
Abstract
Purpose:
The present study was performed to investigate the effect of oral dronabinol, a synthetic tetrahydrocannabinol derivate, on retinal hemodynamics in healthy subjects in a randomized, double-masked, placebo-controlled, 2-way crossover design.
Methods:
Twenty-four subjects received 5 mg dronabinol on 1 study day and placebo on the other study day. Total retinal blood flow (TRBF) was measured using a custom-built Doppler Optical Coherence Tomography system. Oxygen saturation of major retinal vessels was measured with a commercially available Dynamic Vessel Analyzer. Based on these parameters, retinal oxygen extraction was calculated. Measurements were performed before and after drug administration on both study days.
Results:
Placebo had no effect on TRBF, retinal arterial or venous oxygen content, and retinal oxygen extraction (P > 0.1 each). In contrast, dronabinol induced a significant increase in TRBF from 38.9 ± 6.1 to 40.7 ± 6.7 μL/min (P < 0.001), which was accompanied by a significant increase in retinal venous oxygen content (from 0.129 ± 0.008 to 0.132 ± 0.009 mL O2/mL, P = 0.02). As no change in retinal arterial oxygen content occurred (P = 0.12), retinal oxygen extraction remained stable (2.2 ± 0.4 μL vs. 2.2 ± 0.4 μL O2/min, P = 0.29).
Conclusions:
These results indicate that orally administered dronabinol increases TRBF in healthy subjects without altering retinal oxygen extraction. The drug may therefore be a candidate for improving perfusion in patients with ocular vascular disease.
Introduction
Tetrahydrocannabinol (THC), the main psychoactive component of cannabis, is known to exert a large variety of biological effects in neural and non-neural tissues. 1 Pharmacologically, THC is a partial agonist of the CB1 and CB2 receptors, both of which are widely expressed in various tissues of the central nervous system, including the human eye.2–4 It has been previously reported that the well-described acute psychoactive effects are mainly mediated through the activation of the CB1 receptor, resulting in euphoria, relaxation, and sensory intensification. 5
Concerning the eye, the most prominent cannabinoid-related effect described is a reduction in intraocular pressure (IOP) mediated through the CB1 receptor, an effect that has been the subject of extensive research, primarily with the purpose of developing effective IOP-lowering therapeutics.6,7 However, the non-IOP-lowering properties of cannabinoid receptor agonists, particularly when using low dosage of the drug has frequently been overlooked. The recent discovery of the endocannabinoid system as a potential drug target in the eye has revisited the interest in non-IOP-related effects of low-dose cannabinoids.8,9
Among these non-IOP effects, the vasoactive properties of cannabinoids deserve particular attention. 10 There is ample evidence that in the brain, the acute intake of THC increases cerebral blood flow.11,12 As the human retina is part of the central nervous system and therefore shares major physiological properties with the brain, it is reasonable to suggest that cannabinoids also exert vasoactive properties in different vascular beds of the eye. Indeed, cannabinoid receptors have been found in and around ocular vessels, indicative of potential blood flow regulating functions.6,13–15 The effect of endogenously administered cannabinoid receptor agonists on ocular blood flow in humans is, however, only insufficiently described.
We have previously shown that low-dose oral administration dronabinol increases optic nerve head blood flow in healthy subjects without exerting psychoactive side effects. 16 In this study, we present data on the effect of single administration of 5 mg dronabinol on retinal blood flow (RBF) and retinal oxygen metabolism in healthy subjects. Dronabinol is currently approved for the treatment of anorexia due to acquired immunodeficiency syndrome or cancer, nausea, and vomiting related to cancer treatment in patients who have failed to respond adequately to other treatments and for pain management.17,18 In the present study, systemic hemodynamics, total retinal blood flow (TRBF), and retinal oxygen saturation were measured before and after administration of the study medication on each study day to investigate the effect of low-dose dronabinol on these parameters.
Methods
Subjects
The present study was conducted in compliance with the Declaration of Helsinki and followed the Good Clinical Practice guidelines of the European Union. The study protocol was approved by the Ethics Committee of the Medical University of Vienna and the national competent authorities. All subjects provided written informed consent before any study-related procedures. The screening examinations, inclusion/exclusion criteria, and study design have been published in a previous report and are only shortly summarized here. 16
In the 4 weeks before the first study day, a screening examination was performed, which included medical history survey; pregnancy test in women of childbearing potential; urine drug test and analysis; alcohol breath test; physical examination, including 12-lead ECG and measurement of systemic hemodynamics, blood draw for hematological status, clinical chemistry, and Hepatitis B, C, and HIV-Serology; a psychiatric examination using the modified Structured Clinical Interview (SCID-1)19,20 test; and a routine ophthalmic examination comprising of assessment of best-corrected visual acuity, slit lamp biomicroscopy, indirect funduscopy, and measurement of IOP.
