
Abstract
Abstract
Background:
Acupressure is a widely used adjunct for various symptoms in patients with nonchronic kidney disease. However, its role for symptom management in end-stage renal disease (ESRD) populations is not clear.
Objective:
To summarize and critically evaluate the evidence available from randomized clinical trials (RCTs) of acupressure for patients with ESRD.
Design:
Systematic review of RCTs.
Methods:
Thirteen databases were searched from their inceptions through December 2009, irrespective of publication status or language.
Results:
In total, 7 RCTs out of 86 screened studies were included and analyzed. Most studies lacked sufficient description to gauge the quality of the RCT. Acupressure was not superior to sham acupressure (n = 2) or to transcutaneous electrical stimulation (n = 1), while studies suggested benefits of acupressure compared to usual care (n = 3), sleep medication (n = 1), and undefined control intervention (n = 1). None of these studies reported any adverse events.
Conclusion:
No definitive conclusion is available. Future trials should adhere to standards of trial methodology and explicitly report relevant information for evaluation of efficacy and safety of acupressure in patients with ESRD.
Introduction
Acupressure is a specific method of stimulating acupuncture points by pressing or tracking on the acupoints or the meridians using hands and fingers. 5 It can also be classified as a subtype of therapeutic massage. 6 The key characteristic of acupressure that differentiates it from other types of massage is its basis in the theory of Oriental medicine, especially acupuncture and meridian theory. 5
Acupressure is often delivered as an adjuvant component of complex cancer care 7 and for managing chronic pain. 8 It has been suggested as a potential adjunctive therapeutic modality for kidney diseases. 9 However, its effectiveness has not been systematically analyzed in patients with ESRD. Hence, the aim of this systematic review is to summarize and critically evaluate the evidence for the effectiveness of acupressure as supportive care in patients with ESRD.
Methods
Search strategy
Thirteen electronic databases were searched from their inception through December 2009. The databases were Medline, PsycInfo, Alternative Medicine (AMED), Cumulative Index to Nursing & Allied Health Literature (CINAHL), EMBASE, The Cochrane Library 2009 (Issue 4), six Korean databases (Korean Studies Information, DBPIA, Korea Institute of Science and Technology Information, Research Information Center for Health Database, KoreaMed, National Assembly Library), and a Chinese database (CNKI). The search string used was “(acupressure OR massage OR shiatsu OR shiatzu) AND (dialysis OR hemodialysis OR end stage renal disease OR chronic kidney disease OR chronic renal disease OR chronic renal failure OR peritoneal dialysis).” We also manually searched our own retained files, supplements, and relevant journals (FACT [Focus on Alternative and Complementary Therapies] and Research in Complementary Medicine [Forschende Komplementarmedizin]) from their inception date to December 2009. In addition, the references of all located articles and our retained files were hand-searched for additional related articles.
Selection criteria
Randomized controlled trials (RCTs) of any type of acupressure for patients with ESRD, except transplant recipients, were included. Trials that employed acupressure as the sole treatment or as an adjunct to other conventional treatments were included. Trials that used acupressure as an adjunct to other treatments with unproven effectiveness were excluded. If a shiatsu trial used manual stimulation of meridian and acupoints, that trial was included. No language restrictions were imposed. Dissertations and abstracts were included if they contained sufficient detail for critical evaluation. Hard copies of all articles were obtained.
Data extraction, quality, and validity assessment
All articles were read by two independent reviewers (K.K.H. and M.S.L.), who extracted data from the articles according to predefined selection criteria (Table 1). Risk of bias was assessed using the Cochrane classification in four criteria: randomization, blinding, withdrawals, and allocation concealment. 10 According to the Cochrane collaboration's tool for assessing risk of bias, a judgment of “Yes” indicating low risk of bias, “No” indicating high risk of bias, or “Unclear” indicating unclear or unknown risk of bias was determined per each criterion. 10 Given the impossibility of blinding acupressure practitioners, patient and assessor blinding were examined separately. Assessor blinding was admitted when the outcome was measured by another person (not the patient himself ) who did not know the group assignment. Disagreements were resolved by discussion between the two reviewers (K.K.H. and M.S.L.). Between the two reviewers, there was no disagreement about risk of bias.
