visual acuity outcomes are shown in Table 1. There was no significant change of the mean UDVA and CDVA values at the 1 and 6-month visits (P > 0.05 for all), but a statistically significant increase was detected at the 12 and 18-month visits (P < 0.05 for all). At the last visit (18 months), UDVA remained unchanged in 21 eyes (50.0%), increased by 2 or more snellen lines in 5 eyes (11.9%), increased by 1 snellen line in 11 eyes (26.19%), decreased by 1 snellen line in 4 eyes (9.52%), and decreased by 2 snellen lines in 1 eye (2.38%). The CDVA remained unchanged in 22 eyes (52.38%), increased by 2 or more snellen lines in 6 eyes (14.28%), increased by 1 snellen line in 10 eyes (23.80%), decreased by 1 snellen line in 3 eyes (7.14%), and decreased by 2 snellen lines in 1 eye (2.38%).
Values in bold are statistically significant (P < 0.05).
Comparison of preoperative and first month values.
Comparison of preoperative and sixth month values.
Comparison of preoperative and 12th month values.
Comparison of preoperative and 18th month values.
CDVA, corrected distance visual acuity; CXL, corneal collagen cross-linking; D, diopter; K, keratometry; LogMAR, logarithm of the minimal angle of resolution; μm, micrometer; SD, standard deviation; UDVA, uncorrected distance visual acuity.
Topographic and pachymetric outcomes
The mean Kflat, Ksteep, Kaverage, and apical keratometry showed significant flattening at 12 and 18-month visits (P < 0.05 for all) after the CXL treatment compared with the preoperative measurements (Table 1). Kflat, Ksteep, and Kaverage values increased significantly at the 1-month visit (P < 0.05 for all) and then decreased to the baseline values at the 6-month visit (Table 1). Kapex increased insignificantly at the 1-month visit and decreased with a statistically significant rate at the 6-, 12-, and 18-month visits (P < 0.05 for all) (Table 1 and Fig. 1). No significant difference was found in the corneal astigmatism value during the 18-month follow-up visit compared to the baseline values (P > 0.05 for all) (Table 1). Central corneal thickness revealed a significant decrease at the 1-month visit (P < 0.05), but returned to the baseline values at the 12-month visit and remained stable afterward (P > 0.05) (Table 1).
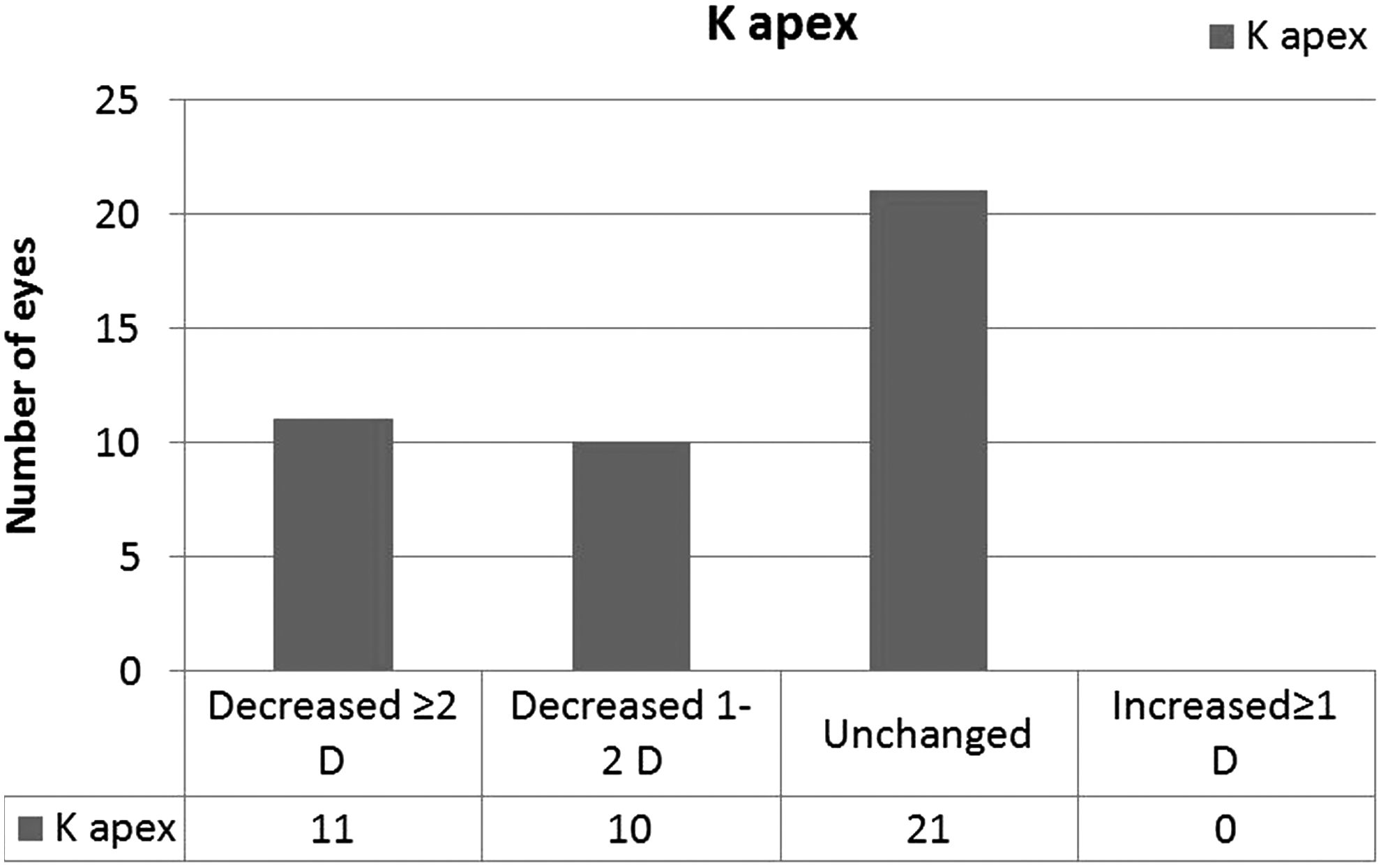
Changes in apical keratometry values between baseline and an 18-month postoperative visit.