Subjects were excluded if clinically significant abnormalities were found at the screening examination. Further exclusion criteria were history of drug or alcohol abuse, ametropia of more than 6 diopters, regular use of medication, regular drug intake during the 3 weeks before the start of the study (except contraceptives), and smoking.
Study design
The study design was randomized, double masked, placebo controlled, 2-way crossover. At the beginning of each of the 2 study days, a pregnancy test was performed in females of childbearing potential as well as a urine drug screening and alcohol breath test. Afterward, 1 drop of tropicamide 0.5% was instilled in 1 randomly chosen study eye and a resting period of at least 20 min was scheduled. Afterward, systemic hemodynamics and IOP were measured. Then, measurements of TRBF and retinal oxygen saturation were performed. After measurements were completed, subjects received dronabinol or placebo according to the randomization list. Again, a resting period of 1 h was scheduled and all measurements described above (except pregnancy, drug, and alcohol test) were repeated.
Study medication
Investigational medical product: Capsules containing 5 mg Dronabinol (Bionorica Ethics, Neumarkt, Germany), also referred to as (−)-trans-Δ 9 -THC. Dose: 1 capsule containing 5 mg.
Placebo: Capsules identical in appearance to Dronabinol capsules without an active ingredient. Dose: 1 capsule.
Subjects received the study medication together with a standardized meal containing of 15 g butter, 2 pieces of bread, and 250 mL of water to assure comparable bioavailability. Dronabinol and placebo capsules were produced and provided by Allerheiligen Apotheke, Mag. pharm. Herbert Baldia KG, Allerheiligenplatz 4, 1200 Vienna under GMP conditions.
Methods
Systemic hemodynamics
Systolic blood pressure, diastolic blood pressure, and mean arterial pressure (MAP) were measured by an automated oscillometric device on the upper arm. Pulse rate was recorded from a finger pulse oxymetry device (Infinity Delta; Draeger, Luebeck, Germany).
IOP and ocular perfusion pressure
A slit-lamp-mounted Goldmann applanation tonometer was used for measurement of IOP. To obtain corneal anesthesia, 1 drop of oxybuprocain hydrochloride combined with sodium fluorescein was instilled before each measurement. Ocular perfusion pressure (OPP) was estimated as 2/3 MAP-IOP. 21
Measurement of TRBF
RBF was measured using a custom-built dual-beam Doppler Fourier Domain-Optical Coherence Tomography (OCT) system coupled to a fundus camera, which has been described in detail previously.22–28 Briefly, a specific rectangular scanning pattern around the optic nerve head is used to obtain measurements from all retinal arteries and veins with a diameter of at least 40 μm. 24 The scanning of each vessel group lasts several seconds to allow for averaging of blood velocity values over several pulse periods. Absolute blood velocity is then quantified by measuring phase shifts in the 2 channels and the mean value of the 2 channels is calculated (Vabs). 26 Vessel diameters (d) were also extracted from the phase images and absolute blood flow (Qabs) was calculated as Qabs = Vabs d2 π/4 for each vessel. 29 TRBF in arteries was calculated by summing up all Qabs values for arteries (QAabs) and the same was done for retinal veins (QVabs). TRBF was then calculated as:

Measurement of retinal oxygen extraction
The Doppler OCT system that was used in the present study is coupled to a commercially available Dynamic Vessel analyzer (DVA; Imedos Systems, Jena, Germany). The DVA contains an oxygen module for measurement of retinal oxygen saturation based on 2 fundus photographs taken at different wavelengths of 610 and 545 nm. One photograph is taken at a wavelength of 545 nm that is close to the isosbestic point at 548 nm, at which oxygenated and deoxygenated hemoglobin show identical absorption. The other photograph is taken at 610 nm, where oxygenated hemoglobin is nearly transparent, allowing calculation of oxygen saturation in all retinal arteries and veins.30,31
A mathematical model that has been described in detail previously was used for calculation of oxygen content at the level of the central retinal artery (cO2CRA) and the central retinal vein (cO2CRV). 27 This model takes several factors into account, such as the oxygen loss through the vascular wall between the point of measurement and the center, as well as the fact that not all oxygen is bound to hemoglobin, as there is also free, nonbound oxygen present. Retinal oxygen extraction is then calculated from oxygen content and TRBF as follows:

Data analysis
All outcomes were tested for normal distribution using the Shapiro–Wilk test, which was thereby confirmed. Data are presented as mean ± standard deviation. For systemic hemodynamics, IOP and OPP mean values were calculated and a t-test was used to compare values between groups and study days.