Risk of bias (randomization, randomization method, drop-out or withdrawal, patient blind, assessor blind, allocation concealment); Y, “Yes”(low risk of bias); N, “No”(high risk of bias); U: “Unclear” (uncertain risk of bias).
HD, hemodialysis; PD, peritoneal dialysis; ESRD, end-stage renal disease; AP, acupressure; n.r., not reported; NS, not significant; TEAS, transcutaneous electrical acupoint stimulation; UP, uremic pruritus; PSQI, Pittsburgh Sleep Quality Index; PFS, Piper Fatigue Scale; VAS, Visual Analogue Scale; BDI, Beck Depression Inventory; PCS, physical component scale; MCS, mental component scale; RLP, role limitation physical; RLE, role limitation emotional; BP, body pain; VT, vitality; SF, social functioning; TCM, traditional Chinese medicine.
The precision of the acupoint was confirmed if the subjects' treatment area felt sore, numb, heavy, distended, and/or warm during the acupoint massage.
Manual refers to “manual acupuncture using hand and fingers”.
Investigators and research assistants were trained by Chinese medicine physicians.
The rate of treatment responders among each group.
Results
Study description
Of the total of 86 studies initially identified, 79 studies had to be excluded (Fig. 1), leaving seven RCTs that met our inclusion criteria. The key data from all included RCTs are summarized in Table 1.11–17 Four RCTs were conducted in Taiwan, two RCTs originated in China, and one was from Poland. Participants in included studies were patients with ESRD experiencing sleep disorder, muscle cramps, uremic pruritus, fatigue, or depression. Acupressure was compared to the following interventions: (1) sham acupressure and usual care in two studies,14,15 (2) usual care in two studies,11,17 (3) transcutaneous electrical acupoint stimulation (TEAS) and usual care in one study, 13 and (4) sleep medication in one study. 12 One study mentioned that acupressure was compared to a control group, but the group was not described in detail. 16 The follow-up period ranged from 4 to 18 weeks from the baseline in six RCTs,11–16 while one RCT observed the immediate effect of acupressure without any follow-up. 17 Five RCTs11,13–15,17 included symptomatic hemodialysis patients and one RCT included both hemodialysis and peritoneal dialysis patients. 16 One RCT did not mentioned dialysis modality in detail (hemodialysis or peritoneal dialysis). 12
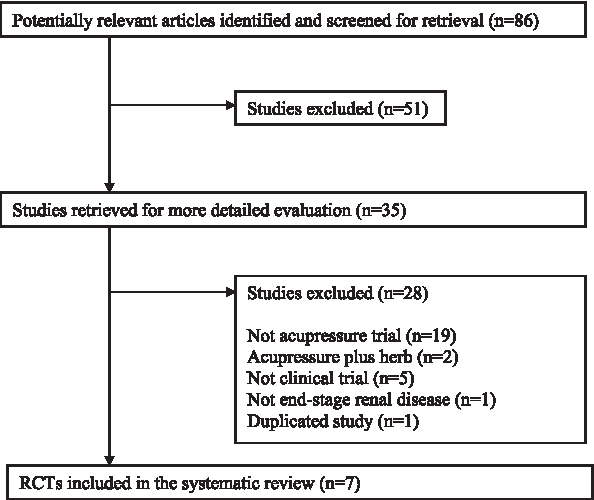
Flow chart of trial selection process. RCT, randomized clinical trial.
Study quality
None of the seven included studies mentioned the method of randomization or used allocation concealment. Only one RCT reported patient and assessor blinding. 14 Drop-outs and withdrawals were described in three RCTs.11,13,14
Acupressure type
All of the included RCTs used acupressure with hands and fingers. Sham acupressure was defined as pressing non-acupoints 1 cm near the real treatment point with the same frequency and time in two RCTs.14,15 None of the two sham acupressure–controlled RCTs mentioned the intensity of sham acupressure.