Postoperative complications
Most of the patients reported experiencing minor to moderate postoperative ocular pain, because of the deepithelialization of the cornea, which decreased over the first 2–3 days. In some of our patients, mild stromal haze had occurred for 3 months after the CXL, but mild stromal haze regressed with topical steroid treatment. No postoperative complications such as persistent haze or infection were observed.
Discussion
Conventional CXL has already proven its success in stabilizing progressive keratoconus in many long-term studies.1,8,27,28 Ghanem et al. reported that apical, differential, and central keratometry showed a statistically significant decrease, while uncorrected visual acuity (UCVA) and best corrected visual acuity (BCVA) increased significantly 2 years after the standard CXL. 28 Caporossi et al. found that Kmean reduced 2 D, while UCVA and BCVA improved at the 48-month visit after treatment with conventional CXL. 8 Recently, Raiskup et al. reported the 10-year outcomes of the Dresden protocol. They showed that Kapex, Kmin, and Kmax were significantly lower than the baseline measurements, and CDVA was significantly improved. 27
The new accelerated CXL procedure has been used recently to maintain the same amount of energy over a shorter period of time to reduce the treatment time and to increase the comfort of patients. Previous studies have shown the effects of accelerated CXL treatment for progressive keratoconus.19–26,29–31 In this study, the 18-month results of accelerated CXL treatment (18 mW/cm2 for 5 min, total radiant exposure 5.4 J/cm2) were evaluated for progressive keratoconus.
This study found that Kflat, Ksteep, and Kaverage were significantly decreased at 12 and 18 months (P < 0.05), and Kapex was also lower at the 6, 12, and 18-month visits (P < 0.05). Recent studies support our outcomes for accelerated CXL.21–23,30–32 Elbaz et al. reported 1-year outcomes of accelerated CXL (irradiance 9 mW/cm2, 10 min). They showed that Ksteep, Kflat, Kaverage, and Kmax were stable at the 12-month visits. 22 Some studies also compared accelerated and conventional CXL,19,21,23,32 and the results were consistent.
Kanellopoulos evaluated the results of accelerated and conventional CXL procedures in 21 patients with bilateral keratoconus for 46 months. One eye was treated with accelerated CXL (irradiance 7 mW/cm2, 15 min), and the second eye was treated with the conventional procedure. Ksteep was found to decrease from 49.5 to 46.1 D and from 48.7 to 45.8 D in the accelerated and conventional groups, respectively. 23 Sherif found that Kmax was significantly flattened and Kmin was insignificantly reduced in the accelerated group, while Kmin and Kmax were decreased in the conventional group, although not with statistical significance. 21 Tomita et al. and Mazzotta et al. also reported that Kmean decreased 12 months after accelerated CXL.19,32 Ozgurhan et al. showed a statistically significant regression in all keratometric findings (K1, K2, Kmean, and Kapex) at 12 and 24-month visits after accelerated corneal cross-linking in pediatric keratoconus cases. 30
This study shows that UDVA and CDVA improved with statistical significance at 12 and 18 months after treatment compared with baseline measurements (P < 0.05). This study does not report a statistically significant reduction of mean refractive sphere and cylinder at 12 and 18 months. Kanellopoulos and Mazzotta et al. reported that UDVA and BCVA improved in both groups (accelerated-conventional 23 and accelerated-pulse accelerated cross-linking 32 ). Sherif also found improvement in BCVA for both groups 12 months postoperatively. 21 Ozgurhan et al. showed statistically significant improvement in UDVA and CDVA at 12 and 24-month visits in pediatric patients. 30 However, Elbaz et al. showed no statistically significant changes in the mean CDVA, while UDVA increased to statistically significant levels (P: 0.012). 22
Central corneal thickness decreases during the 6 months after CXL treatment and returns to baseline measurements ∼1 year later.30,31,33 In our study, central corneal thickness showed statistically significant reduction at 1 and 6-month visits postoperatively and returned to preoperative values after 12 months, remaining stable thereafter. Kanellopoulos found an increase in corneal thickness values at 18 months following the treatment. 23
Corneal haze commonly occurs after CXL treatment. The severity of corneal haze is correlated with thinner corneas and higher Kmax and Kmean values. 34 Occasionally, complications of CXL treatment include microbial keratitis, sterile infiltrates, endothelial damage, persistent epithelial damage, and corneal edema.35,36 No postoperative complications (persistent haze or infection) were observed in this study.
However, our study has 2 major limitations. The retrospective design and the short follow-up time period are the first limitations of our study. A long-term randomized prospective study is required to focus on the efficacy and safety and report to the final decision of accelerated CXL. The second limitation of our study is absence of a control group. A relative study, which includes a control group, is necessary to compare the results and the comfort of accelerated CXL with standard CXL.
In conclusion, accelerated CXL (irradiance of 18 mW/cm2 for 5 min with a total surface dose of 5.4 J/cm2) seems to be an effective and successful treatment on stabilizing the corneal curvature and halting the progresses of keratoconus over the study period of 18 months of follow-up.
Footnotes
Author Disclosure Statement
No competing financial interests exist.