To detect differences in the time and treatment effect of RBF, oxygen content, and oxygen extraction between the dronabinol and the placebo day, a repeated measures ANOVA model was applied. Within this model, predefined planned comparisons were performed to detect differences.
For data description and figures, % changes over baseline were calculated. A P value <0.05 was considered the level of significance. Statistical analysis was carried out using CSS Statistica for Windows® (Version 6.0; Statsoft, Inc., Tulsa, CA).
Results
Twelve female and 12 male healthy subjects between 20 and 35 years of age were included in the present study and completed it according to the protocol. Systemic hemodynamics, IOP and OPP, were similar on the dronabinol and the placebo day before administration of the study medication and neither placebo nor dronabinol had an effect on these parameters (Table 1).
Hemodynamic Parameters on Both Study Days
SBP, DBP, MAP, HR, IOP, and OPP before and after intake of placebo and dronabinol. Values are presented as mean ± SD.
DBP, diastolic blood pressure; HR, heart rate; IOP, intraocular pressure; MAP, mean arterial pressure; OPP, ocular perfusion pressure; SBP, systolic blood pressure; SD, standard deviation.
Administration of placebo had no effect on TRBF (39.0 ± 6.6 μL/min vs. 39.5 ± 6.7 μL/min, P = 0.18, relative change 1.4% ± 4.4%, Fig. 1a). Also, no changes in retinal arterial (0.186 ± 0.010 mL vs. 0.187 ± 0.009 mL O2/mL, P = 0.73 Fig. 1b) or retinal venous oxygen content (0.130 ± 0.008 mL vs. 0.131 ± 0.009 mL O2/mL, P = 0.76 Fig. 1c) were observed after placebo administration. Placebo had no effect on arteriovenous difference in oxygen content (0.056 ± 0.010 mL vs. 0.056 ± 0.009 mL O2/mL, P = 0.97) Thus, calculated retinal oxygen extraction remained stable (2.2 ± 0.5 μL vs. 2.2 ± 0.4 μL O2/min, P = 0.69, Fig. 1d).