Acupressure procedure
Acupressure was performed immediately before or after dialysis in one study, 16 upon symptom occurrence during dialysis in one study, 17 and during the dialysis in two studies.11,14 Three studies did not report the time of treatment administration.12,13,15 Acupressure was conducted on the whole body in one study, 16 on the four acupuncture points of lower extremities in five studies,11–13,15,17 and on two acupuncture points and one auricular acupuncture point in one study. 14 Efforts to build internal validity and reliability of acupressure by achieving consistent intensity of massage pressure and obtaining accurate location of acupressure were reported in four RCTs.11,13–15 Five of seven studies reported information on the acupressure practitioners, who were experienced Mongolian doctors or investigators trained by traditional Chinese medicine physicians.11,13–16
Outcomes
Sleep disorder
Tsay et al. 14 conducted an RCT employing acupressure, sham acupressure, and usual care for 105 hemodialysis patients. In the acupressure group, the mean Pittsburgh Sleep Quality Index (PSQI) score, four components of the PSQI subscale (subjective sleep quality, sleep duration, habitual sleep efficiency, and sleep sufficiency), awake time, and quality of sleep at night obtained from a daily sleep log were significantly improved compared to the usual care group, but not when compared to the sham acupressure group. No difference was observed between the acupressure and sham acupressure group in quality of life, measured by the SF-36 questionnaire. The same researcher also performed an RCT employing acupressure, TEAS, and routine care (not described in detail) for 108 hemodialysis patients. 13 In both the acupressure and TEAS group, sleep quality measured by PSQI was significantly improved compared to the routine care group. No differences were found between the acupressure and the TEAS groups. Dai et al. 12 conducted an RCT of 82 ESRD patients, comparing acupressure to conventional medication (oral intake of 1 mg of estazolam tablets half an hour before sleep). Subjective sleep quality of life and rate of sleep disturbance-related disorders (headache, dizziness, amnesia, and palpitation) were significantly better in the acupressure group than in the medication group.
Muscle cramps
Zhu et al. 17 found that acupressure plus conventional management of leg cramps, including stopping ultrafiltration and providing hypertonic solution, significantly decreased the duration of leg cramps compared to conventional management alone, in an RCT of 44 hemodialysis patients.
Uremic pruritus
Jedras et al. 16 showed that acupressure significantly decreased pruritic symptoms at 6, 12, and 18 weeks after baseline, compared to a control group (not described in detail) in an RCT of 60 dialysis-dependent patients. Most relief was gained at 6 weeks after baseline and was maintained up to the last follow-up.
Fatigue and depression
Tsay 15 reported a significant difference in fatigue between an acupressure group and a usual care group (not described in detail), measured by the revised Piper Fatigue Scale (PFS), visual analogue scale (VAS) of fatigue, and predialysis fatigue. No differences between the acupressure group and a sham acupressure group were observed. PSQI and Beck Depression Inventory (BDI) were also measured; however, only post-treatment values were reported and none of these was analyzed. Tsay et al. 13 conducted an RCT of 108 hemodialysis patients, comparing acupressure to TEAS or routine care (not described in detail). The acupressure group showed no significant differences compared to the TEAS group, but significant differences were observed in both the acupressure and the TEAS group compared to routine care group in fatigue, sleep quality, and questionnaire-screened depression.
Cho and Tsay 11 conducted an RCT that involved 62 hemodialysis patients. Fatigue and depression, measured by revised PFS and BDI, were significantly improved in the acupressure group but no difference was found in the control group receiving routine unit care (not described in detail).
Adverse events
None of the seven RCTs reported whether any adverse events had occurred.
Discussion
Few well-designed trials have tested the benefits of acupressure for ESRD. Real acupressure failed to show specific effects compared to sham acupressure14,15 and TEAS, 13 although it was superior to usual care11,13–15,17 or sleep medication. 12 Target symptoms of acupressure ranged widely, including uremic pruritus, sleep disorder, muscle cramps, fatigue, and depression, all of which are commonly encountered clinical problems accompanying ESRD. In the context of the heterogeneity of the treated conditions, the included RCTs per each condition are relatively too few to assess the benefits of acupressure. Sample sizes were not based on appropriate power calculation in six of seven RCTs.12–17 Randomization methods, such as using random number tables generated by a computer, were not described in any of the seven RCTs. There were no reports of patient or assessor blinding,11–13,15–17 and there was a lack of description about drop-out and withdrawal,12,15–17 which also increases the risk of bias in the included RCTs. None of the seven RCTs, especially three studies that reported drop-out and withdrawal,11,13,14 noted whether intention-to-treat analysis had been conducted. Thus, potential effects of any missing responses could not be excluded. 18 The use of subjective outcome measures, which have not established reliability and validity in two RCTs, inevitably tends to generate bias to some degree.16,17 Paucity of reporting adverse events prevents assessment of the safety of acupressure for ESRD patients. Due to the mentioned methodological flaws above, no definitive conclusion can be drawn from the included RCTs, although these studies may have certain value as preliminary research for conducting rigorous clinical trials.
Future clinical trials should consider accurate estimation of sample size based on proper power calculation, 19 adequate implementation and detailed report of allocation concealment and randomization, 20 patient and assessor blinding,21,22 and the use of objective outcomes, whenever available, or at least of validated outcomes, 23 and should clarify and conduct the intention-to-treat analysis 18 and assess success of blinding at the end of trials 22 in order to improve quality of trials and to minimize potential bias.
Systematic reviews not only summarize existing evidence but also inform and guide future trials. 24 Thus, two major issues, namely the sham-control procedure and the safety of acupressure in ESRD patients, need to be discussed for clearer design and implementation of future acupressure trials.
First, pressing non-acupoints 1 cm away from the exact acupoint or meridian, which was used as sham acupressure in two included studies in our review,14,15 might not be inert. Simple touching has shown therapeutic effects to some degree in other RCTs. 25 The same issue has been increasingly raised in acupuncture research, with the argument that minimal or standard penetration of a non-acupuncture point or invalid point also produces certain physiological and psychological effects. 26 It is also unclear whether the intensity of pressure was controlled in the sham group in two included trials.14,15 It would be logical that sham acupressure should be applied below the pain-threshold thus not generate a “de-qi” response, which is a signal of therapeutic activation of acupoint stimulation. 27 Moreover, none of included RCTs mentioned whether they controlled possible patient–practitioner relationships during manually stimulated finger acupressure procedure. Therefore, no information is available to identify whether nonspecific effects generated by potential patient–practitioner interaction influenced any of the study results. Complex nonpharmacologic interventions, including psychological treatment, acupuncture, some types of physical therapy, and probably finger acupressure, are likely to produce some of their therapeutic effects by counseling and running diagnostic processes during treatment, which is sometimes integral to a certain system of medicine, i.e., asking patients how they feel and optimally adjusting treatment protocol according to how they respond. 31 Although the included sham-controlled RCTs had standardized the pressing intensity and had fixed acupressure points in the treatment group, whether communications between patients and practitioners were allowed was not clearly reported. Thus, the possibility of nonspecific effects related to therapeutic relationships could not be excluded. Given these criticisms, future trials should consider and explicitly describe the optimal sham acupressure, the degree of intensity of sham acupressure, and extent of patient–practitioner interaction in order to build an adequate control procedure and to provide a clear understanding of study results.