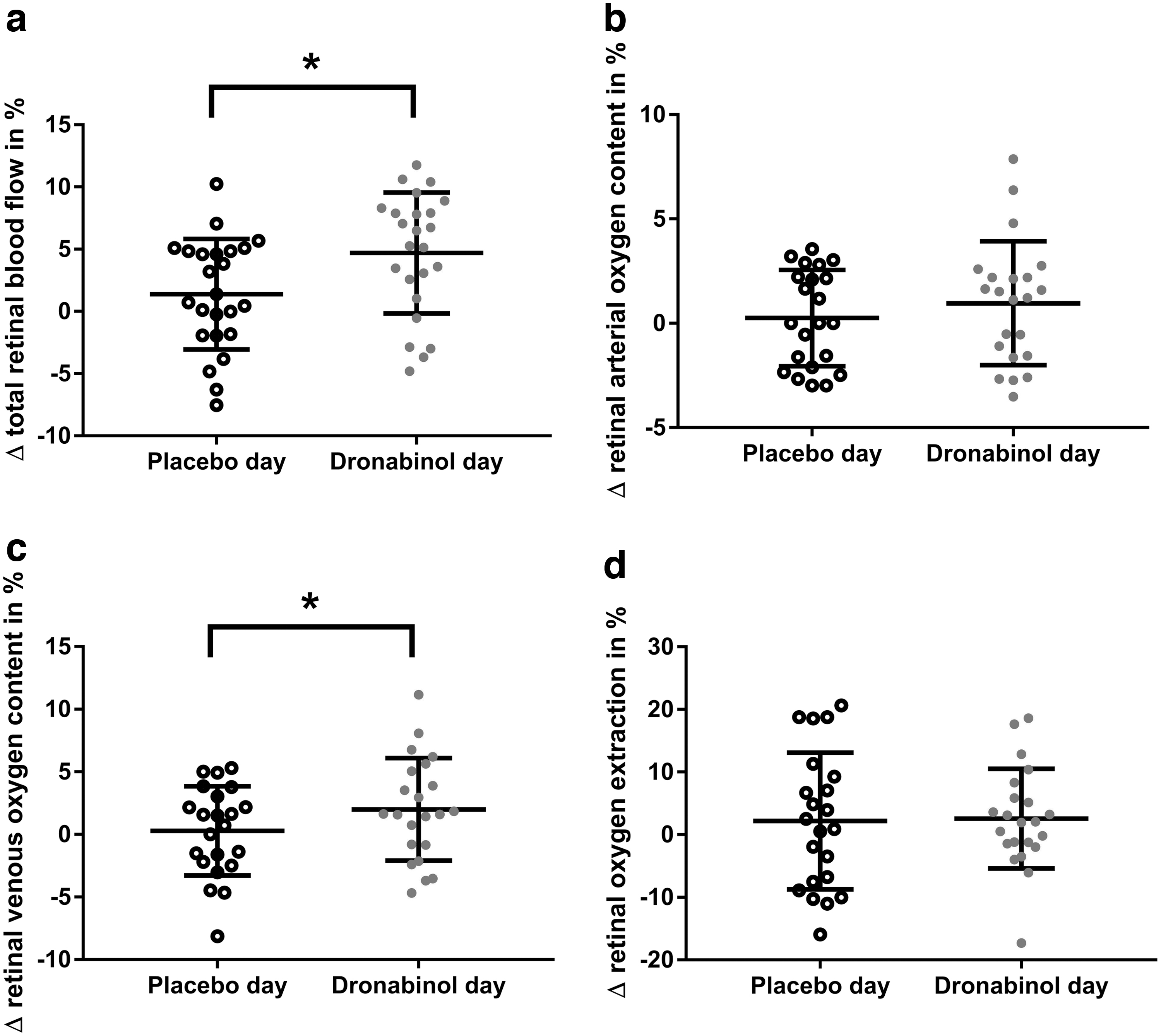
Relative change in total retinal blood flow
After intake of dronabinol, a significant increase in TRBF from 38.9 ± 6.1 to 40.7 ± 6.7 μL/min occurred (P < 0.001, relative increase 4.7% ± 4.9%, Fig. 1a). Retinal arterial oxygen content did not change (0.185 ± 0.009 mL vs. 0.187 ± 0.008 mL O2/mL, P = 0.12, Fig. 1b), while a significant increase in retinal venous oxygen content from 0.129 ± 0.008 to 0.132 ± 0.009 mL O2/mL (P = 0.02, Fig. 1c) was observed, leading to a slight numerical decrease in arteriovenous oxygen content difference (0.056 ± 0.008 mL vs. 0.055 ± 0.009 mL O2/mL, P = 0.51). Oxygen extraction did not change after intake of dronabinol (2.2 ± 0.4 μL vs. 2.2 ± 0.4 μL O2/min, P = 0.29, Fig. 1d). All relative changes are shown in Fig. 1.
The time versus treatment effect in TRBF was significantly different between the placebo and the dronabinol day (ANOVA, P = 0.01). In contrast, no difference between the placebo or dronabinol day was seen in retinal arterial or venous oxygen content (ANOVA P = 0.38 for arteries and P = 0.15 for veins), arteriovenous oxygen content difference (ANOVA P = 0.62) or retinal oxygen extraction (P = 0.64).
The study medication was well tolerated and no treatment-emerged adverse events or serious adverse events occurred during the course of the study.
Discussion
Our study shows that oral intake of 5 mg dronabinol induces a significant increase in TRBF without altering retinal oxygen extraction in healthy volunteers. Furthermore, no psychoactive effects, effects on IOP, or systemic hemodynamics were observed at the selected dose as reported previously. 16 This indicates that exogenous administration of a cannabinoid receptor agonist exerts vasoactive properties at the level of the retina and increases RBF in healthy subjects without altering OPP.