Second, information such as time of acupressure administration and practitioner qualifications, which may be related to the accurate assessment of the safety of acupressure, were not clearly reported in some included trials.12–15,17 Patients usually undergo hemodialysis anticoagulation to prevent thrombo-embolic events during hemodialysis. 28 If acupressure is conducted during hemodialysis and some acupoints are overpressed, unexpected subcutaneous or hypodermal bleeding could be induced, which may be regarded as a minor, but undesirable, adverse event. Acupoint stimulation has been suggested to increase parasympathetic nerve stimulation, but little is known whether these kinds of effects generated by acupressure during hemodialysis might be beneficial or harmful. 29 Some patients could feel extremely drained after hemodialysis, which is sometimes a contraindication for acupoint stimulation, according to traditional acupuncture theory. The qualifications of the acupressure practitioner were also not reported in some included trials.12,17 A qualified practitioner seems to produce few serious adverse events during acupuncture or massage.30,31 Of course, acupressure is a noninvasive technique and could sometimes be conducted by both professional and nonprofessional health-care providers, such as the patients themselves, family members, or caregivers. However, proper instruction or education is still needed for safe implementation of acupressure because patients with ESRD are at increased risk of adverse events of acupressure compared to the general population. For example, uremic or diabetic peripheral neuropathy could lessen patients' perception of pain or pressure. If the practitioner determines pressure intensity only by the patient's response, then tissue or nerve injuries caused by overpressure might occur. 30 Xerosis, caused by chronic uremic state, is a frequent phenomenon in patients with ESRD and dry skin could be easily damaged by iterative pressure and tracking. 32 When acupressure is performed for patients infected with hepatitis C, practitioners should be aware of this and should perform acupressure without contacting wounds or ulcers, to avoid being infected with the virus. Pressing an acupoint on or near an arteriovenous fistula should be avoided to prevent traumatic injury. Concerning these issues, the occurrence of adverse events should be carefully observed and reported when conducting acupressure during or after hemodialysis, even though previous studies employing acupuncture or acupoint injection studies have reported no serious adverse events of intervention during or after dialysis.33,34 To avoid and minimize potential risks of adverse events, acupressure should perhaps be conducted on an interdialytic day or before hemodialyis access. Screening of dialysis efficiency by calculating Kt/V (fractional urea clearance, which can be interpreted as the dialysis dose) 35 or related biological parameters might be required for setting clear eligibility, detecting underlying causes of perceived symptoms, and preventing anyunexpected intradialytic symptoms or diminished medical outcomes, which should be distinguished from acupressure-responsible adverse events. Reporting the qualifications of the practitioner and clarifying adequate instructions regarding acupressure when conducted by nonmedical professionals should be routinely encouraged for accurate assessment of safety and effectiveness in future clinical trials.
Limitations in this review should be noted. We found no acupressure study for patients undergoing peritoneal dialysis except one, 16 despite our efforts to locate the whole range of ESRD conditions. Thus, the effects of acupressure on peritoneal dialysis patients remain unknown. The longest reported follow-up period was 18 weeks from baseline, although the benefit of acupressure is sustained for 6 months in patients without ESRD. 8 Consequently, we cannot determine whether acupressure has long-term effects on various symptoms in patients with ESRD. Heterogeneity of the included studies that treated different symptoms should also be mentioned. Since most studies were conducted in China and Taiwan, where cultural familiarity with acupressure is theoretically based on traditional Chinese medicine, findings may not have external validity and may not be reproducible in patients with different cultures and lifestyles. 36
Conclusion
We could not draw any definitive conclusions that acupressure as a supportive care is beneficial for ESRD patients who experience fatigue, depression, sleep disturbance, uremic pruritus, or muscle cramps. The small number and suboptimal methodological quality of currently available RCT reports are major obstacles in determining the therapeutic effects of acupressure for ESRD patients. The overall safety of acupressure for patients with ESRD could not be assessed due to poor reporting of adverse events. Future well-designed clinical trials are required to evaluate whether acupressure has clinical benefits for this condition.
Footnotes
Acknowledgments
This study was supported by the Development of Acupuncture, Moxibustion, and Meridian Standard Health Technology Project (K 10010) of the Korea Institute of Oriental Medicine.
Author Disclosure Statement
No competing financial interests exist.