It is well known that acute exposure to cannabinoids, that is, by marihuana smoking, is associated with a drop in systemic blood pressure and an increase in heart rate, both of which indicate peripheral vasodilatation. 32 Although it was originally thought that this effect is caused by a centrally mediated mechanism, there is increasing evidence that cannabinoid receptors are directly involved in the regulation of vascular tone. 33 Previous studies from feline isolated cerebral arteries show that CB1 receptor agonists lead to concentration-dependent relaxation of cerebral arteries, most probably by modulating the influx of Ca2+. 34 Along this line of thought, data from the human studies show an increase in cerebral blood flow after THC exposure, which parallels plasma THC levels.11,12 However, the most of latter studies are limited by the fact that THC levels were increased by inhaling or oral ingestion of THC-containing food preparations, which does not allow for exact dosing. 35
More recent evidence supports the hypothesis that cannabinoids also exert vasoactive properties in the level of the eye. We have previously reported that low-dose exposure to dronabinol, a synthetic THC derivate, which can be administered orally, increases optic nerve head blood flow in the range of 10%. 16 In this study, we extend these recent findings by showing that administration of the cannabinoid receptor agonist dronabinol also increases RBF in healthy subjects. Although, to the best of our knowledge, this is the first study to measure the effects of cannabinoids on volumetric RBF, our finding is in keeping with previously published reports on the effect of THC and its derivatives on the ocular vasculature. As such, administration of exogenous administered THC leads to vasodilatation of conjunctival vessels, which is reflected in the clinical appearance of redness of the eye. 35 However, the latter effect is limited to high exposure and major intoxication with THC plasma levels of 5 ng/mL or more. 35 Furthermore, a previous study has investigated potential associations between cannabis use and retinal vessel diameter in young adults. The authors of the latter study report that subjects that have used cannabis in the 24 h before the assessments show wider retinal arteriolar diameters when compared with age-matched control subjects, which also indicates a retinal vasodilator effect of cannabinoids. 36 Additionally, Plange et al. 37 showed in a previous experiment that the retinal arteriovenous passage time, a measure of RBF velocity, decreased after administration of 7.5 mg dronabinol. Although the latter study does not allow for drawing conclusions on volumetric blood flow as it was measured in the current experiment, the results of Plange et al. are in keeping with the hypothesis that cannabinoids exert retinal vasodilatation. 37
As part of this study, oxygen extraction was calculated based on TRBF and oxygen saturation in retinal vessels as measured using a fundus camera-based, reflectometric method.22,24,27,28,30
The results of our study show that tissue oxygen extraction and retinal arterial oxygen saturation remained constant during the study period, whereas venous oxygen saturation increased after administration of dronabinol. These data are consistent with our other findings and can be explained as follows: Venous oxygen saturation is dependent on both RBF and tissue oxygen extraction. Thus, it is reasonable to expect that an increase in blood flow as observed after administration of dronabinol, leads to an increase in venous oxygen saturation if the oxygen demand of the tissue stays constant. Indeed, our data show that the increase in blood flow is paralleled by an increase in venous oxygen content and a numerical decrease in arteriovenous oxygen content difference, resulting in unchanged oxygen extraction. This strongly indicates that the increase in venous oxygen content is caused by an increase in blood flow and not by a change in oxygen metabolism in the retina.
Although our results as well as previous reports consistently indicate that exogenous administration of cannabinoid receptor agonists exert vasodilator effects in different vascular beds of the eye,16,37 the molecular mechanisms mediating this effect warrants further investigation. It has been hypothesized that the vasodilator effect is caused by activation of CB1 receptors leading to vasodilatation mediated through the nitric oxide as well as the endothelin system.14,38 Although both systems have been found to play a major role in the regulation of blood flow in the eye39–41 an experimental proof of this hypothesis is still missing.
Interestingly, no effect of dronabinol on IOP was observed in the current study. This is in contrast to previously published data in the literature, where a decrease in IOP was reported after administration of THC.37,42–44 Similarly, no cannabinoid-induced tachycardia was detected as observed in other studies.45,46 The reason for these differences is not entirely clear but could be related to the higher drug concentrations 37 or the different application methods43,44 used in previous trials. In this context, it also needs to be considered that most previous studies included glaucoma or ocular hypertensive patients with elevated IOP. Thus, one could speculate that a potential IOP-lowering effect of dronabinol is more pronounced in this population than in healthy subjects as included in the present study.42,43
Our study has several strengths. In particular, the current study takes advantage of a recently introduced custom-built Doppler OCT system, which allows for the assessment of TRBF with high precision and excellent reproducibility. 26 Furthermore, the current study was performed in a double-masked, randomized, placebo-controlled 2-way crossover design, where every subject served as its own control. This reduces the influence of confounding covariates and increases statistically robustness, which makes it a gold standard for interventional studies.
The current study also has some limitations, which need to be considered when interpreting our results. Because of technical limitations, RBF as well as oxygen saturation can only be measured in retinal vessels with a diameter of 40 μm or larger. Therefore, only indirect conclusions can be drawn on the effect of dronabinol on small arterioles or the retinal microcirculation. Technologies such as OCT angiography systems may provide data on retinal microcirculation, but no quantification of perfusion is possible.47,48 Furthermore, dronabinol was only administered once. Thus, we do not know the effects of chronic low-dose therapy with cannabinoid receptor agonists. As the data on both retinal and optic nerve head blood flow are promising, further studies are needed to investigate the effect of long-term administration of dronabinol. Finally, because of feasibility reasons, measurements were only performed at baseline and once after drug administration. Thus, no conclusions can be drawn in respect to the time course of the blood flow changes.
In conclusion, the present results indicate that orally administered low-dose dronabinol increases TRBF in healthy subjects without altering retinal oxygen extraction. The drug may therefore be a candidate for improving perfusion in patients with ocular vascular disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for the present study.